
Translate this page into:
Evaluation of SD BIOLINE Syphilis 3.0 for Rapid Diagnosis of Syphilis: Report from a Regional Sexually Transmitted Infection Reference Laboratory in North India
Address for correspondence: Dr. Preena Bhalla, E-mail: preenabhalla@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Serology is considered the mainstay of syphilis diagnosis. The limitations of the traditional serological methods and the advent and availability of novel immunochromatographic assays have led to the widespread application of rapid point-of-care procedures as screening tools for syphilis. However, these tests have not been extensively evaluated. This study was designed to evaluate the performance of a rapid syphilis diagnostic test known as SD BIOLINE Syphilis 3.0 (SD Biostandard Diagnostics Private Limited, Gurgaon, Haryana, India).
Materials and Methods:
A panel comprising of 50 venereal disease research laboratory reactive and 50 nonreactive sera was tested using SD BIOLINE Syphilis 3.0. The performance of the test was evaluated using IMMUTREP Treponema pallidum hemagglutination assay (TPHA) (OMEGA Diagnostics Limited, Scotland, United Kingdom) as the reference standard and sensitivity, specificity, and negative and positive predictive values were calculated.
Results:
The sensitivity, specificity, and positive and negative predictive values of SD BIOLINE Syphilis 3.0 were 92.86% (confidence interval of 95%: 80.52–98.50%), 98.28% (90.76-99.96%), 97.50% (86.84–99.94%), and 95.00% (86.08–98.96%), respectively, compared to TPHA as the gold standard.
Conclusion:
Keeping in view the high sensitivity and specificity of SD BIOLINE Syphilis 3.0, we conclude that the test can be used as a tool for rapid on-site diagnosis of syphilis and as an alternative to TPHA for detection of antibodies to Treponema pallidum.
Keywords
Non-treponemal tests
rapid
serodiagnosis
syphilis
treponemal tests

INTRODUCTION
Syphilis is a sexually transmitted infection (STI) caused by the bacterium Treponema pallidum (T. pallidum). It is a common STI in India.[12] The inability to culture the causative organism in vitro and the limited availability of nucleic acid amplification techniques makes the diagnosis of this infection difficult. Moreover, direct visualization of the organism does not seem to be feasible since it mandates the presence of lesions and of facilities with either dark field or fluorescent microscopy.[3] Serology is thus considered the mainstay of syphilis diagnosis.
Serodiagnosis of syphilis relies on detection of two types of antibodies-antibodies against the cardiolipin antigen, and the treponema-specific antibodies.[45] A major diagnostic limitation encountered with the use of anticardiolipin antibody-based tests (nontreponemal tests) is the occurrence of biological false positive (BFP) reactions.[678] It is, therefore, recommended to use nontreponemal tests such as venereal disease research laboratory (VDRL) and rapid plasma reagin (RPR) test as screening assays followed by confirmation of the nontreponemal reactivity by the more specific treponemal tests like T. pallidum hemagglutination assay (TPHA) and fluorescent treponemal antibody absorption test.[91011] False negative reactions due to the prozone phenomenon are also seen with nontreponemal tests.[12] Moreover, the tests lack sensitivity in the late latent stage of infection.[13]
A major drawback of the laboratory procedures currently in use for syphilis serodiagnosis is that they require laboratory facilities (refrigeration, water bath, centrifuge, rotator, etc.); stringent quality control measures and skilled persons to perform the tests, as well as trained health professionals to read and interpret the results. In resource constraint settings, laboratory infrastructure and facilities for syphilis diagnosis might not be widely available, and the delay encountered in getting the samples tested from referral laboratories may preclude timely initiation of treatment. This eventually translates into continued transmission of disease to the naive or uninfected individuals.
The current situation mandates the need for rapid and reliable tests to serve as screening and confirming assays in all stages of syphilis. Rapid serological procedures offer a potential option with assured rapid availability of results usually in <15 min and ease of use by health professionals allowing on-site testing. The World Health Organization Sexually Transmitted Diseases Diagnostic Initiative has laid down the ASSURED criteria that define the ideal characteristics of a rapid and point-of-care test: Affordable, sensitive, specific, user-friendly, rapid and robust, equipment free, and deliverable to those who need them.[141516] Several rapid, point-of-care assays based on recombinant T. pallidum antigens are now commercially available.[17] Despite the benefits that the rapid tests offer over traditional laboratory methods for syphilis serodiagnosis, their diagnostic performance remains a matter of concern and is still not widely documented.
In this study, the authors have evaluated the performance of SD BIOLINE Syphilis 3.0 (SD Biostandard Diagnostics Private Limited, Gurgaon, Haryana, India), a rapid immunochromatographic assay that qualitatively detects antibodies against T. pallidum. To the best of our knowledge, there is no published peer-reviewed article in medical literature regarding the evaluation of this test kit in an Indian scenario.
MATERIALS AND METHODS
This prospective study was conducted at the Department of Microbiology of a tertiary care health facility in New Delhi. The study was duly approved by the Institutional Review Board. The serology laboratory of the department receives on an average 15,000 serum samples annually for syphilis serology from both the Inpatient and Outpatient Departments of the linked hospitals. Consecutive blood samples received at the serology laboratory from October 2013 to February 2014 with request for syphilis screening were included in the analysis. On arrival in the laboratory, the samples were allowed to coagulate and centrifuged at 2500 rpm (rotations per minute) for 10 min. The sera were separated and stored at 2–8°C till VDRL (employing antigen from Serologist to Government of India, Kolkata) was put up (generally every 2nd or 3rd day). All VDRL reactive sera were serially diluted to determine the antibody titre. After being tested as per the above protocol, the sera were aliquoted and stored in eppendorfs at − 20°C until a panel of 100 sera comprising of 50 VDRL reactive and 50 nonreactive samples were reached. A different technician who did not have access to results of the screening assay, performed the IMMUTREP TPHA (OMEGA Diagnostics Limited, Scotland, United Kingdom) as per the manufacturer's instructions in the kit insert. The third laboratory technician, who was again blinded to the VDRL and IMMUTREP TPHA results performed SD BIOLINE Syphilis 3.0 in accordance with the manufacturer's guidelines. The procedural details of the tests employed in this study along with their interpretative criteria are provided in Table 1 while their characteristics are summarized in Table 2.


The results of VDRL test, IMMUTREP TPHA, and SD BIOLINE Syphilis 3.0 were entered in Microsoft Excel sheet and any discordant results by IMMUTREP TPHA and SD BIOLINE Syphilis 3.0 were tested again by both the procedures before they were finally recorded as positive or negative. The sensitivity and specificity calculations and estimation of negative and positive predictive values of SD BIOLINE Syphilis 3.0 were done by comparing its performance with IMMUTREP TPHA (reference technique). These values were calculated with their respective confidence interval of 95% (95% CI). Sensitivity was calculated as true positives/(true positives + false negatives) ×100; specificity as true negatives/(true negatives + false positives) ×100; negative predictive value as true negatives/(true negatives + false negatives) ×100, and positive predictive value as true positives/(true positives + false positives) ×100.
RESULTS
Of the 50 VDRL reactive samples, 42 (84%) were TPHA positive, and 40 (80%) were reactive with SD BIOLINE Syphilis 3.0. Considering TPHA as the gold standard, the 8 VDRL reactive and TPHA negative samples can be considered as BFPs. All but one of these 8 BFP samples was correctly identified as negative by SD BIOLINE Syphilis 3.0. In addition, of the 42 true positives picked up by IMMUTREP TPHA, 3 were wrongly identified as negative by SD BIOLINE Syphilis 3.0 and remained so on repeat testing. Two of the samples with false-negative rapid test results had a VDRL titre of 1:2, and one sample had a VDRL titre of 1:16. All the VDRL nonreactive sera (n = 50) were negative by both IMMUTREP TPHA and the rapid test. The performance of SD BIOLINE Syphilis 3.0 and VDRL as against IMMUTREP TPHA is presented in Tables 3 and 4, respectively.
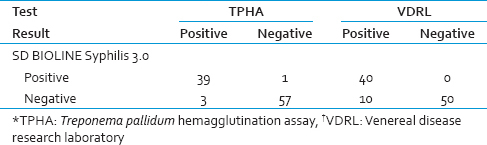

Compared to IMMUTREP TPHA as the gold standard, the sensitivity, specificity, and positive and negative predictive values of SD BIOLINE Syphilis 3.0 were 92.86% (95% CI: 80.52–98.50%), 98.28% (90.76–99.96%), 97.50% (86.84–99.94%), and 95.00% (86.08–98.96%), respectively. The kappa value was 0.917, showing a “very good” strength of agreement between the two tests. The performance characteristics of the currently employed VDRL test in comparison to the gold standard (IMMUTREP TPHA) are as follows: Sensitivity = 100.00% (91.59–100.00%), specificity = 86.21% (74.62–93.85%), positive predictive value = 84.00% (70.89–92.83%), and negative predictive value = 100.00% (92.89–100.00%). Thus, while the sensitivity of SD BIOLINE Syphilis 3.0 was lower than that of VDRL (92.86% vs. 100.00%), the specificity was much higher (98.28% vs. 86.21%).
DISCUSSION
We report sensitivity and specificity values of 92.86% and 98.28%, respectively, for SD BIOLINE Syphilis 3.0, compared to TPHA as the reference standard. A study conducted in Tanzania found the test to be 79% sensitive and 96% specific.[18] In another study conducted in China, the reported sensitivity and specificity values were 95.5% and 97.9%, respectively.[19] Thus, keeping in view the high sensitivity and specificity of SD BIOLINE Syphilis 3.0, we conclude that the test can be used both as a screening assay and as an alternative to TPHA for detection of antibodies to T. pallidum. We found SD BIOLINE Syphilis 3.0 to be less sensitive but more specific than VDRL. Lower sensitivity of immunochromatographic tests has also been reported in previous studies, and the reason cited has been primarily the low levels of antibodies found in sera of patients with early primary syphilis.[20]
The discrepant results between IMMUTREP TPHA and SD BIOLINE Syphilis 3.0 (IMMUTREP TPHA positive and SD BIOLINE Syphilis 3.0 negative sera) can be explained by the fact that a large number of treponemal antigens are exposed during the TPHA test. Therefore, some cross reaction with other organisms may occur. Moreover, as has been hypothesized by some researchers, though the recombinant antigens employed in the rapid tests are specific to T. pallidum, posttranslational processing of these protein in vivo or genetically determined unresponsiveness or restricted responsiveness to these antigens could lead to lack of reactivity even in the presence of disease.[21]
SD BIOLINE Syphilis 3.0 is a rapid, one-step test that is easy to execute, read, and interpret. Apart from serum samples, the test is also compatible with whole blood and plasma. Therefore, neither does the test require any preprocessing of specimens nor does it require any laboratory infrastructure or trained technical personnel for performing the test procedure. This makes the test an ideal on-site screening option in resource-constraint health-care settings without laboratory facilities. In addition, since the test detects treponema-specific antibodies, BFPs do not occur and the test can also be used as an alternative to TPHA for confirming the reactivity in nontreponemal assays. The rapid availability of results with the use of this test would also ensure prompt treatment of reactive patients in their very first visit to the health care services.
The test, however, is fraught with certain shortcomings. An important constraint to its application as a screening tool is that the treponema-specific antibodies detected by the test are retained for years and thus it cannot distinguish past treated infections from recent or active ones.[22] This implies that a large number of previously treated infections would also be picked up by SD BIOLINE Syphilis 3.0, particularly in high-prevalence settings, thereby leading to unnecessary treatment of patients. The test can also give a positive result in various nonvenereal treponematoses such as yaws and pinta.[23] However, some researchers argue that false positive results are preferable to false negative ones.[24] While with a false negative result, a syphilitic patient may go untreated and transmit the infection to others; a false positive serology would at least trigger repeat testing with alternative methods before a definitive diagnosis is made. In this context, we also suggest adopting a reverse algorithm, whereby a nontreponemal assay such as VDRL or RPR could be used to document active disease in patients with a reactive point-of-care treponemal test. Novel dual rapid point-of-care tests have also been devised where both treponemal and nontreponemal tests are combined into one device and can thus simultaneously serve as screening, as well as confirmatory assays.[25] However these tests are still under evaluation and not available for routine use.
Our study has a great relevance from public health perspective and based on our findings we recommend the use of rapid point-of-care procedures such as SD BIOLINE Syphilis 3.0 as primary screening assays for serodiagnosis of syphilis where laboratory facilities are not available and as tests to confirm nontreponemal reactivity where TPHA cannot be done. The study was conducted at a regional STI reference laboratory located at a tertiary care center in North India. The laboratory screens a large number of samples from in-patient and out-patient sections of various departments of the linked hospitals and thus caters to a diverse population base.
This study has a few limitations. First, the number of sera in the panel used for kit evaluation was small. In addition, ours was a laboratory-based study and the evaluation was not done under field or clinical conditions for which the test is primarily intended. Moreover, the test kit was exclusively evaluated using serum samples and its performance characteristics with whole blood and plasma specimens were not determined. Also, we did not have clinical information of the cases from which the reactive sera were obtained and, therefore, performance of the test according to the stage of syphilis could not be assessed.
CONCLUSION
To summarize, we strongly recommend the use of SD BIOLINE Syphilis 3.0 for rapid on-site diagnosis of syphilis. Further field studies are required before the test can be routinely implemented as a screening assay.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Clinical profile of sexual transmitted diseases in Cuttack. Indian J Dermatol Venereol Leprol. 1995;61:143-4.
- [Google Scholar]
- Changing trends in sexually transmitted infections at a Regional STD Centre in North India. Indian J Med Res. 2006;124:559-68.
- [Google Scholar]
- Novel Treponema pallidum serologic tests: A paradigm shift in syphilis screening for the 21st century. Clin Infect Dis. 2010;51:700-8.
- [Google Scholar]
- Cardiolipin antigens in the serodiagnosis of syphilis. Can J Public Health. 1952;43:128-35.
- [Google Scholar]
- Recombinant Treponema pallidum antigens in syphilis serology. Immunobiology. 1996-1997;196:535-49.
- [Google Scholar]
- False-positive rapid plasma reagin tests in human immunodeficiency virus infection and relationship to anti-cardiolipin antibody and serum immunoglobulin levels. J Infect Dis. 1994;169:1356-9.
- [Google Scholar]
- Are you sure it's syphilis. A review of false positive serology? Int J STD AIDS. 1995;6:241-8.
- [Google Scholar]
- Biological true and false serological tests for syphilis: Their relationship with anticardiolipin antibodies. Dermatologica. 1990;180:151-3.
- [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Discordant results from reverse sequence syphilis screening – five laboratories, United States, 2006-2010. MMWR Morb Mortal Wkly Rep. 2011;60:133-7.
- [Google Scholar]
- False-negative syphilis screening: The prozone phenomenon, nonimmune hydrops, and diagnosis of syphilis during pregnancy. Am J Obstet Gynecol. 1990;163:975-7.
- [Google Scholar]
- Evaluation of a new competitive immunoassay (BioElisa Syphilis) for screening for Treponema pallidum antibodies at various stages of syphilis. J Clin Microbiol. 1998;36:358-61.
- [Google Scholar]
- Why do we need quality-assured diagnostic tests for sexually transmitted infections? Nat Rev Microbiol. 2006;4:909-21.
- [Google Scholar]
- Point-of-care tests for diagnosing infections in the developing world. Clin Microbiol Infect. 2010;16:1062-9.
- [Google Scholar]
- Point-of-care tests to strengthen health systems and save newborn lives: The case of syphilis. PLoS Med. 2012;9:e1001233.
- [Google Scholar]
- Clinical evaluation of four recombinant Treponema pallidum antigen-based rapid tests in the diagnosis of syphilis. Chin Med Sci J. 2007;22:250-3.
- [Google Scholar]
- Comparison of the performance of SD Bioline Syphilis 3.0 assay with the RPR test for the syphilis screening in Dar es Salaam, Tanzania. Tanzania Med J. 2006;21:6-7.
- [Google Scholar]
- Clinical evaluation of four recombinant Treponema pallidum antigen-based rapid diagnostic tests for syphilis. J Eur Acad Dermatol Venereol. 2009;23:648-50.
- [Google Scholar]
- Assessment of the rapid test based on an immunochromatography technique for detecting anti-Treponema pallidum antibodies. Rev Inst Med Trop Sao Paulo. 2003;45:319-22.
- [Google Scholar]
- Performance of the rapid plasma reagin and the rapid syphilis screening tests in the diagnosis of syphilis in field conditions in rural Africa. Sex Transm Infect. 2002;78:282-5.
- [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Syphilis testing algorithms using treponemal tests for initial screening – Four laboratories, New York City, 2005-2006. MMWR Morb Mortal Wkly Rep. 2008;57:872-5.
- [Google Scholar]
- The laboratory diagnosis of syphilis. Can J Infect Dis Med Microbiol. 2005;16:45-51.
- [Google Scholar]
- Evaluation of rapid diagnostic tests for the detection of human immunodeficiency virus types 1 and 2, hepatitis B surface antigen, and syphilis in Ho Chi Minh City, Vietnam. Am J Trop Med Hyg. 2000;62:301-9.
- [Google Scholar]
- Novel point-of-care test for simultaneous detection of nontreponemal and treponemal antibodies in patients with syphilis. J Clin Microbiol. 2010;48:4615-9.
- [Google Scholar]



