
Translate this page into:
Actinomycosis of the gallbladder: A rare case report and literature review

*Corresponding author: Manupriya Sharma, Additional Professor, Department of Pathology and Lab Medicine, All India Institute of Medical Sciences, Bilaspur, Himachal Pradesh, India. manupriya.priyasharma@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh R, Sharma M, Bharti S, Chopra S, Rana L. Actinomycosis of the gallbladder: A rare case report and literature review. J Lab Physicians. 2025;17:134-7. doi: 10.25259/JLP_70_2024
Abstract
Actinomycosis of the gallbladder is rare, with only a few documented cases in the medical literature. Actinomyces is typically part of the normal flora of the cervicofacial region, gastrointestinal tract, and urogenital tract. Here, we report a case of a 31-year-old female who presented with pain abdomen. Radiological investigation revealed a contracted gallbladder with multiple calculi and a thickened wall. A provisional diagnosis of acute cholecystitis was considered preoperatively and hence planned for laparoscopic cholecystectomy. Histopathological examination showed moderate lymphocytic infiltrate within the muscular layer of the gallbladder along with colonies of filamentous bacteria suggestive of actinomycosis. The relevant stains, including Gram and Giemsa, highlighted the Gram-positive bacteria and confirmed the diagnosis. Post-cholecystectomy, the patient received prolonged antibiotic therapy to prevent recurrence.
Keywords
Actinomycosis
Cholecystitis
Cholelithiasis
Gallbladder

INTRODUCTION
Actinomycosis is an atypical chronic suppurative disease caused by a Gram-positive anaerobic filamentous bacterium, typically Actinomyces species. This organism is typically a harmless inhabitant of the human oral, gastrointestinal, and genitourinary tracts.[1] However, under certain conditions, it can cause severe infections characterized by the formation of abscesses, tissue fibrosis, and draining sinuses. Although commonly associated with cervicofacial, thoracic, and abdominopelvic infections, actinomycosis of the gallbladder remains exceedingly rare, with limited cases reported worldwide.[2] This rarity often leads to its incidental discovery during histopathological examination post-cholecystectomy, as symptoms usually mimic more common gallbladder diseases such as cholecystitis or cholelithiasis.
This case report aims to describe a rare case of gallbladder actinomycosis in a 31-year-old female presenting with non-specific abdominal pain, diagnosed through histopathological examination following a cholecystectomy. It contributes to the limited global documentation of gallbladder actinomycosis, marking it as one of the very few cases reported in India, where such diagnoses are exceedingly rare and seldom documented in the medical literature. This report underscores the importance of considering actinomycosis in the differential diagnosis of gallbladder disease, particularly in patients presenting with typical symptoms of cholecystitis but who respond poorly to conventional treatment. By reviewing the literature and adding another case to the scarce reports, we aim to enhance awareness among clinicians and pathologists regarding this unusual but significant pathological entity.
CASE REPORT
A 31-year-old female presented with a complaint of abdominal pain in the right hypochondrium, which she had experienced intermittently over the past 4 years. There was no associated history of nausea, vomiting, bloating, or fever. The patient had no history of any abdominal surgery, and there was no personal history of diabetes mellitus or hypertension. On general physical examination, tenderness over the abdomen was present. Ultrasonography revealed a contracted gallbladder with multiple calculi and a thickened wall. However, no mass was identified on ultrasonography [Figure 1].
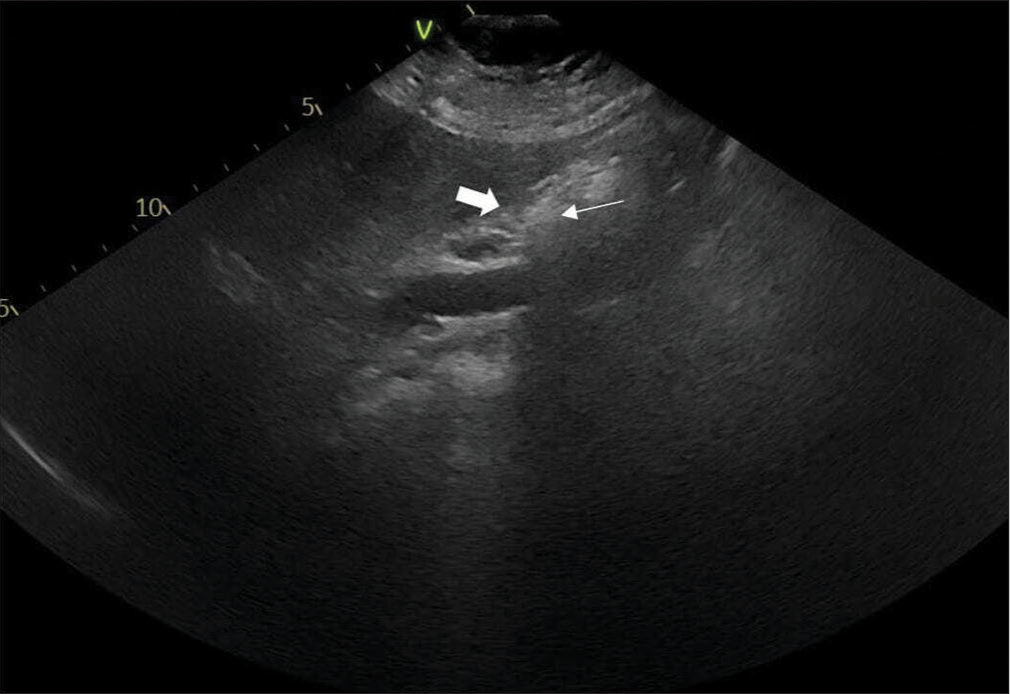
- A sonographic image of the patient shows a contracted gallbladder (thick white arrow) with a thickened wall with calculi (thin white arrow) seen with the gallbladder having posterior acoustic shadows.
In blood investigations, her hemoglobin level was 11.7 g/dL, and her total leukocyte count was 6.90 × 103/µL, both of which were normal. The liver function test, lipid profile test, serum amylase, and lipase levels were within normal ranges. Tests for human immunodeficiency virus and hepatitis B were both negative. The pre-operative diagnosis was chronic cholecystitis with cholelithiasis, and the patient underwent laparoscopic cholecystectomy. Intraoperative findings revealed dense adhesions of the gallbladder to the duodenum and surrounding structures. The gallbladder specimen was sent for histopathological examination.
On gross examination, the gallbladder was distended and measured 7 × 3 × 2 cm. The serosa was dull and congested. On the cut opening, there were multiple calculi in the lumen, and the wall thickness varied from 0.5 to 1 cm. Mucosa was ulcerated and hemorrhagic in many places. Microscopic examination revealed ulcerated mucosal epithelium with dense inflammation predominantly comprising neutrophils admixed with few lymphocytes. At places, numerous colonies of filamentous bacilli with sulfur granules were observed [Figure 2]. On Gram stain, aggregates of Gram-positive rods were seen [Figure 3]. Ziehl–Neelsen stain was negative. No evidence of any dysplasia or malignancy was found.
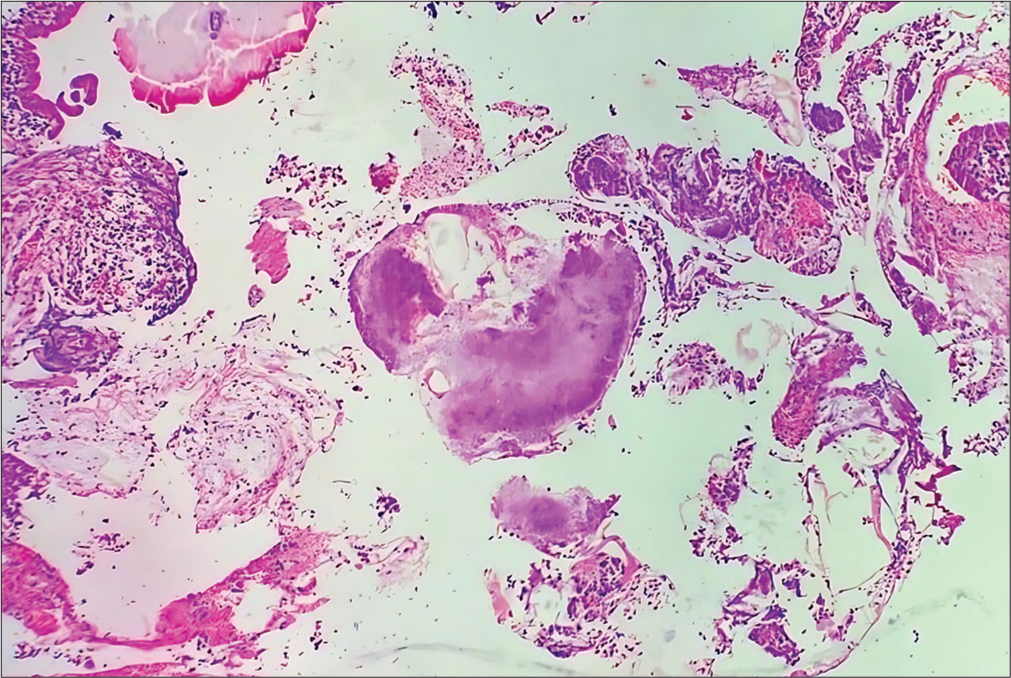
- Histopathological examination of the gallbladder revealed features of chronic cholecystitis along with spherical colonies of actinomycosis composed of radiating filaments (Hematoxylin and Eosin (HE) ×40).
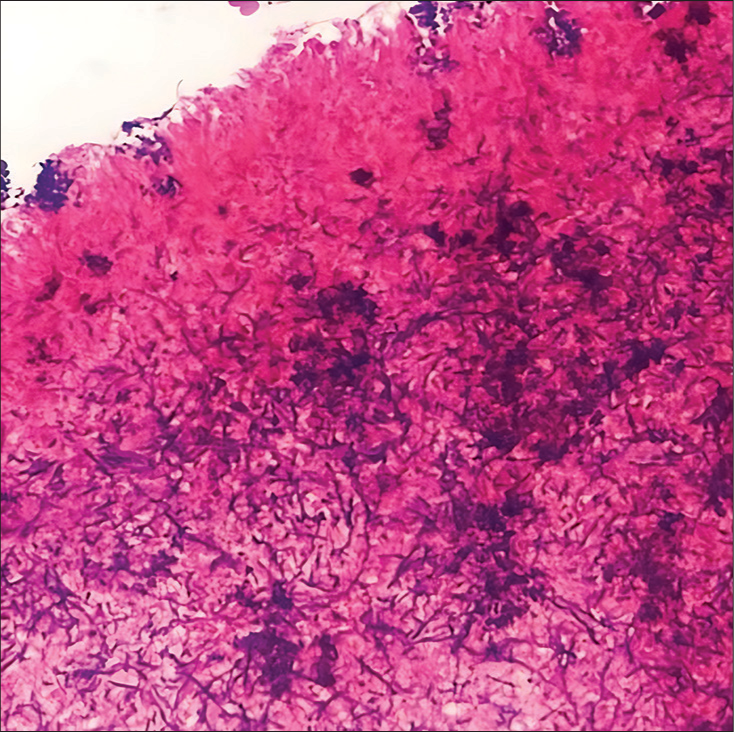
- Gram stain (×40) highlights aggregates of actinomyces bacilli.
Postoperatively, the patient was treated with intravenous penicillin for 1 week, followed by oral penicillin therapy for 6 months to prevent recurrence.
DISCUSSION
Actinomycosis, caused by Actinomyces species, is an intriguing pathology that exemplifies the complexity of infectious diseases, particularly due to its ability to mimic other conditions and its challenging diagnosis. Actinomyces is a Gram-positive, filamentous bacterium commonly residing as a commensal in the oral, gastrointestinal, and genitourinary tracts. Despite its prevalence in these areas, it infrequently affects the hepatobiliary system, accounting for less than 5% of cases. The most commonly identified species include Actinomyces israelii, Actinomyces gerenseriae, and Actinomyces naeslundii.[3]
We did the literature search over the past 15 years (1989–2024) using the search engine PubMed and using MeSh terms “Actinomycosis AND Gallbladder,” “Actinomycosis AND Cholecystitis,” and “Actinomycosis AND Cholelithiasis.” We reviewed 19 kinds of literature on the subject. Using inclusion and exclusion criteria, nine pieces of literature were found relevant and included in the review.[2-9] Articles published in English were mainly included in the analysis. The cases have been documented across various countries and patient demographics. It underlines the global but sparse reporting of this condition [Table 1]. Notably, there has been only one documented case in India by Arora et al. in 1997, highlighting the rarity of such diagnoses in India.[2,3]
| S. No. | Year | Country | Age/Sex | Stones | Clinical details | Sites | Special stain | Identification |
|---|---|---|---|---|---|---|---|---|
| 1. | 1997 | India | 65/F | + | Abdominal pain | GB | Gram’s+ | Actinomyces sp.[2] |
| 2. | 1998 | USA | 80/F | + | Abdominal pain | CBD | Gram’s+ | A. naeslundii.[3] |
| 3. | 2004 | Australia | 71/F | - | Jaundice with abdominal pain | GB | NP | Actinomyces sp.[4] |
| 4. | 2005 | Sudan | 50/M | + | Abdominal pain | GB | Gram’s+PAS+ | Actinomyces sp.[5] |
| 5. | 2007 | Korea | 65/M | + | Abdominal pain | GB | NP | Actinomyces sp.[6] |
| 6. | 2008 | Chile | 41/M | - | Gallbladder Ca | GB | NP | Actinomyces sp.[7] |
| 7. | 2009 | Korea | 56/M | + | Abdominal pain | GB | Gram’s+ | Actinomyces sp.[8] |
| 8. | 2021 | Nepal | 60/M | + | Abdominal pain | GB | Gram’s+ | Actinomyces sp.[9] |
| 9. | 2022 | Japan | 75/M | + | Acute cholecystitis with liver abscess | GB | Gram’s+ | Actinomyces odontolyticus.[1] |
GB: Gallbladder, PAS: Periodic acid Schiff, NP: Not performed, CBD: Common bile duct
In our case, the clinical presentation mirrored that of chronic cholecystitis without specific symptoms directly indicating actinomycosis. This situation is a common complication in diagnosing gallbladder actinomycosis, as the symptoms often overlap with more prevalent gallbladder diseases such as cholecystitis and cholelithiasis. It is hypothesized that in our patient, actinomycosis may have been facilitated by bacterial reflux from the duodenum into an inflamed gallbladder, showcasing the opportunistic nature of this infection.
Various predisposing factors contribute to the development of actinomycosis, including surgical operations, endoscopic manipulations, compromised immune status, and chronic inflammatory conditions that breach the mucosal barrier, facilitating bacterial invasion. This underscores the need for a nuanced diagnostic approach, particularly given the potential for misdiagnosis. [8]
In most of the literature, presenting complaints of actinomycosis of the gallbladder included epigastric pain, with radiological findings typically revealing cholelithiasis and a thickened gallbladder wall, similar to our case. However, two reports documented notably different clinical and radiological findings. Furuya et al. described a patient with recurrent episodes of acute cholecystitis, where ultrasonography revealed acute cholecystitis complicated by a liver abscess. They reported the rare isolation of Actinomyces odontolyticus in bile, whereas A. israeli is typically the most common pathogen.[1] Similarly, in a case reported by Lee et al. in 2007, ultrasonography and computed tomography revealed a gallbladder mass with impacted stones, leading to surgery under suspicion of gallbladder carcinoma.[6]
A notable observation across most of the literature is that these cases predominantly involved older individuals, whereas our patient was a younger female, adding an uncommon demographic to the documented cases. In our case, it could not be performed as the diagnosis was made post-operatively, and thus, the specific variant of Actinomyces could not be identified.
Histopathological examination remains the definitive method for identifying actinomycosis, supported by the characteristic sulfur granules-dense filamentous aggregates visible in the histological examination, which need to be confirmed through special stains. Actinomycosis and Nocardia come in the differential. Both Actinomycosis and Nocardia are Grams and Giemsa positive. However, Nocardia is weakly acidic fast, and Actinomyces is nonacid fast, as in the present case, which helped in the diagnosis.
Effective management involves an aggressive regimen of antibiotics, primarily high-dose penicillin, aimed at addressing both aerobic and anaerobic bacterial challenges and preventing recurrence.[9] This case emphasizes the critical need for awareness among clinicians to consider actinomycosis in differential diagnoses, especially in patients presenting with typical symptoms of gallbladder diseases but who respond inadequately to standard treatment protocols.
CONCLUSIONS
Thus, actinomycosis is an incidental finding in cholecystectomy specimens. The diagnosis is challenging, as patients often have non-specific symptoms that can mimic symptomatic cholelithiasis or gallbladder carcinoma. Therefore, pathologists should be vigilant in examining gallbladder specimens for this unpredictable occurrence of actinomycosis in the background of cholelithiasis. Prolonged antibiotic therapy is necessary to prevent recurrence.
Author contribution
RS, MS, SB: Literature search and manuscript writing; MS, SC, LR: Manuscript review and final editing.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- A case of recurrent acute cholecystitis caused by Actinomyces odontolyticus rare actinomycosis. BMC Infect Dis. 2022;22:518.
- [CrossRef] [PubMed] [Google Scholar]
- Actinomycosis of the cholecystic duct: Case report and review. Pathology. 1998;30:65-7.
- [CrossRef] [PubMed] [Google Scholar]
- Cytologic diagnosis of suppurative cholecystitis due to Candida albicans and Actinomyces A report of 2 cases. Acta Cytol. 2004;48:407-10.
- [CrossRef] [PubMed] [Google Scholar]
- Actinomycosis of the gallbladder: Case report and review of the literature. Asian J Surg. 2005;28:230-2.
- [CrossRef] [PubMed] [Google Scholar]
- Actinomycosis of the gallbladder mimicking carcinoma: A case report with US and CT findings. Korean J Radiol. 2007;8:169-72.
- [CrossRef] [PubMed] [Google Scholar]
- Actinomycosis: A great pretender. Case reports of unusual presentations and a review of the literature. Int J Infect Dis. 2008;12:358-62.
- [CrossRef] [PubMed] [Google Scholar]
- A case of actinomycosis of gallbladder presenting as acute cholecystitis. Korean J Gastroenterol. 2009;53:261-4.
- [CrossRef] [PubMed] [Google Scholar]
- Actinomycosis of gallbladder in cholecystectomy specimen: A case report. JNMA J Nepal Med Assoc. 2021;59:1177-9.
- [CrossRef] [PubMed] [Google Scholar]



