
Translate this page into:
Angiosarcoma of the scalp – A histopathological surprise in a benign looking scalp lesion
 , Sushma Malik1, Vikram Singh1, Vipin Venugopal Nair2, Venkatesan Somasundaram1
, Sushma Malik1, Vikram Singh1, Vipin Venugopal Nair2, Venkatesan Somasundaram1
*Corresponding author: Chinmay Pendharkar, Department of Pathology, Armed Forces Medical College, Pune, Maharashtra, India. drchinmaypendharkar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Pendharkar C, Malik S, Singh V, Nair VV, Somasundaram V. Angiosarcoma of the scalp – A histopathological surprise in a benign looking scalp lesion. J Lab Physicians. 2025;17:138-41. doi: 10.25259/JLP_89_2024
Abstract
Angiosarcoma is an uncommon malignant tumor that primarily affects older people and affects vascular endothelial cells. This tumor is quite deceptive and could be mistaken for a benign lesion based on its presentation and progression. We describe the case of a 50-year-old male who had post-traumatic left occipital edema that appeared benign on radiography and clinical examination. The index of suspicion increased due to the sudden increase in size. The excised specimen’s histomorphology revealed a cellular tumor that was mitotically active with large areas of necrosis. Vimentin, CD34, CD31, and FLI1 were all positive in the tumor cells. Clinically benign looking scalp swelling turning out a highly aggressive fatal malignancy was surprising in this case. Histopathology and evaluation by immunophenotyping remain the gold standard in timely diagnosis.
Keywords
Angiosarcoma
Scalp lesions
Vascular tumor

INTRODUCTION
Scalp lesions present a diverse array of differential diagnoses, spanning from the relatively common benign conditions such as sebaceous cysts, pilar cysts, adnexal tumors, and spindle cell lesions to the more uncommon malignant conditions including squamous cell carcinoma and melanoma. An aggressive malignancy, angiosarcoma of the scalp is uncommon and is seen with a median age of 74 years, accounts for 0.1% soft tissue sarcomas, and is aggressive in nature with 5-year disease-free survival rates <24%.[1,2]
We report the case of a 50-year-old male patient who presented with 2 years of progressive benign-looking swelling over the cranium, which was identified as angiosarcoma upon subsequent histopathological examination. The diagnostic surprise is discussed in this article.
CASE REPORT
A 50-year-old male presented with a 2-year history of swelling in the left occipital region of his cranium. Before the development of this swelling, he disclosed an incidental fall in the bathroom. The initial size of the swelling was approximately 2 × 2 cm, and it exhibited a non-progressive pattern. However, 15 days before the patient visited this center, the condition experienced an abrupt increase in size, which compelled the patient to seek consultation. The patient’s medical history indicated that he had a documented case of varicose veins accompanied by chronic venous ulceration affecting the left lower limb.
A local examination identified a hard, spherical mass over the left occiput, positioned 2 cm medial to the left mastoid and 2 cm laterally to the midline. The mass measured 6 × 5 cm and had regular margins; no visible skin changes were observed [Figure 1]. A well-defined calcific density lesion was observed in the right medial occipital region in the non-contrast computed tomography head, which was associated with a left parieto-occipital scalp hematoma. Repeated fine needle aspiration cytologies were attempted but sufficient cells were not obtained. The patient underwent an excision biopsy of the lesion with a working diagnosis of osteoma of the scalp. Intraoperatively, the lesion was 6 × 5 cm, hard, and adherent to the occipital bone.
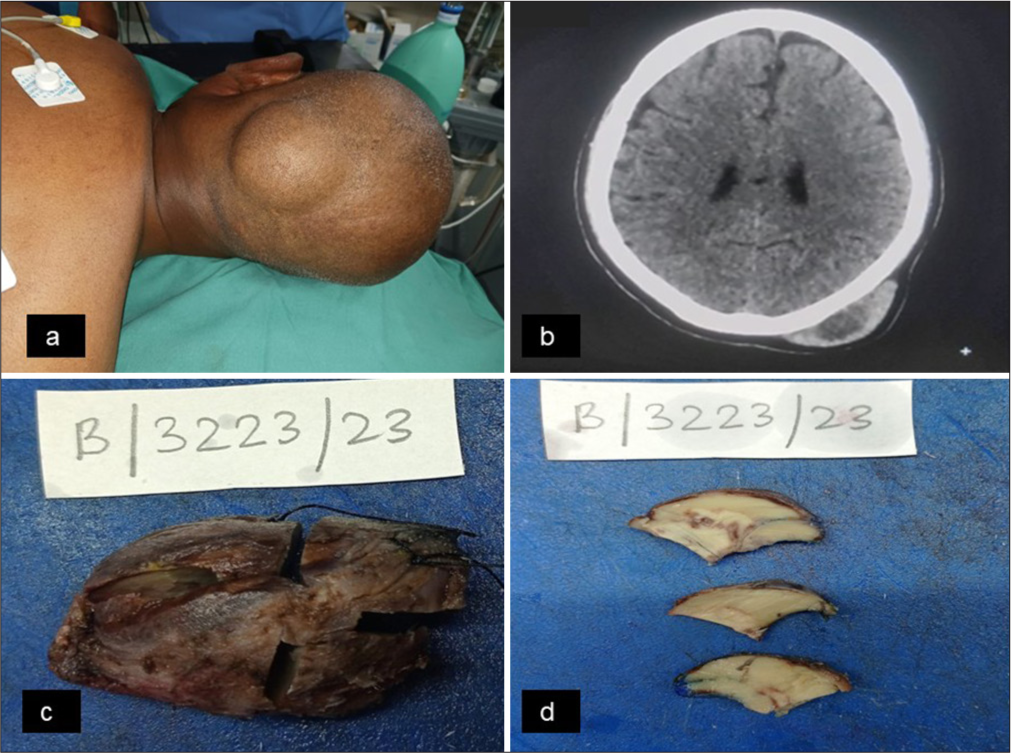
- (a) Clinical photograph shows the swelling over the scalp, (b) Computed tomography (CT) image of the swelling, (c) Gross appearance of the excised mass: External surface, (d) Gross appearance of the excised mass: Cut surface.
The specimen received for the histological examination showed normal skin overlying the tumor. The cut surface was whitish, homogeneous in appearance with few discolored necrotic areas. Microscopic examination showed large areas of necrosis. Viable areas revealed the presence of cellular tumors arranged in sheets, infiltrating into the underlying skeletal muscle fibers. Interspersed in these tumor cells, numerous varying-sized blood vessels were noted. Tumor cells and endothelial cells lining these blood vessels demonstrated round-to-oval nuclei showing dispersed chromatin and marked nuclear atypia. Brisk mitotic activity was also noted. All the margins were abutting the tumor (~1 mm) with the posterior margin being positive [Figure 2a-d].
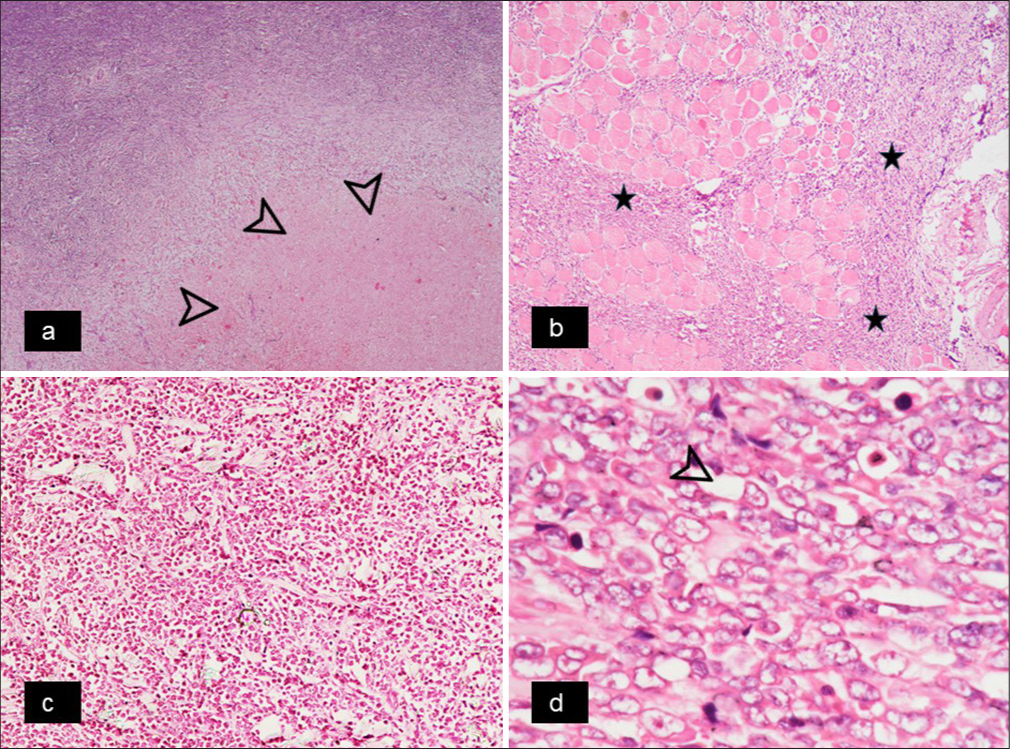
- (a) Photomicrograph shows viable tumor tissue (upper left) along with the area of necrosis (shown with black arrowheads) – Hematoxylin and eosin (H&E) stain, ×40, (b) The tumor shows invasion into the underlying skeletal muscle fibers (Infiltrating tumor cells are shown with asterisk) – H&E stain, ×100, (c) These tumor cells are seen lining the vascular spaces and exhibit moderate to marked nuclear pleomorphism – H&E stain, ×200, (d) The morphological details of the individual cells lining the vascular spaces (marked with black arrowhead) are better appreciable at higher magnification – H&E, ×1000.
For establishing the definitive diagnosis, immunohistochemistry was performed which showed that the tumor cells were positive for vimentin, Cluster of Differentiation 34 (CD34), Cluster of Differentiation 31 (CD31), and Friend Leukemia Integration 1 (FLI1) and negative for PanCK, CD99, Melan A, Human Melanoma Black 45 (HMB-45), and Leucocyte Common Antigen (LCA). In most proliferative areas, the Ki67 labeling index was 60–70%. Based on the characteristic histomorphological and immunohistochemical findings, the diagnosis of angiosarcoma was rendered [Figure 3a-f].
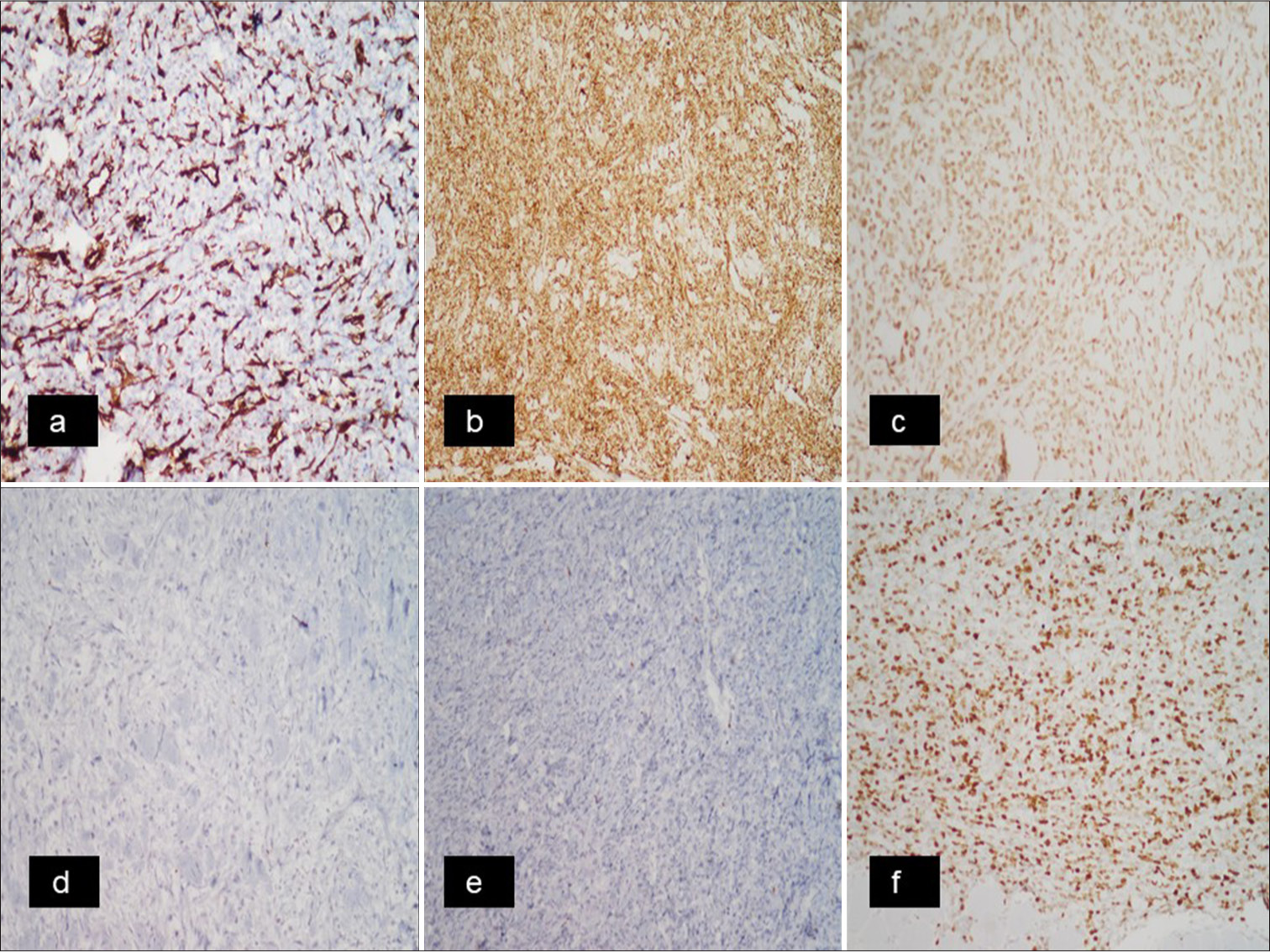
- Immunohistochemistry- (a) Tumor cells show positivity for vimentin (Vimentin, ×20), (b) Positivity for CD34 stresses the vascular endothelial origin of these tumor cells (CD34, ×100), (c) Tumor cells show positivity for FLI1 (FLI1, ×20), (d) Desmin immunohistochemistry shows absence of expression in tumor cells, ruling out the myogenic differentiation (Desmin, ×20), (e) HMB45 immunohistochemistry shows negative results, ruling out the melanoma (HMB45, ×20), (f) Ki67 Proliferation Index in most proliferative areas is around 60–70% (Ki67, ×20).
Because of the positive/abutting margins, the patient underwent revision-wide local excision and staged scalp reconstruction. Margins from the revision procedure were free of tumor.
DISCUSSION
Angiosarcomas are malignant vascular tumors that originate from endothelial cells. Aust et al. investigated angiosarcomas in the head and neck, with the most common presenting complaint being a mass over the scalp, as found in our case.[3]
The malignancy primarily affects elderly males more than females with a median age at the time of diagnosis being 74 years.[4] The incidence of cutaneous angiosarcoma was found to be highest in white people (88%) with a mean age of 73 years; African Americans accounted for only 4% of cases, according to data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results program, which recorded 434 cases of the disease from 1973 to 2007.[5] However, this unusual malignancy has been recorded seldom from the Indian subcontinent, with only a few case reports.
The etiology of cutaneous angiosarcoma is unclear but may be related to previous radiation exposure or chronic lymphedema. Few cases related to lesions after trauma have been documented although its significance is unknown. Trauma usually alerts the patient to the presence of the lesion but is not responsible for the development of the tumor, and the index case also gave a similar history.[6]
Due to its multicentricity and widespread microscopic dissemination, cutaneous angiosarcoma is difficult to treat. Wide excision of the lesion to obtain a histologically tumor-free margin affects prognosis. Angiosarcoma has the highest rate of lymph node metastases among all soft tissue sarcomas of the head and neck and distant metastasis may occur in up to 50% with the lung being the most common site followed by the liver,[7] which was not found in our case. Delayed recurrence of angiosarcoma at distant sites has been reported, which makes regular, lifelong surveillance a must.
In widespread scalp angiosarcoma, high-dose brachytherapy with a surface mold approach has been used to avoid marginal recurrence. Alternatives to surgery include intralesional interferon alpha-2b and interleukin-2 plus surface irradiation. Angiosarcoma is rare and has no recognized chemotherapy; therefore, conventional chemotherapy is dubious. Liposomal doxorubicin with irradiation in large lesions has been established. Antiangiogenic paclitaxel treats scalp angiosarcoma effectively, according to Memorial Sloan Kettering Cancer Center experts.[8]
This tumor has a very bad prognosis due to delayed diagnosis. Early detection through biopsy offers the only realistic chance of a cure. The microscopic characteristics of the biopsy or material, together with the ultrastructural and histochemical markers, are used to make the diagnosis. Morgan et al., have shown that the most common histologic pattern was characterized by anastomosing dissecting sinusoids lined by atypical endothelial cells (64%) with 15% of cases showing a diffuse epithelioid or spindle cell proliferation and 21% showing a mixture of the 2 histologic patterns.[9] Dasgupta et al. reported a similar case in a 55-year-old woman who had a bleeding scalp mass diagnosed as pyogenic granuloma. Excision biopsy was found to be angiosarcoma with microscopic margin involvement. Two years passed without recurrence after staged reconstructive surgery without chemotherapy or radiotherapy.[10]
Wide excision of the lesion is done to achieve a histologically tumor-free margin as this has a direct impact on the prognosis. After wide excision, primary wound closure is usually not possible due to the tumor’s considerable microscopic dissemination. Only after tumor-free margins have been verified by histological analysis, a staged reconstruction is carried out. However, in our case, the patient initially underwent excision surgery in view of the clinical diagnosis of osteoma, but on histopathological examination of the excised soft tissue mass, it was diagnosed as angiosarcoma, where all the surgical margins were found abutting the tumor with one of the margins (posterior margin) being positive, for which revision surgery was done.
CONCLUSIONS
Angiosarcoma of the scalp is a highly aggressive cancer with a bad prognosis. Early diagnosis and rigorous early treatment can help improve outcomes. The current case report demonstrates that with rigorous histomorphological examination and immunohistochemical investigation, such rare neoplasms can be detected for early treatment, even if the main clinical diagnosis is ambiguous. Staged reconstructions and lifelong surveillance are recommended to detect any delayed distant metastases.
Author contributions
CSP, SUM, VS: Conceptualization, drafting of manuscript; CSP, SUM: Data curation; VS, VVN, SV: Critical and intellectual evaluation; All authors approved the final manuscript.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Histopathological spectrum of scalp tumors: Analysis with review of literature. Int J Head Neck Pathol. 2019;2:25.
- [CrossRef] [Google Scholar]
- Misdiagnosis of scalp angiosarcoma: A case report. World J Clin Cases. 2023;11:3099-104.
- [CrossRef] [PubMed] [Google Scholar]
- Angiosarcomas of the head and neck: Clinical and pathologic characteristics. Ann Otol Rhinol Laryngol. 1997;106:943-51.
- [CrossRef] [PubMed] [Google Scholar]
- Survival outcomes for cutaneous angiosarcoma of the scalp versus face. Head Neck. 2017;39:1205-11.
- [CrossRef] [PubMed] [Google Scholar]
- Cutaneous angiosarcoma. Analysis of 434 cases from the surveillance, epidemiology, and end results program, 1973-2007. Ann Diagn Pathol. 2011;15:93-7.
- [CrossRef] [PubMed] [Google Scholar]
- Cutaneous angiosarcoma of the head and neck: A case presentation and review of the literature. Ear Nose Throat J. 2006;85:672-4.
- [CrossRef] [PubMed] [Google Scholar]
- Angiosarcoma of the scalp with calvarium involvement in a 50 year old African-American man. J Nat Med Assoc. 2004;96:1507-12.
- [Google Scholar]
- Angiosarcoma of the scalp. Indian J Plast Surg. 2009;42:118-21.
- [CrossRef] [PubMed] [Google Scholar]
- Cutaneous angiosarcoma: A case series with prognostic correlation. J Am Acad Dermatol. 2004;50:867-74.
- [CrossRef] [PubMed] [Google Scholar]
- Angiosarcoma of the scalp. Indian J Plast Surg. 2009;42:118-21.
- [CrossRef] [PubMed] [Google Scholar]



