
Translate this page into:
A Case of Empyema Thoracic due to Salmonella typhi in 18-month-old Child: An Unusual Cause
Address for correspondence: Dr. Devki Nandan, E-mail: devkinandan2002@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
We herein report an 18-months-old child who presented with high-grade fever, cough, and breathlessness along with tachypnoea and diminished air entry on the left side of the chest, in which a diagnosis of left-sided pleural effusion was made. Salmonella typhi was isolated from the pleural tap culture. The patient had uneventful recovery with appropriate antibiotic therapy. Empyema thoracic as a complication is extremely rare in the absence of an underlying co-morbid illness, is even more uncommon in a child, and is even rarer to find with Salmonella typhi species. After reviewing the available literature we could find only five cases of empyema thoracic due to Salmonella typhi in children with the age range of 9–13 years. We are reporting this case as the youngest child reported with this complication.
Keywords
Children
empyema thoracic
Salmonella typhi

INTRODUCTION
Complications of Salmonella typhi, besides gastrointestinal system, involve nervous system, bone marrow, kidneys, and heart.[1–3] Empyema thoracic due to S. typhi is a rarely reported complication, and most of the case reports are from adults. Cases with empyema thoracic due to Salmonella usually have underlying immunocompromised/comorbid conditions.[4] Although respiratory symptoms are common,[5] empyema thoracic is a rare occurrence in S. typhi infection. In reviews on cases with atypical manifestation of S. typhi infection, none of the 32 cases presented with empyema thoracic.[6] A review of the literature of past 100 years published in 2005 could find only 14 cases due to S. typhimuruim and 25 cases due to other nontyphi Salmonella.[7] A 10-year-old girl with bilateral pleural effusion due to S. typhi with high-level of ciprofloxacin resistance has been reported recently in the year 2010.[8] We herein report an 18-month-old immunocompetent child with empyema thoracic due to S. typhi, sensitive to ofloxacin, an extremely rare occurrence; as the youngest child reported with this complication till date.
CASE REPORT
An 18-months-old male child presented with history of high-grade fever for 1 month, cough for 15 days and progressive breathlessness of 7 days duration without relief of symptoms by medications prescribed by a local medical practitioner. History of loose stools, vomiting, significant weight loss, and contact with tuberculosis were absent. He belonged to a low socioeconomic class. He was a predominantly breast fed baby, and his mother had been suffering from fever 2 months back, which responded to 10 days of antibiotic therapy.
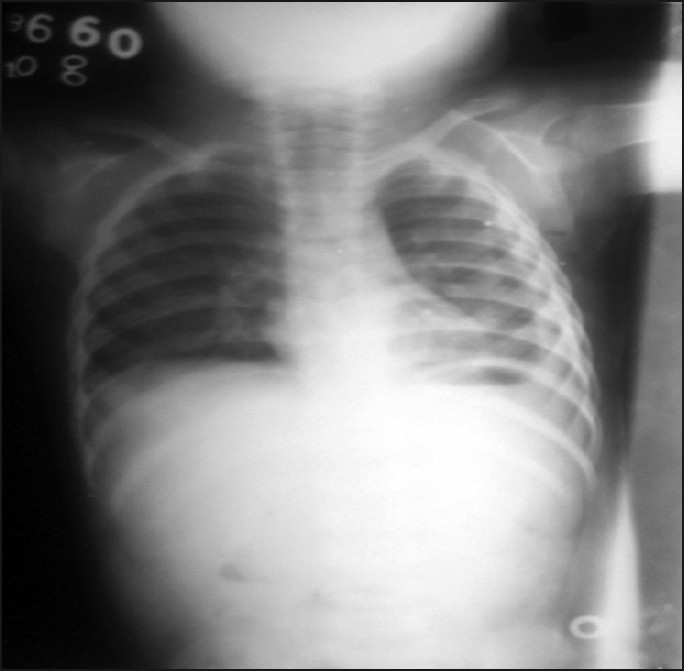
On examination, it was seen that he was acutely ill, irritable, pale, and febrile (temperature 39 °C). His weight was 9.6 kg. (> –2 SD as per WHO growth charts); the heart rate was 130/min; respiratory rate was 60/min with intercostal recession along with diminished air entry on the left side. Liver and spleen were not palpable. Diagnosis of left-sided pleural effusion was made and the same was confirmed on chest x-ray [Figure 1a]. Ultrasonography (USG) and CT further confirmed left-sided pleural effusion. Pleural tap was done and 150 mL of viscid purulent fluid was aspirated.

- X ray chest showing left sided pleural effusion.
Cell count of pleural fluid revealed a total of 6800 cells/mm3 (84% polymorphs and 16% lymphocytes) and proteins of 4.6 gm/dL. Intercostal drain (ICD) was placed and intravenous ceftriaxone and vancomycin was started empirically. Gram stain of pleural fluid revealed Gram negative bacilli. After 48 hrs of incubation, culture growth obtained was subjected to biochemical testes. These tests were suggestive of S. typhi. The organism was further confirmed using serotyping method and the confirmed S. typhi was reported along with antibiogram. Antibiogram showed sensitivity to ceftriaxone, ceftazidime, amikacin, ofloxacin, and ciprofloxacin. Ceftriaxone alone was continued. Blood and stool cultures were sterile and Widal test was positive (O titer of 1:120 and H titer of 1:240). Hemoglobin was 8.8 gm% and total leucocyte counts was 20,500 (Polymorphs 78%, Lymphocytes 20%, Eosinophils 2%,). Peripheral smear examination showed normocytic normochromic anemia with reticulocyte count of 2%. Liver function tests, renal function tests, serum electrolytes, iron profile, sickling test, and ultrasound abdomen were normal.
Intercostal drainage tube was removed after 5 days when no drainage was seen from the tube. However, even after 10 days of antibiotic therapy fever was persisting and x-ray chest was still hazy; therefore, a CT thorax was done that revealed loculated pus in the left pleural cavity [Figure 1b]. Based on pleural fluid culture sensitivity report, ofloxacin was added to the treatment. After 6 days of further treatment, the patient became afebrile and chest X-ray improved markedly with a total of fourteen days of ofloxacin therapy [Figure 2]. Repeat USG revealed minimal pleural effusion less than 30 cc. ELISA for HIV of both child and mother were negative and immunoglobulin profile (IgG, IgA, and IgM) of the child were normal. Echocardiography done to rule out pericardial involvement was normal. The patient was doing well during a year's follow up. To find out the source of infection in this child we investigated his mother, and performed cultures of her blood, urine, stool, and breast milk. Mother's stool culture was positive for S. typhi, and other cultures were sterile. A course of amoxicillin was prescribed for treatment of her carrier status and repeat stool culture after a month of follow up was sterile.
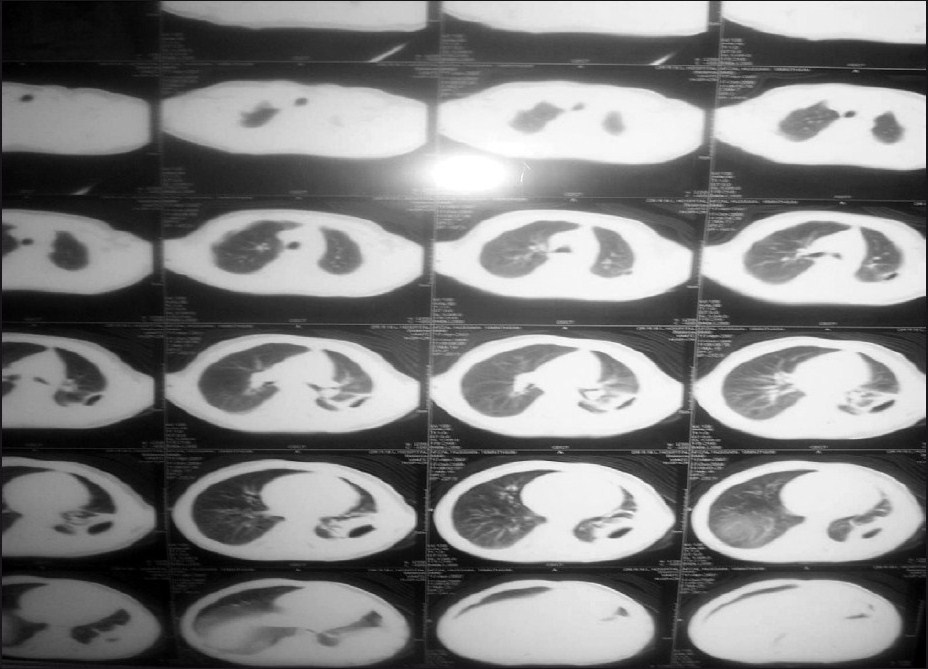
- CT thorax showing left sided pleural effusion
- Repeat x-ray showing improvement
DISCUSSION
Enteric fever caused by Salmonella group of organisms is an endemic infection in India with more than 0.3 million cases occurring every year.[9] It has been reported to occur in 10–20% of children less than 2 years of age.[110] Usual symptoms in children less than 2 years are fever (100%), cough (40%), diarrhea (35%), and vomiting (28%).[1] Common complications reported in the literature amongst children with Salmonella infection include encephalopathy, meningitis, chorea, gastrointestinal perforation and hemorrhage, myocarditis, shock, hepatitis, cholecystitis, acute renal failure occurring in 9.5% to 37% of these patients.[1–310] In a series of 42 children of less than 2 years of age with enteric fever, complications were reported in only four children; these included two cases of encephalopathy and ileus each.[1]
Extra intestinal involvements due to these organisms are encountered less frequently, but if they are, most of these occur in immune-compromised children.[11] Empyema thoracic due to Salmonella is extremely rare, even in the presence of underlying co-morbid illnesses such as lung disease, malignancy, diabetes, sickle cell anemia, or alcohol abuse and almost all of these case reports are due to nontyphoidal Salmonella.[5] On reviewing literature we could find only five cases of empyema thoracic due to S. typhi.[812–15] Four of these children had some associated condition such as splenic abscess, sickle cell anemia, protein energy malnutrition, and anemia except a case by Mohanty et al.[8] who previously had no other associated medical condition. Thus, we believe that the present case is the youngest child with S. typhi empyema thoracic who had no underlying immunodeficiency/co morbid conditions. The present case probably got the S. typhi infection from mother. The involvement of pleura in this child could have been either hematogenous or transdiaphragmatic spread from an abdominal focus. This case is interesting as he was immuno-competent and yet developed empyema thoracic in the absence of underlying lung disease or any other co-morbid condition at a very young age.
Underlying immunodeficiency or co morbid condition may not always be required for Salmonella organisms to present as empyema thoracic. In the era of antimicrobial drug resistance, awareness about this atypical presentation of Salmonella typhi is essential to initiate a prompt laboratory diagnosis and treatment.
ACKNOWLEDGMENT
The authors would like to thank Dr T.P Yadav, consultant in Pediatrics, PGIMER, and Dr RML Hospital for critically reviewing the manuscript & Dr B.P Baruah, Consultant & Head of Department of Radiology, Dr RML Hospital for providing radiological assistance.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Unusal complications in multidrug resistant Salmonella Typhi outbreak. Indian Pediatr. 1992;29:118-20.
- [Google Scholar]
- Changing characteristics of typhoid fever in Taiwan. J Microbiol Immunol Infect. 2004;37:109-14.
- [Google Scholar]
- Non-typhi Salmonella empyema: case report and review of the literature. Scand J Infect Dis. 2005;37:852-7.
- [Google Scholar]
- Bacteraemia with pleural effusions complicating typhoid fever caused by high-level ciprofloxacin-resistant Salmonella enterica serotype Typhi. Ann Trop Paediatr. 2010;30:233-40.
- [Google Scholar]
- Government of India. Health Information 1993. DGHS, New Delhi: Department of Publications, Govt. of India, Civil Lines; 1994.
- [Google Scholar]
- A clinical profile of multidrug resistant typhoid fever. Indian Pediatr. 1991;28:1171-4.
- [Google Scholar]
- Salmonella. In: Eigin RD, Cherry JD, eds. Text book of Pediatric infectious disease (4th ed). Philadelphia: W.B. Saunders; 1998. p. :1331-4.
- [Google Scholar]
- Sickle cell anaemia with Salmonella empyema thoracis: (a case report) Indian Pediatr. 1978;15:605-6.
- [Google Scholar]



