
Translate this page into:
A Rare Case of Mycetoma Due to Curvularia
Address for correspondence: Dr. H Sreedevi, E-mail: svh105192119@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Mycetoma due to Curvularia is a rare clinical entity. Here, we report a case of 27-year-old female presented with multiple swellings and discharging wounds around left shoulder joint since 12 years. Local examination showed diffuse nodular swellings over left anterior chest wall, posterior chest wall, and axilla. Multiple nodules and discharging sinuses were seen. Fungal culture of the biopsy of the lesion revealed Curvularia species. Patient showed significant clinical improvement with itraconazole therapy.
Keywords
Culture
Curvularia
eumycetoma
sinus
swelling

INTRODUCTION
Mycetomas are chronic subcutaneous infections caused by fungi or actinomycetes, known as eumycetoma and actinomycetoma, respectively.[1] It is usually posttraumatic, most commonly involves foot and rarely other body parts. It is mainly seen in Africa, India, Mexico, and South America. In India, actinomycetoma is prevalent in South, Southeast Rajasthan, and Chandigarh; while eumycetomas are common in North India.[2] The most common agents of eumycetomas are Madurella mycetomatis, Madurella grisea, Acremonium spp. and Fusarium spp.[3]
Here, we report a very rare case of Mycetoma occurred around the shoulder joint caused by Curvularia. To the best of our knowledge, only two reports of Mycetoma caused by Curvularia are reported till now.[45] This requires special importance because of a rarity of causative agent and involvement of uncommon site.
CASE REPORT
A 27-year-old housewife, from a nearby village presented to dermatology outpatient clinic of our hospital in March 2012 with complaints of multiple swellings and discharging wounds around the left shoulder joint since 12 years. She had taken treatment at multiple private hospitals without any relief and also etiological diagnosis. Patient did not remember any trauma to the particular part. Systemic examination did not reveal any abnormality. Local examination showed a diffuse nodular swelling located over left anterior chest wall, posterior chest wall and axilla. Multiple nodules and discharging sinuses were seen [Figure 1]. The discharge was seropurulent, and no granules were detected. Few sinuses were found healed with scarring. The skin over the area was hyperpigmented and thickened. There was no regional lymph node involvement.

- Multiple nodules and discharging sinuses around the left shoulder joint
All routine investigations including hematological, biochemical, and radiological tests were within normal limits. Pus samples from discharging sinuses were sent for microbiological investigation. Furthermore, multiple tissue biopsies were sent for histopathology and for bacterial and fungal culture. Gram stain of the pus sample showed plenty of pus cells along with Gram-positive cocci in clusters. Bacteriological culture yielded Staphylococcus aureus in pure culture. This was considered as a probable case of botryomycosis and was started on antibiotic therapy. There was no significant improvement in discharge. Multiple tissue fragments were cultured on Sabouraud's dextrose agar both with and without antibiotics and were incubated at room temperature and at 37°C. Fungal culture of multiple biopsies isolated black colored colonies after 1-week of incubation. Colonies were having black reverse and white aerial hyphae [Figure 2]. Microscopically, the lactophenol cotton blue preparation revealed septate, unbranched, brown-colored conidiophores along with conidia. The conidia were large, brown in color, with swollen subterminal cell, usually four-celled with three septa [Figure 3]. The isolate was identified as Curvularia species. Similarly, tissue biopsy showed basophilic centers and a dark periphery showing mycelia along with neutrophilic infiltrate. Patient was identified as a case of eumycotic Mycetoma considering laboratory confirmation and also the duration of the disease and nonresponsiveness to antibiotics. Patient was started on itraconazole 100 mg twice a day and responded well to the therapy with reduction of swelling and sinuses.

- Fungal colonies with white aerial hyphae and black reverse
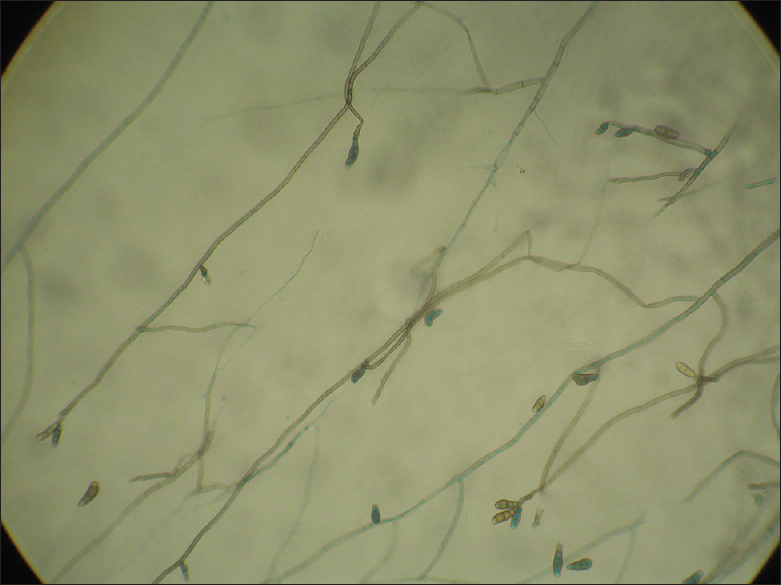
- Lactophenol cotton blue mount showing septate, unbranched, brown-colored conidiophores with large, brown conidia 3–4 septa
DISCUSSION
Mycetoma is a chronic slowly progressive, posttraumatic infection of subcutaneous tissue, usually involving foot. It is characterized by swelling, draining sinuses, and discharge of grains. Mycetoma caused by true fungi has been encountered less frequently as compared with those caused by actinomycetes. There are various etiological agents of eumycetoma, commoner ones are M. mycetomatis, M. grisea, Acremonium spp. and Fusarium spp. Curvularia causing mycetoma is very rare, and only a few cases have been reported.[2345]
Curvularia is a dematiaceous fungus that is ubiquitous among soil and vegetation in temperate areas. There are 31 species, and most commonly recovered in man has been Curvularia lunata, followed by Curvularia geniculata.[1] Originally thought to be solely a pathogen of plants but in the last centuries it is encountered in human infections also. Curvularia can cause ocular, respiratory, cerebral infections, and Mycetoma.
In the present case, there is an unusual site involvement. Here, lesions were present around the joint. Infection could be due to carrying wooden splint on head and shoulder joint which is a common practice in rural India.
Identification of causative agents of Mycetoma is very essential for proper and effective management of it as eumycetoma should be treated with adequate antifungal therapy and surgery whereas actinomycetoma responds well to antibacterial therapy. Currently, itraconazole and ketoconazole are the treatment options used for eumycetoma. This patient had lesions around shoulder joint hence was difficult for surgical therapy and was started on itraconazole. Within 3 months, the patient showed significant improvement in terms of reduction of discharging sinuses, nodules and healing by scarring.
To conclude, it is very important to determine the causative agent in every patient suspected of Mycetoma to establish an adequate and timely plan to avoid persistence and dissemination of the disease.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Agents of eumycotic Mycetomas. Topley and Wilsons Textbook of Microbiology. Vol 4. (10th ed). London: Hodder Arnold Ltd; 2005. p. :487-96.
- [Google Scholar]
- Mycetoma in Chandigarh and surrounding areas. Indian J Med Microbiol. 1998;16:64-5.
- [Google Scholar]
- The pathogenic fungi and pathogenic actinomycetes. Medical Mycology. (3rd ed). London: WB Saunders; 1998. p. :80-118.
- [Google Scholar]
- Eumycetoma due to Curvularia lunata. Indian J Dermatol Venereol Leprol. 2008;74:515-6.
- [Google Scholar]



