
Translate this page into:
A Rare Case of Primary Lymphoma of the Caecum Presenting as Intussusception
Address for correspondence: Dr. JB Leena, E-mail: drleenapriye@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Mucosa associated lymphoid tissue (MALT) lymphomas are rare neoplasms. They are most common in the stomach followed by small intestine and colon. The symptoms are nonspecific and generally do not present with intussusception. Here we report a rare clinical entity in which a 35-year-old female presented to the emergency with severe abdominal pain which was sudden in onset. History revealed that she had been having vague mild abdominal pain for 2 years. Ultrasonography showed ileocolic intussusception with hypoechoic lesion of 54 × 46 mm seen at the lead point. Emergency laparotomy with the right hemi-colectomy was done. The specimen was sent for histopathological examination which revealed a diagnosis of MALT lymphoma. Awareness of the varied clinical presentation helps in formulating the appropriate therapeutic strategy.
Keywords
Caecum
intussusception
primary lymphoma

INTRODUCTION
The term MALT lymphoma was first described by Isaacson and Wright in 1983.[1] Primary gastrointestinal lymphoma is very rare, constituting only about 1-4% of all gastrointestinal malignancies.[2] Due to infrequent occurrence, there are only few reports of colonic MALT type lymphoma, and absence of sufficient data makes evaluation and management of these patients challenging.[3] Adult intussusception is uncommon and accounts for 5% of all intussusception and 1% of all bowel obstruction.[4] Mucosa-associated lymphoid tissue (MALT) and diffuse large B cell lymphomas (DLBCL) are the two histologic subtypes most commonly observed.[5] Prognosis is poor when compared to gastric lymphomas.[6] Here, we report a case of a MALT lymphoma of the colon in a female patient who presented with intussusception. The therapeutic strategies of this rare entity are not well defined and require further research.
CASE REPORT
A 35-year-old woman presented with a pain in the right iliac fossa of one month duration with a sudden increase in the severity of the pain. On examination, a tender mass was palpable in the right iliac fossa. Ultrasound and CT scan of the abdomen revealed a ileocolic intussusception with homogenous enhancing mass lesion approximately 5.6 × 5.3 × 3.5 cms seen at the lead point. The ileocecal junction, cecum and ascending colon pulled up by intussusceptum. Multiple mesenteric nodes were seen. The differential diagnosis offered were adenoma/lymphoma. A right hemicolectomy was done with an uneventful postoperative course.
On gross examination, a fleshy circumscribed polypoid mass was seen at the caecum measuring 5.5 × 4.5 × 3.5 cm, with the cut surface showing areas of hemorrhage [Figure 1].

- Gross specimen: Polypoidal mass arising from the ileocecal region
Microscopy of the lesion with adjacent intestinal mucosa revealed necrosis of the mucosa. The lamina propria was infiltrated by a monotonous population of lymphoid cells that showed destruction of the glands and were seen extending into the muscularis propria and the serosa. The cells were small with irregular nuclear membrane, having hyperchromatic nucleus and scant cytoplasm. The tumor cells were characteristically arranged around the epithelium (lymphoepithelial lesion) [Figure 2]. Seventeen lymph nodes isolated showed reactive hyperplasia. A histological diagnosis of MALT lymphoma was offered. Immunohistochemistry was done which showed strong positivity of the tumor cells for CD-20 [Figure 3] and negative for CD 10, thus confirming the diagnosis. The patient was referred to oncology for chemotherapy.
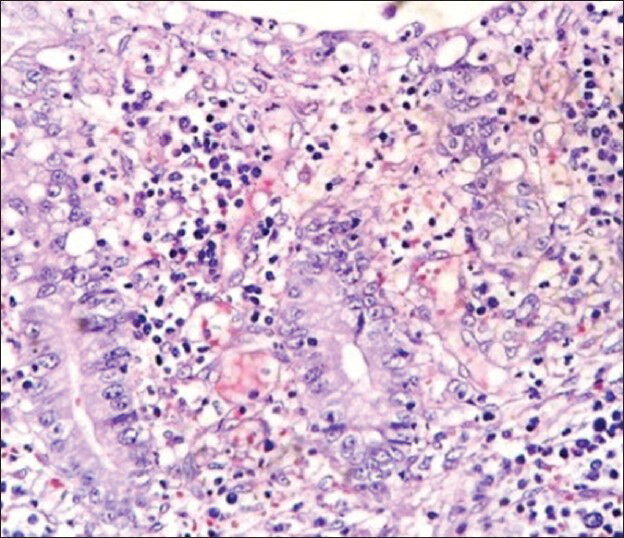
- Microscopy sections shows tumor cells infiltrating and surrounding the colonic epithelium. (H and E ×40)

- Immunohistochemistry staining positive for CD20
DISCUSSION
MALT lymphoma is defined as an extranodal marginal zone B-cell lymphoma of MALT type. Common age of presentation is middle age and older adults with both sexes being equally affected. The most common site in the large intestine is the caecum, as in our case, and the rectum.[7] Reports of colonic intussusception in adults are less common in literature and are confined to both small and large bowel. Colonic intussusception presents in a subacute manner with prolonged abdominal pain and constipation.[8] The symptoms of MALT lymphoma are nonspecific mimicking colorectal cancer and hence the delay in the diagnosis up to the last stage. Primary intestinal lymphoma most commonly involves the ileocecal region, probably due to the high proportion of lymphoid tissue.[7]
Because the ileocecal region includes the area from the distal ileum to the cecum, it is often difficult to designate the ileocecal region as part of the small or large intestine. Thus, the designation for this region differs among studies, as some considered it part of the small or large intestine.[9]
Our case was B-Cell lymphoma of the ileocecal region which presented as intussusception and had no regional lymph node involvement. Regional lymph nodes, if involved, are found to have a bad prognosis. The patient underwent surgery followed by chemotherapy with uneventful course during the three months follow-up period.
Immunohistochemical analysis can distinguish the MALT lymphoma from other low-grade lymphomas by detecting positivity for superficial immunoglobulins and pan B antigens – CD19, CD20, CD79 without expression of CD5, CD10, CD23 and cyclin D1.[10] Colorectal MALT lymphomas do not have the same association with H. pylori infection and are treated as a different clinical entity. In the absence of standardized treatment, various treatment methods have been used which include surgery, chemotherapy, radiation and endoscopic resection. As a causative organism has not been identified, the role of antibiotics is controversial.[11]
Convincing evidence has been established showing the relationship between H.pylori and gastric MALT lymphoma, and therefore therapeutic strategy has been altered for the patients with gastric MALT lymphoma in the early stages.[12] In contrast, a therapy for colonic MALT lymphoma has not yet been established due to rarity of the disease and late presentation.
Conservative treatment is preferred to surgery in the localized gastric lymphomas, the same is not true for intestinal lymphomas because the surgery in combination with chemotherapy has proven superior to any other treatment combination. Thus, because of the divergent therapies reported in the various studies, there are as yet no clear therapeutic guidelines for the treatment of MALT lymphoma of the colon.[13] Surgical resection may be effective when a colorectal MALT lymphoma does not respond to the eradication therapy or chemotherapy and is localized without dissemination. The survival of the patients with ileocecal region involvement is better than that of the patients with involvement at other sites, which might be related to the histologic distribution, the proportion of the tumor stage, and the need for surgical resection. T-cell lymphoma rarely occurs in the ileocecal region and present with complications, such as obstructions requiring immediate surgical intervention.[614] The treatment for primary malignant lymphomas in general requires a multidisciplinary approach, combining surgery and chemotherapy.
In conclusion, colonic MALT lymphoma is a rare entity presenting as intussusception. Though definitive treatment has not yet been established, combination of surgery and chemotherapy is thought to be superior to any other treatment combination.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Malignant lymphoma of mucosa-associated lymphoid tissue. A distinctive type of B-cell lymphoma. Cancer. 1983;52:1410-6.
- [Google Scholar]
- Increasing incidence rates, distribution and histological characteristics of primary gastrointestinal non-Hodgkin lymphoma in a North American population. Can J Gastroenterol. 2012;26:452-6.
- [Google Scholar]
- Primary extranodal lymphomas of stomach: Clinical presentation, diagnostic pitfalls and management. Ann Oncol. 2008;19:1992-9.
- [Google Scholar]
- Multicenter retrospective analysis of 581 patients with primary intestinal non-hodgkin lymphoma from the Consortium for Improving Survival of Lymphoma (CISL) BMC Cancer. 2011;11:321.
- [Google Scholar]
- Primary non-Hodgkin lymphomas in the small and large intestine: Clinicopathological characteristics and management of 40 patients. Int J Hematol. 2008;87:375-81.
- [Google Scholar]
- Laparoscopy-assisted ileocecal resection for mucosa-associated lymphoid tissue lymphoma of the appendix: Case report. Hepatogastroenterology. 2009;56:1078-81.
- [Google Scholar]
- Primary mucosa-associated lymphoid tissue (MALT) lymphoma occurring in the rectum: A case report and review of the literature. South Med J. 2006;99:1378-84.
- [Google Scholar]
- Regression of gastric high grade mucosa associated lymphoid tissue (MALT) lymphoma after Helicobacter pylori eradication. Gut. 2001;49:584-7.
- [Google Scholar]
- Primary lymphoma of the small intestine. A clinicopathological study of 119 cases. Am J Surg Pathol. 1993;17:429-42.
- [Google Scholar]
- Primary intestinal lymphoma: Clinical and therapeutic features of 32 patients. Haematologica. 1997;82:305-8.
- [Google Scholar]



