
Translate this page into:
Coinfection of chikungunya and dengue viruses: A serological study from North Western region of Punjab, India
Address for correspondence: Dr. Kanwardeep Singh, Department of Microbiology, GMC, Amritsar, Punjab, India. E-mail: kdmicrogmcasr@gmail.com
-
Received: ,
Accepted: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
INTRODUCTION:
Dengue and chikungunya (CHIK) infections appear to be increasing in all parts of India. Aedes aegypti mosquitoes are common vectors for dengue virus (DENV) and CHIK virus (CHIKV). In areas where both viruses cocirculate, they can be transmitted together. There are very few studies discussing the dengue-chik coinfection from Punjab region of India. The present study was undertaken to study the clinical features of dengue–CHIK coinfection and compare with monoinfection.
MATERIALS AND METHODS:
IgM antibody capture (MAC) ELISA for dengue IgM and CHIK IgM and ELISA for nonstructural protein 1 antigen was performed on serum samples obtained from suspected patients.
RESULTS:
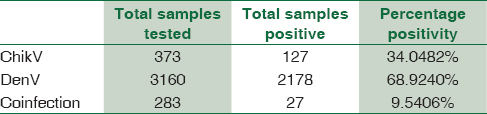
Out of total 3160 samples from suspected patients for dengue infection, 2178 (68.92%) samples were positive for DENV while CHIK IgM antibodies were positive in 127 patients out of the total suspected 373 cases (34.04%). In addition to this, 283 samples were tested for both viruses, out of which 27 sera were positive (9.54%) for coinfection of dengue and CHIK. The comparison of signs and symptoms showed that the coinfected patients had fever in all cases while rash was seen in only 30% cases. Arthralgia (79%) and thrombocytopenia (77%) was seen in significant number of coinfected cases thus revealing overlapping nature of dengue–CHIK coinfection.
CONCLUSION:
Increase in the number of Dengue and Chikungunya infections and their cocirculation is an important public health concern which warrants the implementation of strict control measures.
Keywords
Aedes aegypti
dual infection
ELISA
virology research and diagnostic laboratory

Introduction
Arthropod-borne viruses represent a global threat for public health as they can be transmitted to humans by bloodsucking vectors that are rapidly spreading worldwide. Aedes aegypti is an important vector mainly found in tropical and subtropical areas across the world[1] and is implicated in the spread of several arboviruses; most important of them being dengue virus (DENV) and chikungunya virus (CHIKV).
Dengue fever (DF) is a viral illness caused by a flavivirus and spreads by bite of A. aegypti mosquito. There are four serotypes of the virus referred to as DV-1, DV-2, DV-3, and DV-4. The name dengue originated from the Swahili word for “bone-breaking fever” or the word for “the walk of a dandie” in Spanish.[2] The spectrum of disease ranges from self-limited DF to more severe forms of dengue hemorrhagic fever (DHF) or dengue shock syndrome. The first major epidemic of the DHF occurred in 1953–1954 in Philippines followed by a quick global spread of epidemics of DF/DHF.[3] In India, the first confirmed outbreak occurred in Kolkata in 1963–1964.[4] Since then, there are many reports of dengue outbreaks from various parts of India.
CHIK fever is a viral disease caused by an alpha virus that is also spread by bite of A. aegypti mosquito. The name is derived from the Makonde word meaning that which bends up in reference to the stooped posture developed as a result of the arthritic symptoms of the disease.[5] CHIK first established its presence during a 1952–1953 epidemic outbreak in Tanzania.[6] In India, CHIKV was first isolated in Calcutta in 1963. The virus disappeared from our country after last reports from Maharashtra in 1973.[7] It then reemerged in 2006 after a gap of 32 years and caused an explosive outbreak affecting 13 states.[2]
In Asia, the CHIKV-affected areas overlap with DENV-endemic areas[89] and provide opportunities for mosquitoes to become infected with both viruses. Both the diseases have some common signs and symptoms which include fever with chills, swelling of major and minor joints with pain, difficulty in moving limbs, nausea, headache, and vomiting, and sometimes appearance of rashes.[10] In India, concurrent isolation of CHIKV and DENV had been reported since 1964 from different states.[911]
There have been no reports of coinfections from this part of the country in the past so we undertook this study to know the prevalence of dengue, CHIK monoinfection, and their coinfection in Amritsar and nearby districts during a major outbreak in 2016.
Materials and Methods
The study was conducted in Virology Research and Diagnostic Laboratory, Government Medical College (GMC), Amritsar, during June 2016–December 2016.
Blood samples were collected from patients attending different wards in hospital or visiting the outpatient departments at GMC and Hospital, Amritsar and other districts nearby with typical clinical history of high fever (>39°C) with chills, rashes, joint pain, swelling of joints, nausea/vomiting, headache, myalgia, and retro-orbital pain. Approximately, 2–5 ml of blood was collected, serum separated, and subjected to ELISA. IgM antibody capture (MAC) ELISA was performed using kit provided by National Institute of Virology (NIV), Pune, for dengue on patients presenting with fever >5 days while ELISA for nonstructural protein 1 antigen (fever <5 days) was performed (using Panbio Diagnostics kit, Germany) for patients presenting with fever of <5 days. CHIK IgM ELISA was performed on those samples in which request was made for testing CHIKV infection. In some samples both CHIKV and DENV were tested because requisition was made by the treating physician to check for both viruses. All tests were carried out following the manufacturer's instruction.
Results
In the present study, out of total 3160 samples from suspected patients for dengue infection, 2178 (68.92%) samples were positive for DENV. While 373 samples were tested for CHIK IgM antibodies which came positive in 127 patients (34.04%) [Table 1]. In addition to this, in 283 samples, requisition was made for testing both viruses, out of which 27 sera were positive (9.54%) for both dengue and CHIK.
Age-wise distribution of the DENV-infected and CHIKV-infected samples revealed that majority of the patients were in the productive age group of 21–40 years [Figure 1].
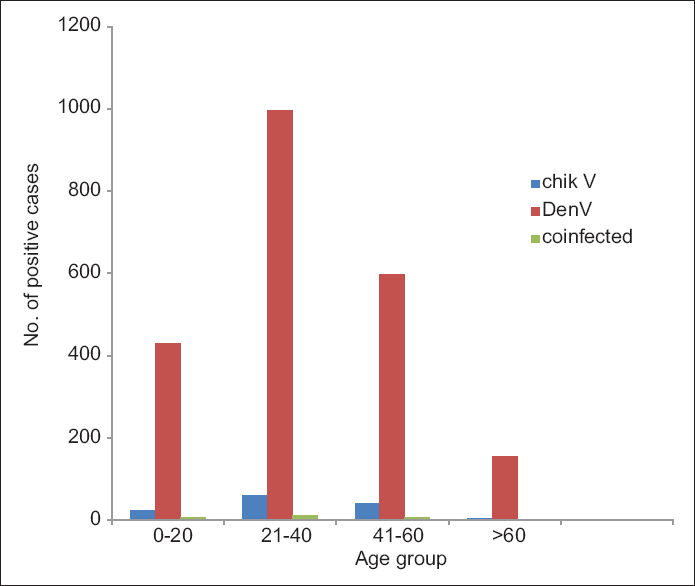
- Age distribution of cases
From the gender distribution of the positive samples, it was observed that a higher percentage of monoinfected patients with DENV were males (63.64%) compared to monoinfected patients with CHIKV where females outnumbered males (54.33%). However, there was no gender-based difference of infections among males and females of coinfected patients [Figure 2].
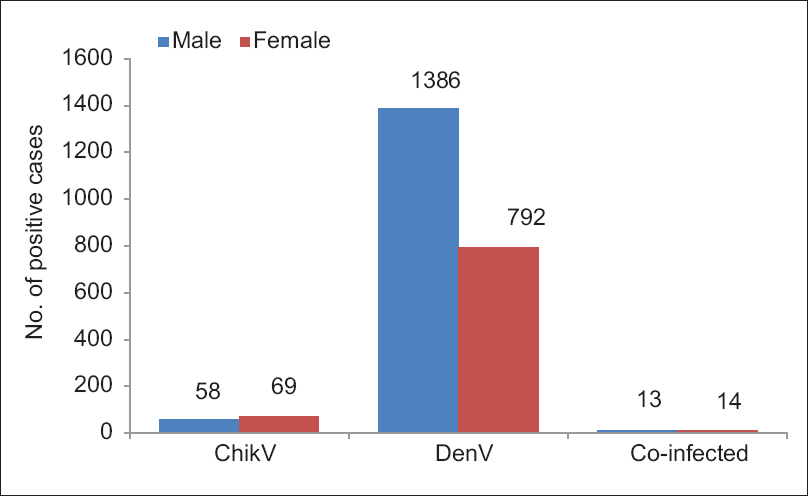
- Sex distribution of samples
The seasonal distribution of dengue cases showed a peak during the month of september while cases of chikungunya and coinfection predominated during October [Figure 3].
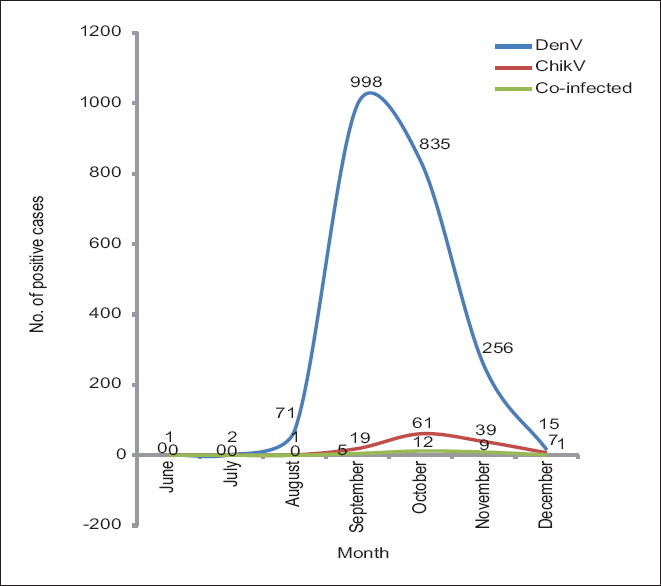
- Seasonal distribution of cases
Clinical comparison of the cases showed that fever (100%) was present in all patients while rash was seen more commonly in dengue-positive (80%) patients as compared to those with CHIK (48%) and dengue–CHIK coinfection (30%). Furthermore, myalgia was seen more prevalent among dengue patients (79.03%) while arthralgia predominated among CHIK patients (82%). Thrombocytopenia was more common in dengue monoinfection (85.07%) as compared to CHIK monoinfection (61%) [Figure 4].
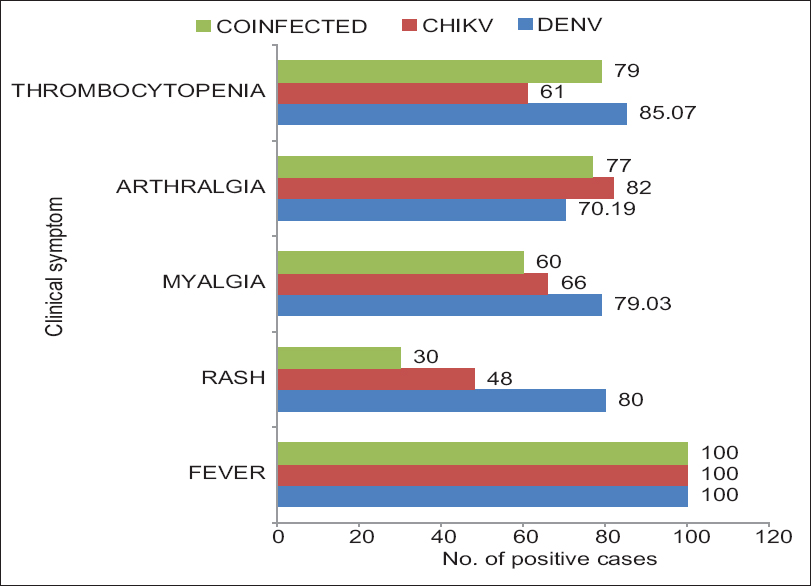
- Comparison of clinical signs and symptoms of dengue virus, chikungunya virus, and coinfected cases
Discussion
DF is highly endemic in northern India. CHIK has similar clinical presentation as dengue, so it has remained underreported in this part of the country. Even coinfections may result in illness with overlapping signs and symptoms, making diagnosis and treatment difficult for physicians. As mosquitoes are abundantly present, they may become infected with both types of viruses and often get transmitted to human beings as coinfections following the mosquito bite.
It is important to diagnose the type of virus with which the patient is infected because it can help the clinician in proper treatment and management of the patient against complications like haemorrhages, ARDS, renal failure and arthritis. Hence, diagnosis of the type of infection can help the clinician in proper management of the patients during treatment and follow-up.
There are few reports on dual infection, reported from other parts of India, showing patients coinfected with CHIKV and DENV.[1112]
In our study, although dengue cases predominated (68.92%), it was observed that the prevalence of CHIK cases (34.048%) has also increased as compared to the past years.[13] Coinfected cases were not reported earlier but our study reported a prevalence of 9.54%. The prevalence of coinfection using serological methods has been reported in the earlier studies by Kalawat et al. as 2.7%,[14]2.8% by Omarjee et al.,[15] and 12.4% by Taraphdar et al.[12]
Maximum number of cases belonged to the age group of 21–40 years, in all types of infections as this group is maximally involved in outdoor activities, and being occupationally active has higher chances of exposure to arthropod-borne viruses. Similar trend was observed by Lall et al.,[16] Neeraja et al.,[17] Babaliche and Doshi,[18] and Chattopadhyay et al.[7]
The CHIKV was slightly more prevalent in females (54%) as compared to the males (46%), supported by other findings by Balasubramaniam et al.[19] and Dwibedi et al.,[20] but it is in contrast with the pattern seen be Kalawat et al.[14] However, the males (64%) outnumbered females (36%) in DENV positivity and similar pattern was observed by other researchers.[21222324] There was almost an equal representation of males and females among coinfected cases.
Both types of infections were seen more during and subsequent to the monsoon months. The climatic conditions during this period favor vector-breeding places, thereby increasing the number of mosquitoes; resulting in a rise of dengue and CHIK. The reason may be due to prime occupation of the people being agriculture, and breeding of A. aegypti is highest during pre- and postmonsoon period.
In dengue-positive cases, symptoms such as fever, rash, myalgia, and thrombocytopenia were more common as compared to CHIK in which arthralgia and fever were the common presenting symptoms. Our clinical findings correlate with Babaliche and Doshi[18] and Londhey et al.[25]
The comparison of signs and symptoms showed that the coinfected patients had fever in all cases while rash was seen in only 30% cases. Arthralgia and thrombocytopenia were also seen in significant number of cases, thus revealing overlapping nature of dengue–CHIK coinfection.
Limitations of the study
The limitation of our study is the small sample size for dual infection cases. We would like to test our results with a larger sample size. Although RT-PCR is considered as standard criteria for confirmation of dual infections, we could not perform it as ours is a resource limited setting. But we used ELISA kits recommended by NIV, Pune which have fairly good sensitivity and specificity for diagnostic purposes. In some other studies also, coinfection has been diagnosed on the basis of ELISA only.[1114]
Conclusions
Repeated outbreaks of dengue, recent activity of CHIKV, and CHIKV/DENV coinfections in this region of Punjab suggest that the epidemiology of these viruses is changing in this region and that these viruses are becoming endemic to this region. Thus, in clinically suspected cases of dengue or CHIK fever, it is advisable to test for both viruses as they cocirculate. The widespread emergence of DENV and exponential increase in CHIK cases warrant the need for more effective surveillance to monitor the spread of these deadly arboviruses so that timely control strategies can be implemented.
Financial support and sponsorship
Financial support was provided by Department of Health Research (DHR), Ministry of Health and family Welfare and ICMR under Viral Research and diagnostic laboratory Project.
Conflicts of interest
There are no conflicts of interest.
References
- Macroclimate determines the global range limit of Aedes aegypti. Ecohealth. 2014;11:420-8.
- [Google Scholar]
- Current status of dengue and Chikungunya in India. WHO South East Asia J Public Health. 2014;3:22-6.
- [Google Scholar]
- Haemorrhagic fever in Calcutta: Some epidemiological observations. Indian J Med Res. 1964;52:651-9.
- [Google Scholar]
- Chikungunya fever: A re-emerging viral infection. Indian J Med Microbiol. 2008;26:5-12.
- [Google Scholar]
- Complete nucleotide sequence of chikungunya virus and evidence for an internal polyadenylation site. J Gen Virol. 2002;83:3075-84.
- [Google Scholar]
- Chikungunya virus infection in West Bengal, India. Indian J Med Microbiol. 2016;34:213-5.
- [Google Scholar]
- Concurrent isolation from patient of two arboviruses, chikungunya and dengue type 2. Science. 1967;157:1307-8.
- [Google Scholar]
- Emerging viral diseases of Southeast Asia and the Western Pacific. Emerg Infect Dis. 2001;7:497-504.
- [Google Scholar]
- Co-infection of dengue virus and chikungunya virus in two patients with acute febrile illness. Med J Malaysia. 2007;62:335-6.
- [Google Scholar]
- Co-infections with chikungunya virus and dengue virus in Delhi, India. Emerg Infect Dis. 2009;15:1077-80.
- [Google Scholar]
- A comparative study of clinical features between monotypic and dual infection cases with chikungunya virus and dengue virus in West Bengal, India. Am J Trop Med Hyg. 2012;86:720-3.
- [Google Scholar]
- Seroprevalence of common viral diseases: A hospital based study from Amritsar, India. J Clin Diagn Res. 2016;10:DC15-9.
- [Google Scholar]
- Prevalence of dengue and chickungunya fever and their co-infection. Indian J Pathol Microbiol. 2011;54:844-6.
- [Google Scholar]
- Importance of case definition to monitor ongoing outbreak of chikungunya virus on a background of actively circulating dengue virus, St.Martin, December 2013 to January 2014. Euro Surveill 2014:19. pii: 20753
- [Google Scholar]
- Sero-prevalence of dengue in tertiary care hospital in Delhi. Int J Curr Microbiol Appl Sci. 2016;5:439-45.
- [Google Scholar]
- Serodiagnosis of dengue virus infection in patients presenting to a tertiary care hospital. Indian J Med Microbiol. 2006;24:280-2.
- [Google Scholar]
- Catching dengue early: Clinical features and laboratory markers of dengue virus infection. J Assoc Physicians India. 2015;63:38-41.
- [Google Scholar]
- Prevalence of chikungunya in urban field practice area of a private medical college, Chennai. Indian J Community Med. 2011;36:124-7.
- [Google Scholar]
- Rapid spread of chikungunya virus infection in Orissa: India. Indian J Med Res. 2011;133:316-21.
- [Google Scholar]
- Recent trend of seroprevalence of dengue in Haryana. Int J Pharm Med Bio Sci. 2013;2:44-51.
- [Google Scholar]
- A hospital based serosurveillance study of dengue infection in Jaipur (Rajasthan), India. J Clin Diagn Res. 2013;7:1917-20.
- [Google Scholar]
- Seroprevalence of dengue viral infection in patients attending to a tertiary care hospital in Kanchipuram, Tamil Nadu, India. Int J Res Health Sci. 2014;2:818-22.
- [Google Scholar]
- Dengue and chikungunya virus co-infections: The inside story. J Assoc Physicians India. 2016;64:36-40.
- [Google Scholar]



