
Translate this page into:
Comparison of Immunocytochemistry and Immunohistochemistry on Breast Carcinoma: A Boon or a Bane?
Address for correspondence: Dr. Kempula Geethamala, E-mail: drgeethamala@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction:
Breast carcinoma is the most common cancer among women in the urban Indian population. Conventionally, immunohistochemistry (IHC) is done to determine the hormone receptor status of the tumor. Immunocytochemistry (ICC) on fine-needle aspiration cytology (FNAC) was carried out to determine the same hormone receptor status of the tumor.
Objective:
The study was undertaken to evaluate the diagnostic reliability of performing estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (Her2/neu) receptor status on FNAC by ICC and to compare the results with IHC.
Materials and Methods:
A 2 years 6 months prospective study conducted in the Department of Pathology, ESIC Medical College and PGIMSR and ESIC Model Hospital, Rajajinagar, Bengaluru, wherein 100 breast carcinoma patients' samples both cytology and histology were collected. IHC and ICC were done by peroxidase antiperoxidase technique. Validations of the receptor status were analyzed using sensitivity, specificity, positive and negative predictive values (PPV and NPV), and kappa statistics for agreements between ICC and IHC.
Results:
ICC was positive for ER, PR, and Her2/neu in 53, 50, and 22 cases, respectively. For ER, a cytohistologic correlation of 98%, with a sensitivity of 96.3%, specificity of 100%, and PPV and NPV being 100% and 95.7%. For PR, concordance of 97%, with a sensitivity of 94.3%, specificity of 100%, and PPV and NPV being 100% and 94%. Her2/neu had an agreement of 89%, with a sensitivity of 72%, specificity of 95.5%, and PPV and NPV being 85.7% and 90.1%.
Conclusion:
ICC has been a boon and can be a paramount diagnostic adjunct to the routine investigations.
Keywords
Breast carcinoma
immunocytochemistry
immunohistochemistry

INTRODUCTION
Breast carcinoma is the most common cancer among women in the urban Indian population and second only to cervical cancer in the rural population based on cancer registry data.[12] The most accepted protocol followed for the diagnosis of breast lumps is “Triple assessment” which includes clinical, radiological, and cytopathological assessment.[3] Detection of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor (Her2/neu) receptors in breast carcinoma is essential for pre- and post-operative chemoendocrine therapy and for predicting prognosis.[45] Conventionally, trucut biopsy and immunohistochemistry (IHC) are carried out on tissue sections to determine the hormone receptor status of the tumor. However, fine-needle aspiration cytology (FNAC) for breast lumps is a simple initial outpatient procedure which is easy, accurate, reliable, and repeatable. Hence, it would save time if these markers are performed on cytological material at the time of diagnosis using immunocytochemistry (ICC). Although immunocytochemical characterization of breast carcinoma on fine-needle aspirates is recognized as an effective procedure, there are only a few studies that compare the results obtained on fine-needle aspirates and on tissue sections; hence, the present study was undertaken.[6789]
Objectives
-
The study was undertaken to evaluate the diagnostic reliability of performing ER, PR, and Her2/neu receptor status on FNAC by ICC
-
And compare the results with IHC (gold standard) on tissue sections.
MATERIALS AND METHODS
FNAC of 100 breast carcinomas together with corresponding modified radical mastectomy (MRM) specimens paraffin-embedded tissue sections over a period of 2 years 6 months from September 2011 to March 2014 were studied in the Department of Pathology, ESIC Medical College and PGIMSR and ESIC Model Hospital, Rajajinagar, Bengaluru, FNAC smears were stained with H and E and material was checked, marked, destained, fixed for 10 min in cold acetone, and then used for ICC. Corresponding patients MRM specimens paraffin embedded tissue sections having both tumor and internal controls were taken for IHC. IHC and ICC were performed together by peroxidase-antiperoxidase technique and were reported by two independent pathologists. Monoclonal antibodies were obtained from “Scytec” company. ER (mouse monoclonal clone 1D5), PR (mouse monoclonal clone PR88), and Her2/neu (rabbit monoclonal clone EP1045Y). Hundred tumor cells on FNAC and 500 cells on tissue sections were counted for positivity. Cases of both ICC and IHC results of the same patient were available and were further taken up for correlative study. ER, PR positivity was denoted by nuclear staining using Allred scoring system which takes into account both intensity of staining and proportion of positive tumor cells. American Society of Clinical Oncology guidelines 2007 denoting cytoplasmic membrane staining was used for Her2/neu grading.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences software version 18.0 (SPSS Inc, Chicago). Obtained parameters were evaluated using descriptive statistical analysis and presented in terms of percentage. Validation of ER, PR, and Her2/neu receptors was analyzed using sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Kappa statistics was used to find the agreements between ICC and IHC hormone receptor status.
RESULTS
In the present study, majority of women with breast carcinoma were in the age group of 41–50 years 49/100 (49%) with the mean age of 48.2 ± 6.887 years. The youngest was 24 years and oldest 75 years. Left breast 50/100 (50%) was marginally more affected than right side 49/100 (49%) of breast and in a single case both breasts 1/100 (1%) were affected.
By ICC, ER+/PR+ 49/100 (49%) were the mostcommon hormone receptor expressed followed by triple negative 26/100 (26%) and Her2/neu positive21/100 (21%) [Table 1 and Figures 1–3]. By IHC, ER+/PR+52/100 (52%) were the most common hormone receptor expressed followed by Her2/neu 25/100 (25%) and triple negatives 20/100 (20%) [Table 2 and Figure 4]. Among the individual hormone receptor study by ICC, ER was expressed in 53/100 (53%), PR in 50/100 (50%), and Her2/neu in 22/92 (23.9%).

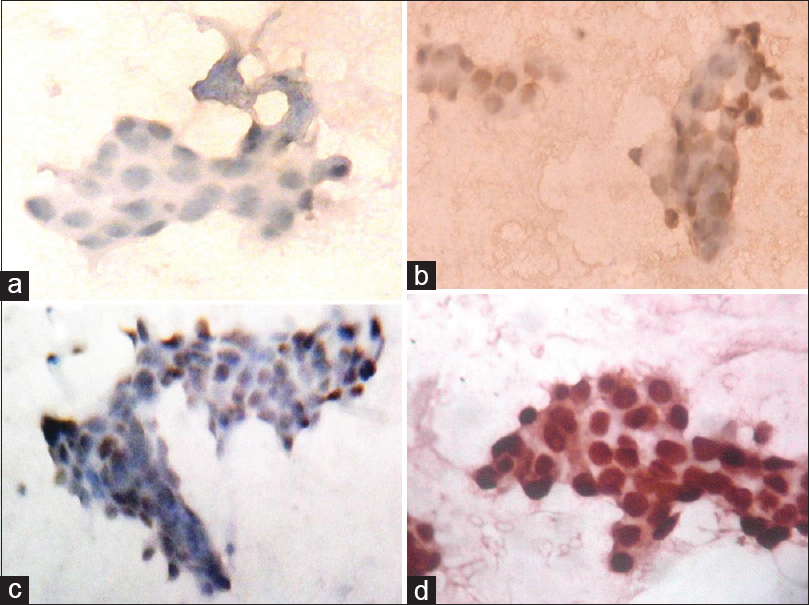
- (a) Immunocytochemistry-negative nuclear staining-estrogen receptor-Allred score-2-negative, (b) positive nuclear staining for estrogen receptor-Allred score-4-positive, (c) Allred score-6-positive, (d) Allred score-8-positive (×40)
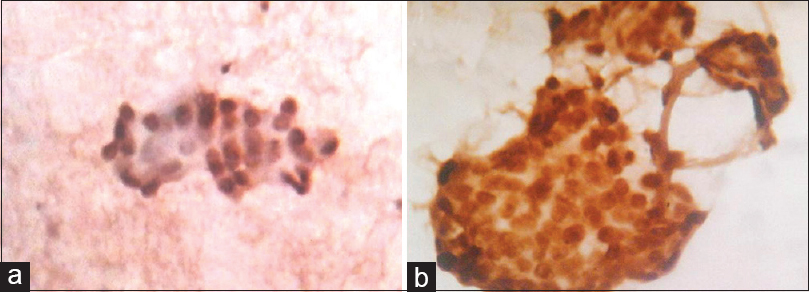
- (a) Immunocytochemistry photomicrograph of breast carcinoma shows positive nuclear staining for progesterone receptor-Allred score-6-positive (×10), (b) Allred score-8-positive (×40)
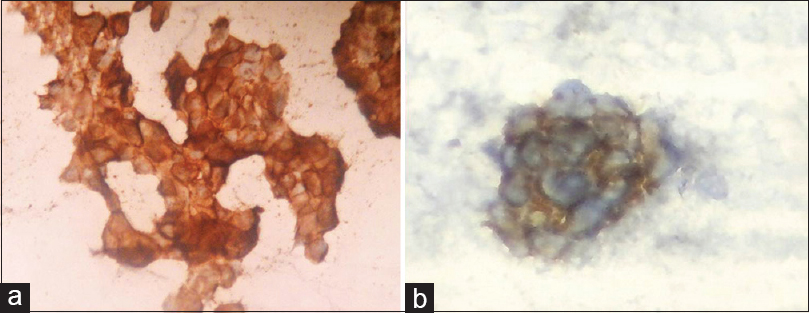
- (a) Immunocytochemistry photomicrograph of breast carcinoma shows complete cytoplasmic membrane staining for human epidermal growth factor/neu–score-3+ (×10), (b) human epidermal growth factor/neu–score-3+ (×40)

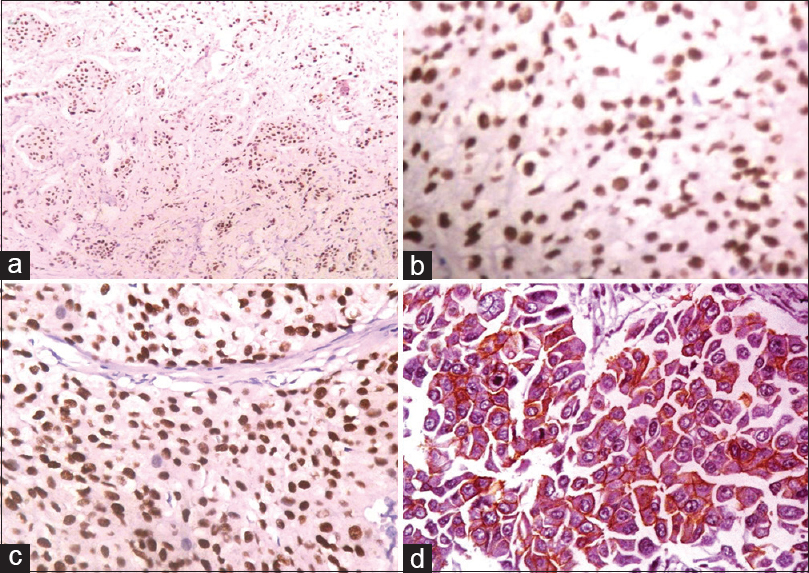
- (a) Immunohistochemistry nuclear stain positivity for estrogen receptor – Allred score-8 (×10), (b) immunohistochemistry nuclear stain positivity for estrogen receptor-Allred score-8 (×40), (c) immunohistochemistry nuclear stain positivity for progesterone receptor-Allred score-8 (×40), (d) immunohistochemistry nuclear stain positivity for human epidermal growth factor/neu receptor-score-3+ (×40)
The immunocytochemical results were then compared with those of IHC of the corresponding excised surgical specimens (gold standard). By ICC, ER-positive expression was seen in 53/100 (53%) of cases and rest 47/100 (47%) were negative. Among 53/100 (53%) ICC positive cases of ER, all were positive by IHC (true positives). Of 47/100 (47%) ICC negative cases, 45 were negative (true negatives) by IHC and 2 were positive (false negative) by IHC. Compared to IHC, the ICC diagnostic sensitivity, specificity, PPV, and NPV for ER staining were 96.3%, 100%, 100%, and 95.7%, respectively. The overall accuracy and concordance between ICC and IHC were 98% [Table 3].

PR ICC positive cases were 50/100 (50%) and rest 50/100 (50%) were negative. Among fifty ICC positive cases of PR, all fifty were positive by IHC (true positive). In rest 50 ICC negative cases, 47 were negative (true negatives) by IHC and 3 were positive (false negatives) by IHC. The diagnostic sensitivity, specificity, PPV, and NPV for PR immunocytochemical staining were 94.3%, 100%, 100%, and 94%, respectively. The concordance between ICC and IHC was 97% [Table 3].
Of the 100 cases, only 92 cases of Her2/neu were suitable for the study. Among which ICC positive cases were 21/92 (22.8%) and negative cases were 71/92 (77.1%). Among the 21 Her2/neu receptor immunocytochemical positive cases, 18 cases were positive by IHC (true positive) and three cases were negative by IHC (false positives). Of 71 ICC Her2/neu receptor negative cases, 64 cases were negative by IHC (true negative) and 7 cases were positive by IHC (false negatives). In comparison to IHC, the diagnostic sensitivity, specificity, PPV, and NPV for Her2/neu receptor immunocytochemical staining were 72%, 95.5%, 85.7%, and 90.1%, respectively, and the concordance being 89% [Table 3].
DISCUSSION
The incidence of breast carcinoma rises throughout a woman's lifetime. Age range among Indian breast cancer patients is found to be lower when compared to the Western countries with an average difference of one decade. This is likely to be due to the different age distribution of the Indian population, where only 7% of the population is above the age of 60 years.[101112] In the present study, 49% of women were in the age group of 41–50 years, in contrast a study by Pakseresht et al.[13] had lower age range from 31 to 40 years (34.5%), whereas Suvarchala and Nageshwararao[11](45.31%) and Ambroise et al.[12](46.4%) had higher age range between 51 and 60 years.
Literature search reveals breast carcinomas are more common in the left breast than the right side. The possible explanations are that the left breast being more bulky and having larger volume of breast tissue comparatively. However, side of breast involved has no clinical significance.[1415] In the present study also left breast was marginally more affected than right with a single case of bilateral breast carcinoma.
Analysis of steroid receptor status has become the standard of care for patients with breast cancer. Traditional factor such as detection of the presence or absence of ER, PR, and Her2/neu in breast carcinoma is known to be clinically essential for determining the responsiveness to the endocrine therapy and predicting prognosis in newly diagnosed and relapsed breast carcinoma.[111214] These factors can be assessed on the FNAC aspirates by the procedure called as ICC which is a well-accepted procedure for determining ER, PR, and Her2/neu. In both ICC as well as IHC, the crucial steps involved are fixation and antigen retrieval.[6789]
Some authors evaluated the hormone receptor status using the immunocytochemical technique on archived Papanicolaou and H and E stained fine-needle aspiration slides and concluded that Papanicolaou-stained slides used as such, without destaining for ICC showed better agreement with IHC than the destained slides. While others reported that using Papanicolaou and H and E stained slides for ICC without destaining but with antigen retrieval showed a much better agreement with IHC than destained slides. The explanation being that harsh destaining techniques results in the loss of receptor antigenicity. However, other authors assessed the hormone receptor status on cytological smears using destained slides and achieved good results. Considering the reasons, we chose to do ICC on H and E destained slides and also opine that prior staining will help in checking the adequacy of the material.[6789161718] Identifying suitable fixative and processing conditions for the preservation of the antigen required are of prime importance in determining ER, PR, and Her2/neu immunoreactivity. The fixatives commonly used are freshly prepared 4% buffered formalin, cold acetone, ether alcohol, Carnoy's fixative, and combination of methanol and acetone all of which have to be freshly.[6789161718] In the present study, we used cold acetone as a fixative and yielded us with better results.
Antigen retrieval is another crucial step in the documentation of receptors in breast carcinoma. However, antigen retrieval can be performed by pressure cooker heating or microwave. Many Indian authors have suggested using a pressure cooker for heating compared to a microwave on account of financial constraints although microwave heating is proved to give better results in the West in the presence study to, we used pressure cooker since it was well established in our laboratory and yielded good results.[6789161718] The retrieval buffers which can be used are 0.9 M Tris-HCl buffer, sodium citrate, and ethylenediaminetetraacetic acid (EDTA). Among them, EDTA has been proved to be a superior antigen retrieval solution; hence, the same was used in the presence study.[6789161718]
For reporting purposes, Allred scoring[19] for ER, PR receptor, and CAP protocol Her2/neu scoring[20] was used in the present study and totally 100 cases were studied for both ICC and IHC correlation.
In the present study, ICC was positive for ER, PR, and Her2/neu in 53%, 50%, and 23.9% of cases, respectively. The sensitivity, specificity, PPV, and NPV results for ER and PR receptor ICC expression of the present study were similar to the Western studies[6716] and higher compared to a study by Radhika and Prayaga.[8] However, lower results by Radhika and Prayaga[8] were explained by the author as due to the use of improper antigen retrieval [Tables 4 and 5].


Very few studies are found in the literature which uses Her2/neu for ICC and IHC correlation. In the present study, Her2/neu sensitivity was 72%, specificity 95.5%, PPV and NPV were 85.7% and 90.1%. Concordance being 89% the present study concordance rates were equal to the other studies.[212223] However, other authors have compared ICC with fluorescence in situ hybridization (FISH) and found FISH to be a most powerful technique for Her2/neu evaluation on breast carcinoma[2324] [Table 6].

CONCLUSION
ICC has been a boon and can be a paramount diagnostic adjunct to the routine investigations. Identifying suitable fixative and antigen retrieval processing is of fundamental importance. ICC on FNA has a rapid turnaround time with minimal processing time and antigen loss due to fixation. ICC on FNA helps in sequential receptor status determinations at different times during the course of treatment and also in the evaluation of metastatic tumors of unknown origin without the need of invasive open surgical biopsy. ICC is more advantageous in planning treatment for patients for whom surgery would be contraindicated because of elderly patients, advanced inoperable tumor, metastases, local disease recurrence, or malignant effusions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- National Cancer Registry Programme, Indian Council of Medical Research. Leading Sites of Cancer. In: Consolidated Report of Population Based Cancer Registries 2001-2004, Incidence and Distribution of Cancer. Bangalore: Coordinating Unit, National Cancer Registry Programme(ICMR); 2006. p. :8-30.
- [Google Scholar]
- The magnitude of cancer breast in India: A summary. Indian J Surg Oncol. 2010;1:8-9.
- [Google Scholar]
- Replace fine needle aspiration cytology with automated core biopsy in the triple assessment of breast cancer. Ann R Coll Surg Engl. 2001;83:110-2.
- [Google Scholar]
- Status of HER-2/neu receptors and Ki-67 in breast cancer of Indian women. Int J Appl Basic Med Res. 2011;1:15-9.
- [Google Scholar]
- Hormone receptors over the last 8 years in a cancer referral center in India: What was and what is? Indian J Pathol Microbiol. 2009;52:171-4.
- [Google Scholar]
- Assessment of the reliability of immunocytochemical detection of estrogen and progesterone receptors status on the cytological aspirates of breast carcinoma. J Egypt Natl Canc Inst. 2010;22:217-25.
- [Google Scholar]
- Comparison of the results of immunocytochemical assays for biologic variables on preoperative fine-needle aspirates and on surgical specimens of primary breast carcinomas. Cancer. 2000;90:61-6.
- [Google Scholar]
- Estrogen and progesterone hormone receptor status in breast carcinoma: Comparison of immunocytochemistry and immunohistochemistry. Indian J Cancer. 2010;47:148-50.
- [Google Scholar]
- Immunocytochemistry on scrape cytology in breast cancer: Will it unearth the weaker positives? Acta Cytol. 2006;50:284-90.
- [Google Scholar]
- Estrogen, progesterone and HER2 receptor expression in breast tumors of patients, and their usage of HER2-targeted therapy, in a tertiary care centre in India. Indian J Cancer. 2011;48:391-6.
- [Google Scholar]
- Carcinoma breast-histopathological and hormone receptors correlation. J Biosci Technol. 2011;2:340-8.
- [Google Scholar]
- Immunohistochemical profile of breast cancer patients at a tertiary care hospital in South India. Asian Pac J Cancer Prev. 2011;12:625-9.
- [Google Scholar]
- Risk factors with breast cancer among women in Delhi. Indian J Cancer. 2009;46:132-8.
- [Google Scholar]
- Comparison of ER, PR and HER-2/neu (C-erb B 2) reactivity pattern with histologic grade, tumor size and lymph node status in breast cancer. Asian Pac J Cancer Prev. 2008;9:553-6.
- [Google Scholar]
- Profile of breast cancer patients at a tertiary care hospital in North India. Indian J Cancer. 2010;47:16-22.
- [Google Scholar]
- Correlation of immunocytochemical and immunohistochemical determination of estrogen and progesterone receptors in breast cancer. Acta Cytol. 2002;46:337-40.
- [Google Scholar]
- Immunocytochemical evaluation of estrogen receptor on archival Papanicolaou-stained fine-needle aspirate smears. Diagn Cytopathol. 2003;29:309-14.
- [Google Scholar]
- Optimal fixation conditions for immunocytochemical analysis of estrogen receptor in cytologic specimens of breast carcinoma. Cancer. 2004;102:34-40.
- [Google Scholar]
- ASCO-CAP guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010;28:2784-95.
- [Google Scholar]
- American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25:118-45.
- [Google Scholar]
- Hormone receptor status and HER2/neu overexpression determined by automated immunostainer on routinely fixed cytologic specimens from breast carcinoma: Correlation with histologic sections determinations and diagnostic pitfalls. Diagn Cytopathol. 2004;30:251-6.
- [Google Scholar]
- Immunocytochemical evaluation of HER-2/neu on fine-needle aspirates from primary breast carcinomas. Diagn Cytopathol. 2003;28:142-6.
- [Google Scholar]
- HER-2/neu detection in fine-needle aspirates of breast cancer: Fluorescence in situ hybridization and immunocytochemical analysis. Am J Clin Pathol. 2004;122:246-55.
- [Google Scholar]
- Her-2 neu (Cerb-B2) expression in fine needle aspiration samples of breast carcinoma: A pilot study comparing FISH, CISH and immunocytochemistry. J Cytol. 2011;28:54-6.
- [Google Scholar]



