
Translate this page into:
Cytodiagnosis of Epidermoid Cyst of the Upper Lip: A Common Lesion in an Uncommon Site
Address for correspondence: Dr. Jyoti Prakash Phukan, E-mail: drjyotiphukan@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Epidermoid cyst and dermoid cysts are developmental pathologies thought to derive from aberrant ectodermal tissue. They are uncommon in the head and neck region. Rarely, they can be found in the oral cavity and buccal mucosa. However, epidermoid cyst is extremely uncommon in the upper lip and is rarely reported. In this study, we report an uncommon case of epidermoid cyst occurring in the upper lip diagnosed by fine-needle aspiration cytology (FNAC). We present this case because of its extremely rare site of presentation and also to highlight the role of FNAC to in the pre-operative diagnosis of this benign lesion.
Keywords
Dermoid cyst
epidermoid cyst
fine-needle aspiration cytology

INTRODUCTION
Epidermoid and dermoid cysts are benign lesions encountered throughout the body that are derived from abnormally situated ectodermal tissue. Histologically, epidermoid cyst is a cyst lined by stratified squamous epithelium and lumen is filled with lamellated keratin while dermoid cyst contains skin adnexal structures in the cyst wall. Epidermoid cysts are uncommon in the head and neck region, occurring about 7% in this region and 1.6% within the oral cavity.[1] Within the oral cavity, the most common sites includes submandibular, sublingual and submental region.[23] Rare cases have been reported from tongue, uvula, intraosseously within mandible and maxilla and palatine tonsil.[456] However, epidermoid cyst occurring in the upper lip is very uncommon and rarely reported in English literature.[7] We intend to present a case of epidermoid cyst of the upper lip, which was diagnosed by fine-needle aspiration cytology (FNAC) and subsequently confirmed by histopathology.
CASE REPORT
A 52-year-old male attended FNAC clinic of our hospital with a globular swelling in the upper lip [Figure 1]. The swelling was present for last 5 years and gradually increasing in size. It was not associated with pain. On physical examination, the size of the swelling was approximately 2.5 cm × 1 cm, cystic, non-tender and soft in consistency. No associated cervical lymphadenopathy was detected.

- External clinical photograph. Cystic mass in the upper lip
With a clinical diagnosis of mucocele, fine needle aspiration was performed using a 22 gauge needle. Aspiration yielded pultaceous material and the smears were stained with May-Grünwald Giemsa stain. Cytological smears showed many anucleated squames and few benign mature squamous cells in a dirty background [Figure 2]. A cytological diagnosis of epidermoid cyst was made with a recommendation for excision of the swelling and histopathological examination.
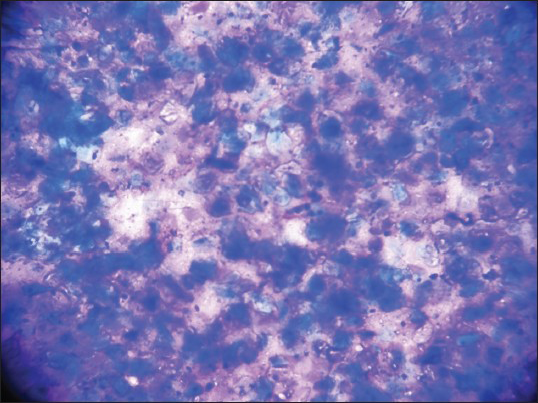
- Fine-needle aspiration cytology showing many anucleated squames and few benign nucleated squamous cells in a dirty background (May-Grünwald-Giemsa, ×100)
Excision biopsy and histopathological examination of the resected specimen showed a cyst lined by stratified squamous epithelium filled with lamellated keratin [Figure 3]. No skin appendages seen. Thus, hispathological diagnosis of epidermoid cyst was confirmed.
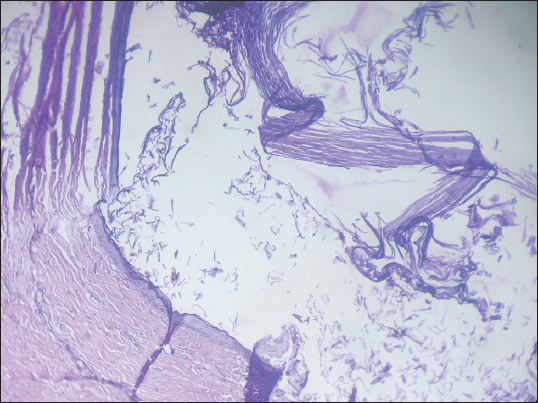
- Histopathological section showing a cyst lined by keratinized squamous epithelium, cavity filled with lamellated keratin. No skin appendages seen (H and E, ×100)
DISCUSSION
Histologically Meyer divided the cysts of the floor of mouth into three categories: Epidermoid cysts, true dermoid cysts and teratoid cysts.[8] In the epidermoid cysts, the cyst cavity is lined by squamous epithelium without skin appendages, while the true dermoid cyst contains skin appendages such as hair, hair follicles, sebaceous and sweat glands etc., Cyst is defined as teratoid when in addition to skin appendages other tissuessuch as muscle, bone, cartilage etc., are present. Although typical dermoid cyst is a distinct entity, all above mentioned three types of cysts generally mentioned as dermoid cyst. The most common sites of dermoid are ovaries and testicles (80%), with head and neck accounting for only 7%.[12] Epidermoid and dermoid cysts are uncommon in the mouth and comprises less than 0.01% of all the oral cysts.[9]
Epidermoid cysts can be classified as congenital or acquired; however clinical presentation or histology of both types is similar. The exact etiology of these cystsis unknown and many etiopathological theories have been proposed. Congenital cysts are dysembryogenetic lesions that arise from ectodermal elements entrapped during the midline fusion of the first and second branchial arches between the 3rd and 4th weeks of intrauterine life.[10] Acquired epidermoid cysts occur due to traumatic or iatragenic implantation of epithelium or occlusion of a sebaceous duct.
Dermoid cysts are usually diagnosed in young adults in the second and third decades of life.[11] In our case, however the age of the patient is 52 years. Hence, it may arise due to traumatic implantation of the epithelium.
As epidermoid cysts are quite rare in the upper lip, correct clinical diagnosis is usually not possible. The most common clinical differential diagnosis of cystic lip mass is mucocele as in our case. Lip contains adipose tissue, connective tissue, blood vessels, nerves and salivary glands; so that any lesion that may originate from these components may occur in lips. Other clinical differential diagnosis of lipmass include fibroma, lipoma, mucous retention cyst, sialolith, phlebolith and salivary gland neoplasms.[12] Fibromas are nodular lesions that can be initiated by trauma. They are the most common intraoral soft-tissue lesion and are seen most frequently in lips.[13] Lipomas are the benign tumour of adipose tissue. Lipomas are uncommon in the oral cavity, but may involve lips.[13] Clinically they are soft, mobile and fluctuation may be present, which may give a cystic consistency. Mucous retention cyst usually occurs in older age group. They most commonly involve the upper lip. Sialolith may also present as the upper lip mass, however they are usually firm not cystic. Rarely phleboliths, which occurs due to calcification of intravascular thrombi may present as lipmass. Various salivary gland pathologies ranging from salivary gland cysts, benign salivary gland neoplasmssuch as canalicular adenoma, pleomorphic adenoma to malignant neoplasmssuch as mucoepidermoid carcinoma, acinic cell carcinoma etc., may occur in lip.[13] Vascular malformationssuch as hemangiomas and varices may also be considered in the differential diagnosis of lip mass in children. They are usually blue in colour and blench in pressure, which differentiates it from mucoceles.
FNAC of epidermoid cyst usually show debris with mature squamous cells with anucleate squames. Inflammatory cells and foreign body giant cells may also be found. The cytological differential diagnosis of epidermoid cyst includes trichilemmal cyst and dermoid cyst.[14] The three cysts are cytologically quite similar. The characteristic abrupt transition from basaloid squamous epithelial cells to keratinized globules can be rarely seen in fine-needleaspiration smears of trichilemmal cysts. Hair shafts can be present in aspiration of dermoid cyst in addition to mature squamous cells and anucleate squames. Histopathologic examination provides the correct diagnosis and shows a cyst cavity lined by squamous epithelium and filled with lamellated keratin. No skin adenexal structures are identified. Giant cells may also be present in some cases.
We have presented this case because of the rare site of presentation of epidermoid cyst in the upper lip. We also want to highlight the role of FNAC in the diagnosis of this simple benign lesion from any site, which is easily accessible. Patient presented with a cystic mass in the upper lip from where fine-needle aspiration was easily done, which gives a correct pre-operative diagnosis.
Finally, we recommend FNAC from any accessible mass, because it is cheap, easy to perform and gives a correct diagnosis in most of the cases.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Case report: Epidermoid cyst of the floor of the mouth: Diagnostic imaging by sonography, computed tomography and magnetic resonance imaging. Br J Radiol. 1995;68:205-7.
- [Google Scholar]
- Epidermoid cyst in the floor of the mouth: Report of a case. Quintessence Int. 2007;38:473-7.
- [Google Scholar]
- Epidermoid cyst of the buccal mucosa: A case report. J Contemp Dent Pract. 2007;8:90-6.
- [Google Scholar]
- Epidermoid cyst of the buccal mucosa. Oral Surg Oral Med Oral Pathol. 1989;67:181-4.
- [Google Scholar]
- Epidermoid cyst of the uvula: Report of a case. J Oral Maxillofac Surg. 1986;44:828-9.
- [Google Scholar]
- Epidermoid cyst localized in the palatine tonsil. J Oral Maxillofac Pathol. 2013;17:148.
- [Google Scholar]
- The sublingualdermoid cyst. Report of five cases and review of the literature. Oral Surg Oral Med Oral Pathol. 1985;59:578-80.
- [Google Scholar]
- Midline (dermoid) cysts of the floor of the mouth: Report of 16 cases and review of surgical techniques. Plast Reconstr Surg. 2003;112:1560-5.
- [Google Scholar]
- The canalicular adenoma: Considerations on differential diagnosis and treatment. J Oral Maxillofac Surg. 1984;42:728-30.
- [Google Scholar]
- Mucocele of the upper lip: Case report of an uncommon presentation and its differential diagnosis. J Can Dent Assoc. 2004;70:318-21.
- [Google Scholar]
- Skin and subcutis. In: Orell SR, Sterrett GF, Whitaker D, eds. Fine Needle Aspiration Cytology (4th ed). New Delhi: Elsevier Limited; 2005. p. :395.
- [Google Scholar]



