
Translate this page into:
Enterobius vermicularis infestation leading to Meckel's diverticulitis in an adolescent boy: An extremely rare presentation
Address for correspondence: Dr. Manupriya Sharma, Set No. 112, Vivekanand Hostel, Dr. RPGMC, Kangra, Tanda - 176 001, Himachal Pradesh, India. E-mail: manupriya.priyasharma@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Enterobius vermicularis is an intestinal nematode commonly affecting children worldwide. Its transmission is by feco-oral route. Meckel's diverticulitis due to E. vermicularis infestation is an extremely rare presentation. An 11-year-old boy presented with acute abdomen. During surgery inflamed Meckel's diverticulum (M.D) was seen. Histopathology examination of specimen revealed E. vermicularis. Till date, only one case of E. vermicularis infestation of M.D is reported around five decades ago. This histopathological confirmation is extremely important as the required treatment (Mebendazole) of the infected case along with household contacts can prevent the spread of infection and may avoid surgery in known contacts.
Keywords
Children
Enterobius vermicularis
Meckel's diverticulitis

Introduction
Enterobius vermicularis (pinworm) is an intestinal nematode affecting children worldwide. It is transmitted through feco-oral route. Following ingestion, the embryonated eggs hatch in small intestine, develop into adult worms and reside in the caecum, appendix, colon, and rectum. Adult worms mate in intestinal tract and gravid female worm lays eggs at night leading to nocturnal pruritus caused by an irritant mucous; shed with the eggs by the female.[1]
Meckel's diverticulum (M.D) is the most common congenital abnormality of the small intestine, presenting in 1%–4% of the general population. It is a remnant of the vitellointestinal duct which arises as a true diverticulum from the antimesenteric border of terminal ileum.[2] We hereby report a case of Meckel's diverticulitis due to E. vermicularis infestation.
Case Report
An 11-year-old boy presented to emergency with complaints of acute pain abdomen for the last 1 day. The pain was sudden in onset and severe in intensity. There were two episodes of vomiting in last 24 h. There were no urinary or bowel complaints. On examination, there was tachycardia (pulse rate 96/min), low-grade fever (38.6°C) and tenderness in the right iliac fossa. Emergency ultrasonography revealed probe tenderness at Mcburney's point along with inflamed gut loops in infraumbilical region. The patient was planned for emergency laparotomy with a provisional diagnosis of acute appendicitis. Intraoperatively, appendix measured 8 cm in length with congested serosal aspect. On further exploration, inflamed M.D was found measuring 6 cm in length, approximately two feet from ileocaecal junction. Meckel's diverticulectomy along with appendicectomy was done.
Laboratory investigations
Emergency investigations revealed leukocytosis (11.8 × 109/L). Absolute eosinophil count was 1.3 × 109/L. Histopathological examination of appendiceal lumen had E. vermicularis infestation [Figure 1a]. M.D showed ulceration of the lining epithelium with trans-mural inflammation and necrosis [Figure 1b]. E. vermicularis ova were seen in wall of M.D [Figure 1b]. However, no adult worm was identified in the sections examined from M.D. Multiple sections from M.D were examined to rule out any heterotopic tissue. No worms/eggs or cysts were identified in stool examination or after the application of a transparent adhesive tape to the perianal area. The index case was treated with mebendazole 100 mg twice a day for 3 days. This course was repeated after 2 weeks. All the family members were also given empirical treatment for the infection.
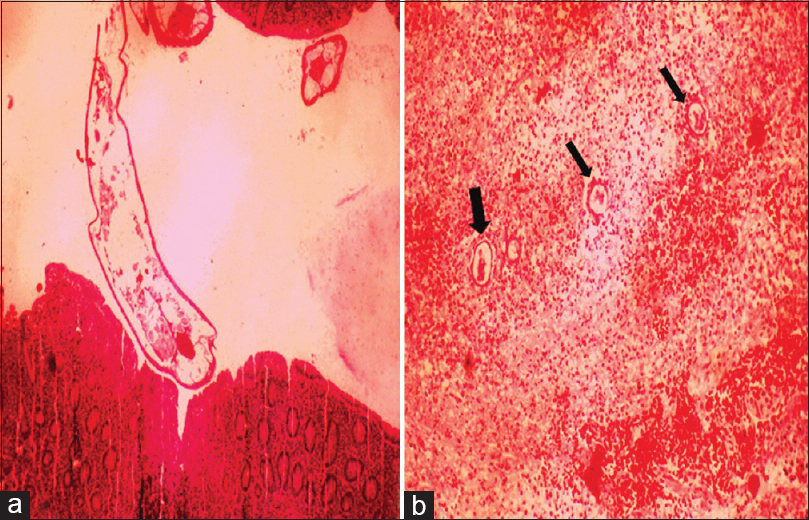
- (a) Appendix lumen showing adult worms of Enterobious vermicularis. (b) Meckel's Diverticulum with ova of Enterobious vermicularis and transmural necrosis and inflammation
The patient is on regular follow-up and is asymptomatic till date. Repeat stool examination was normal.
Discussion
Fabricus Hildanus described the appendiceal pinworm for the first time in 1634.[34] Since then, E. vermicularis is known as one of the most common intestinal nematode. The organism occurs more frequently in temperate and cold climates. Children are especially susceptible to the infection. The infection is transmitted by feco-oral route. Infrequent bathing, use of soiled underwears, crowded habitation, and lack of exposure to sunlight all favor disease transmission. E. vermicularis in the appendix is usually an innocent bystander and does not elicit an inflammatory response as seen in the particular case. E. vermicularis has rarely been reported at ectopic sites such as genitourinary tract, kidney, and eye.[345]
M.D is usually asymptomatic and detected incidentally during laparotomy. About 4%–6% of cases can have symptomatic presentation in the form of intestinal obstruction, bleeding, diverticulitis, and perforation. Meckel's diverticulitis with E. vermicularis infestation is an extremely rare clinical presentation. To the best of our knowledge, there is one case report of E. vermicularis infestation of the M.D five decades back.[6] Tseng and Yang reviewed clinical and diagnostic characteristics of M.D from 1988 to 2008. There were a total of 47 children and characterized as follows: bleeding (n = 21), obstruction (n = 12), diverticulitis (n = 12), and two diagnosed incidentally.[7] No case of parasitic infestation of M.D was found. No protective immunity against E. vermicularis infection develops, and re-infection is common. Environmental contamination with infective eggs is seen, so testing/treatment of household contacts should be considered. According to Centers for Disease Control and Prevention guidelines treatment of E. vermicularis is mebendazole 100 mg orally to be repeated after 2 weeks or pyrantel pamoate, given at a dose of 11 mg/kg body weight (to be repeated after 2 weeks).[8] This case was treated with mebendazole 100 mg twice a day for 3 days. This course was repeated after 2 weeks. Family members were treated empirically for the infection. General instructions for maintenance of adequate cleanliness and hygiene such as washing hands properly with soap and warm water after using the toilet, changing diapers, or before handling food items were given.
Conclusion
We report an extremely rare manifestation of E. vermicularis infection presenting as Meckel's diverticulitis. The identification of underlying pathology of Meckel's Diverticulitis as E. vermicularis infection is important as timely treatment of infected case and testing/treatment or recommendations of environmental cleaning can prevent reinfection or spread of infection to other household contacts and may ultimately avoid surgical intervention in family members too.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Enterobius vermicularis in a 14-year-old girl's eye. J Clin Microbiol. 2011;49:4369-70.
- [Google Scholar]
- Meckel diverticulum: The Mayo Clinic experience with 1476 patients (1950-2002) Ann Surg. 2005;241:529-33.
- [Google Scholar]
- Enterobius vermicularis in the kidney: An unusual location. J Med Microbiol. 2010;59:860-1.
- [Google Scholar]
- Assessment of frequency, transmission, and genitourinary complications of enterobiasis (pinworms) Int J Dermatol. 2005;44:837-40.
- [Google Scholar]
- Topical anthelmintic treatment of recurrent genitourinary enterobiasis. Genitourin Med. 1989;65:284-5.
- [Google Scholar]
- Acute appendicitis and a Meckel's diverticulum with Enterobius vermicularis. First reported case. Am Surg. 1966;32:343-6.
- [Google Scholar]
- Clinical and diagnostic relevance of Meckel's diverticulum in children. Eur J Pediatr. 2009;168:1519-23.
- [Google Scholar]
- The Medical Letter on Drugs and Therapeutics. In: Drugs for Parasitic Infections. New Rochelle, NY: The Medical Letter, Inc; 2010.
- [Google Scholar]



