
Translate this page into:
Evaluation of the effectiveness of critical result notification protocol of biochemistry laboratory at a tertiary care hospital
*Corresponding author: Silpa Thota, MBBS, MD, Department of Biochemistry, Sri Venkateswara Institute of Medical Sciences, Tirupati 517507, Andhra Pradesh, India silpa.thota@yahoo.co.in
-
Received: ,
Accepted: ,
How to cite this article: Thota S, Bitla AR. Evaluation of the effectiveness of critical result notification protocol of biochemistry laboratory at a tertiary care hospital. J Lab Physicians. 2024;16:26-35. doi: 10.1055/s-0043-1775573
Abstract
Objectives:
Critical value reporting is an essential aspect of laboratory medicine, ensuring prompt communication of life-threatening results to clinicians for immediate action. Existing guidelines emphasize the importance of timely notification, but protocols may vary. This study evaluated the effectiveness of the protocol for reporting critical results in the biochemistry laboratory of a tertiary care hospital and proposed alternative protocols for improvement.
Materials and Methods:
Data were collected over a 6-month period, including the total number of investigations, critical values detected, parameters analyzed, and clinical departments involved. Quality indicators such as turnaround time (TAT), unsuccessful reporting rates, and clinical actions taken were assessed. Statistical analysis was performed using Microsoft Excel.
Statistical Analysis:
All statistical analyses were performed using Microsoft Excel spreadsheets (Microsoft, Redmond, WA, United States). Data were presented as numbers and percentages.
Results:
Out of 390,000 investigations, 0.5% had critical values. Serum potassium (55.9%) had the highest frequency of critical values, followed by sodium, calcium, and glucose. The emergency department received the highest number of critical alerts. The success rate of critical result reporting within 1 hour was 86.8%, while unsuccessful reporting accounted for 10.7%. The causes of unsuccessful reporting included outpatient requests and delayed intimation due to patient transfers. Corrective action was taken in 91% of cases, with documentation primarily in nurse charts.
Conclusion:
Evaluation of the protocol for reporting critical results identified areas for improvement. Recommendations included revising the critical value list, reducing TAT through process optimization and automation, enhancing staff training and awareness, fostering interdisciplinary collaboration, and maintaining incident records. Implementing these changes can enhance compliance, reduce errors, and improve patient care.
Keywords
clinical decision-making
critical value
laboratory communication systems
turnaround time

INTRODUCTION
A critical value is defined as “a laboratory test result that represents a pathophysiologic state at such variance with normal as to be life-threatening unless something is done promptly and for which some corrective action could be aken.”[1] The concept of a critical value system was first created and implemented at the Los Angeles County-USC Medical Centre in 1971.[1] This system requires that laboratory personnel identify a critical value and after validation ensure that it is communicated to the clinician so that appropriate action is taken. After its initial implementation in the laboratories in the United States, it soon found a place as one of the accreditation requirements.[2] Various professional bodies have published guidelines and recommendations for the harmonization of critical risk results and their communication.[3,4] The current laboratory accrediting agencies also recommend critical value reporting as one of the requirements for accreditation. The guidelines issued by International Organization for Standardization (ISO) 15189 mention immediate reporting of critical values as a standard of Good Laboratory Practice.[5] Our national laboratory accreditation body, that is, the National Accreditation Board for Testing and Calibration Laboratories (NABL), India, also mentions critical value reporting as mandatory under the NABL 112 document clause 5.9.[6] Timely notification of critical results to the clinician will ensure appropriate timely action, which can help in decreasing morbidity and mortality. Existing guidelines of the professional bodies including the Joint Commission (JC), Royal College of Pathologists (RCP), Clinical and Laboratory Standards Institute (CLSI), and Italian Society of Clinical Biochemistry and Laboratory Medicine/Italian Society of Laboratory Medicine (SIBIOC-SIMEL) emphasize the importance of timely notification of critical laboratory values, with consensus that such values should be communicated immediately or within 1 hour from their identification. However, it is important to note that specific turnaround time (TAT) goals may vary depending on the laboratory test and clinical context. Therefore, laboratories should establish their own TAT goals based on their performance data and clinical needs to ensure high-quality patient care.[7]
In the present study, we analyzed the protocol for reporting critical alerts in the biochemistry laboratory of a tertiary care hospital and compared it with similar studies in the literature. Our study aimed to evaluate the protocol of telephonic notification of critical values at our tertiary care teaching hospital in terms of TAT, rates, efficiency, and use of these notifications in clinical decision-making and based on the findings of our study suggest alternative protocols for improving compliance.
MATERIAL AND METHODS
This study was conducted in the clinical laboratory of the Department of Biochemistry at Sri Venkateswara Institute of Medical Sciences (SVIMS), Tirupati, Andhra Pradesh, from December 2021 to May 2022 for a period of 6 months after receiving approval from the Institutional Ethics Committee (IEC no. 1232 dated October 27, 2021). The protocol of telephonic notification of critical results introduced in 2016 and being currently followed was evaluated. The parameters for which critical results are reported in our clinical biochemistry laboratory and their critical limits arrived at are based on inputs from the clinicians. The critical alert notification protocol is the same for routine tests and short turnaround time laboratory analyses.
In brief, the critical values obtained for the defined parameter were confirmed by repetition after ruling out preanalytical interferences (hemolysis, diluted sample, sample contamination with anticoagulant, etc.). Then, the results were immediately notified to the clinician/resident/nursing staff available in the ward based on the information available in the request form of the patient by calling the intercom number. Readback of results was ensured to avoid errors due to miscommunication. The name of the person to whom the result was notified was enquired and the same was noted down along with other details like date, patient name, age, gender, ward, parameter, time of sample received in the laboratory, time of critical value reported in the laboratory, and time of critical value intimated in the critical value register. The efficiency of the notification protocol was assessed by employing the following quality indicator metrics[8,9]:
Table 1 shows the critical results analyzing metrics and formulae.
Percentage of critical values reported for the total number of test results performed during the study period.
Time required for notification or the TAT. TAT was defined as the period between the time of critical value reported in the laboratory and the time critical value intimated to the concerned doctor/nursing staff.
The percentage of unsuccessful reporting of results (defined as the inability to report the critical values after several failed attempts).
Document the causes of the unsuccessful attempts.
Percentage of cases wherein appropriate intervention was taken by the treating team upon receipt of the critical results (defined as the number of cases wherein appropriate intervention was taken by the treating team upon receiving of critical results, which are measured by manually verifying the patients’ case records within 1 week of intimation of critical result).
| Metric | Formula |
|---|---|
| % of critical results of each parameter | (No. of critical results reported/no. of tests done) × 100 |
| % of critical results relative to all critical results | (No. of critical results/total no. of critical results) × 100 |
| % of unsuccessful reporting of critical results | (No. of critical results that could not be notified/total no. of critical values) × 100 |
Statistical Analysis
All statistical analyses were performed using Microsoft Excel spreadsheets (Microsoft, Redmond, WA, United States). Data were presented as numbers and percentages. The number of cases wherein appropriate intervention was taken by the treating team upon receipt of the critical results was calculated for 100 cases.[8] These cases were selected from successfully intimated critical results and were done by random number selection through Microsoft Excel. A comparison of the data obtained was made with the values obtained from other centers.
RESULTS
During the 6-month study period, our biochemistry laboratory performed approximately 390,000 investigations, out of which 190,000 investigations were from outpatient testing and 200,000 investigations from inpatient testing. In the same period, the number of critical values detected was 1,963, which was approximately 0.5% of the total number of investigations performed.
The list of critical value limits used in our laboratory at the time of the study is presented in Table 2. In our laboratory, these limits were established by a team comprising clinicians and laboratory medicine specialists. The frequency of critical values was calculated for each parameter, as shown in Table 3. The parameter with the highest percentage of all critical values was serum potassium (55.9%), followed by serum sodium (19.3%), serum calcium (15.7%), and plasma glucose (1.7%).
| Parameters | Lower critical values limit | Upper critical values limit |
|---|---|---|
| Plasma glucose | ≤40 mg/dL | ≥450 mg/dL |
| Serum calcium | ≤8.0 mg/dL | ≥11.0 mg/dL |
| Serum magnesium | ≤1.0 mg/dL | ≥9.0 mg/dL |
| Serum total bilirubin | ≥15 mg/dL | |
| Serum sodium | ≤120 mmol/L | ≥150 mmol/L |
| Serum potassium | ≤3.0 mmol/L | ≥5.5 mmol/L |
| Serum creatinine | ≥8 mg/dL | |
| Serum osmolality | ≤250 mOsm/kg | ≥325 mOsm/kg |
| Toxic drug levels | ||
| Serum total carbamazepine | ≥15 μg/mL | |
| Serum total phenobarbitone | ≥50 μg/mL | |
| Serum total phenytoin | ≥30 μg/mL |
| Parameters | N test results | N critical values | % critical values | % of all critical values |
|---|---|---|---|---|
| Serum total bilirubin | 29,057 | 11 | 0.04 | 0.6 |
| Serum calcium | 9,388 | 309 | 3.29 | 15.7 |
| Serum creatinine | 65,583 | 118 | 0.18 | 6 |
| Plasma glucose | 31,466 | 35 | 0.11 | 1.7 |
| Serum magnesium | 3,718 | 1 | 0.03 | 0.05 |
| Serum potassium | 57,690 | 1099 | 1.91 | 55.9 |
| Serum sodium | 47,367 | 379 | 0.80 | 19.3 |
| Serum osmolality | 369 | 2 | 0.54 | 0.1 |
| Serum total phenytoin | 15 | 6 | 40.00 | 0.3 |
| Serum total phenobarbitone | 4 | 2 | 50.00 | 0.1 |
| Serum total carbamazepine | 6 | 1 | 16.67 | 0.05 |
Notes: N test results: total number of tests performed by the clinical laboratory in 6 months.
N critical values: total number of critical values reported in 6 months (1,963).
% critical values: percentages of critical values concerning the number of test results for each parameter.
% of all critical values: percentages of critical values for all critical values.
The number of critical values reported in each clinical department in the 6-month period is depicted in Figure 1. The emergency department was the requesting department that received the maximum number of the calls from the clinical laboratory for critical alert notification (596, 30.4%), followed by nephrology (318, 16.2%), medicine (274, 14%), and intensive care unit (ICU; 194, 9.9%). These four departments accounted for about 70.5% of all critical alerts in the biochemistry laboratory. The successful and unsuccessful critical alert intimation is represented in Table 4. The percentage of successful reporting of critical results, which was within 1 hour of TAT, was approximately 86.8% (N = 1,703), whereas 2.5% (N = 50) of critical alerts were intimated to the concerned person in greater than 1 hour of TAT, and the percentage of unsuccessful reporting of critical results was 10.7% (N = 210).
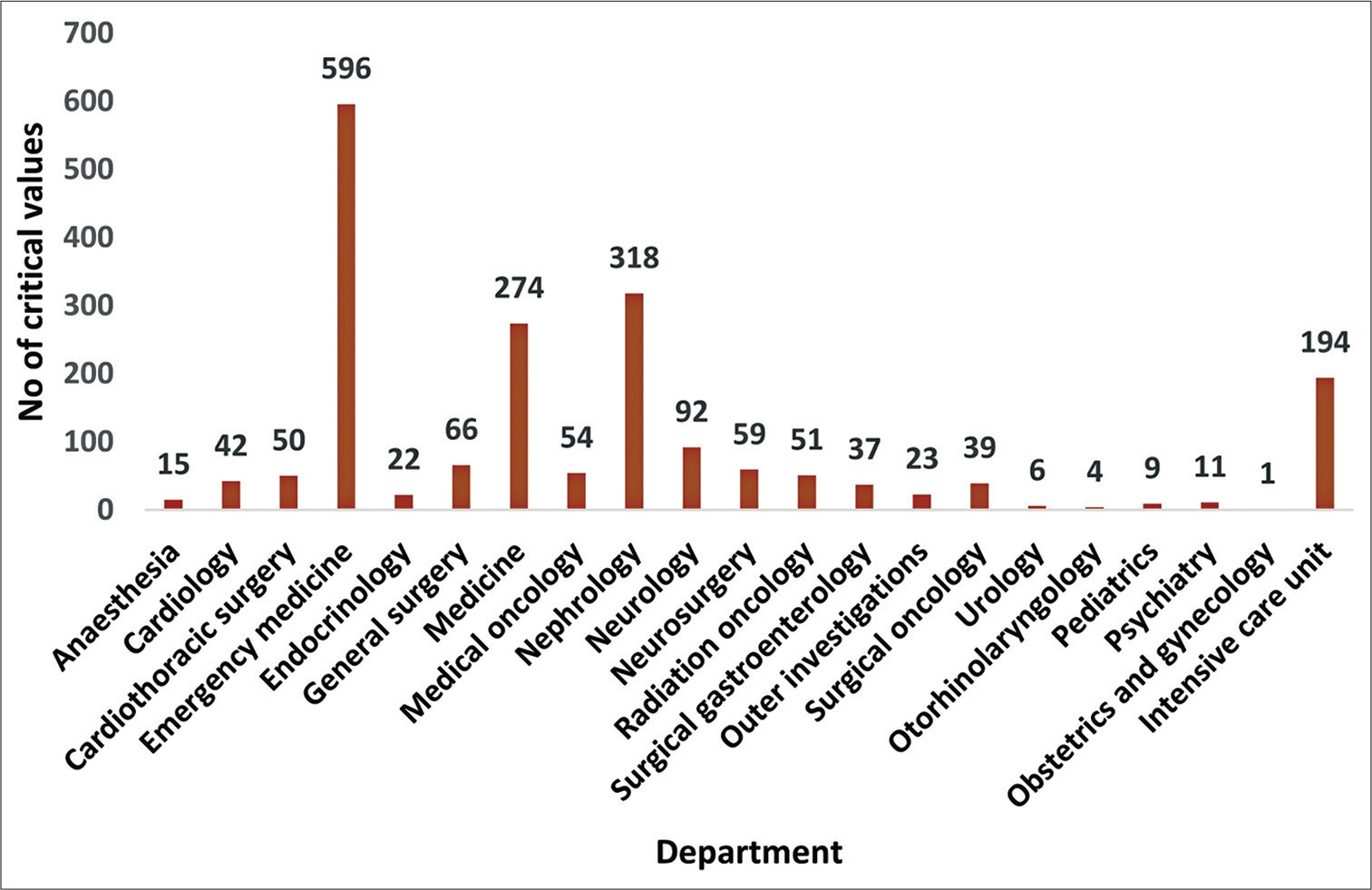
- Bar graph with the number of critical values reported by each clinical department during the 6-month study period. The x-axis represents different clinical departments. The y-axis represents the number of critical values reported.
| Critical alertintimation | N criticalalerts | % of all critical alerts(N = 1,963) |
|---|---|---|
| TAT<1 h | 1,703 | 86.8 |
| TAT>1 h | 50 | 2.5 |
| Unsuccessful | 210 | 10.7 |
TAT, turnaround time (time from the critical value reported in the laboratory to the time critical value intimated to the concerned doctor/nursing staff).
Out of 1,963 critical alerts reported in the biochemistry laboratory, 260 (13.3%) alerts were not intimated successfully or intimated at greater than 1 hour after the critical alert was reported in the laboratory. Table 5 presents the causes of unsuccessful or delayed intimation of critical alerts. Outpatient requests are the major cause among all the causes of unsuccessful reporting of critical alerts (~38.8%), whereas delay in the intimation of critical alert (>1 hour TAT) is mainly due to the transfer of the inpatient to a different ward as a part of treatment (~19.2%). Investigations requested from other hospitals contribute approximately 10.8% of all unsuccessful intimations of critical alerts.
| Causes of unsuccessful or delayed intimation of critical values | N critical values (%) |
|---|---|
| OP requests | 101 (38.8) |
| Patient not found in the ward mentioned in the request/patient transferreda | 50 (19.2) |
| Phone in the ward not working/not answered | 10 (3.8) |
| Not able to trace the inpatient location | 71 (27.3) |
| Investigations from other hospitals | 28 (10.8) |
N, number of critical values of unsuccessful intimation or delay in intimation (>1 h); OP, outpatient, TAT: Turnaround time.
aIntimation time of critical alert is greater than 1 hour. 7
The department with the highest number of unsuccessful or delayed intimation of critical alerts was the nephrology department (20%), followed by the emergency medicine (19.2%) and medicine departments (17.3%). The major cause of unsuccessful or delayed nephrology critical values was outpatient requests, which account for approximately 82.6% of all the causes. For emergency medicine, the major cause was traceability of patients (48%) and in the medicine department, the major cause was again outpatient requests (42.2%).
The clinical actions taken after critical result notification are represented in Table 6. Out of successfully reported critical alerts (1,703), 100 case sheets were randomly reviewed to assess the impact of telephonic notification in the documentation of critical alerts and the use of critical alert notification in clinical decision-making. Of the 100 intimated critical results, 91 cases led to corrective action by initiating or changing treatment to resolve life-threatening conditions, 1 patient expired by the time critical alert was intimated, 1 patient left against medical advice, and in 7 patients it did not lead to medical action after intimation of the critical result. According to medical records, all intimations were recorded in the case sheets, out of which 88/100 intimations were documented in the nurses’ charts and 68/100 were documented in the doctors’ charts. In all the 100 case sheets, these critical reports were documented either in the doctors’ or nurses’ charts or in both (20 of 100 case sheets). A repeat investigation was initiated in 98/100 cases after corrective action to reassess the treatment given (except for the patient who expired and the one who left against medical advice). The seven cases where no medical action was taken were chronic kidney disease patients. These patients were already on treatment and dialysis was continued. No further treatment change was done, but post dialysis, a repeat investigation was requested.
| Actions after notification | No. of records per 100 records |
|---|---|
| Documented in doctors’ charts | 68/100 |
| Documented in nurses’ charts | 88/100 |
| Notifications lead to treatmentinitiation or change of treatment | 91/100 |
| Repeat investigations requested after correction | 98/100 |
DISCUSSION
This study provides an overview of our critical value reporting system after analyzing data collected over a 6-month period. We comprehensively reviewed the various operational aspects of critical value reporting like the parameters studied, TAT, and clinical action taken. There are very few studies on critical value notification from our region, and this study provides us an opportunity to compare with published literature and introspect. The implementation of the critical values list varied among the laboratories depending on the sample load, knowledge of laboratory staff, type of hospital, and also the type of analyzer used.[10] The first prerequisite for an efficient critical value notification system is shortlisting the tests to be included and their cutoff limits.[11] There is a huge variation among these tests across laboratories as they are based on recommendations by professional bodies based on older surveys,[12] and it is essential to identify the most appropriate alert thresholds based on well-designed outcome studies done in collaboration with clinicians.[13] Laboratories can use published national standards on critical value ranges as a benchmark and adjust their list of critical values accordingly.[14,15] The critical value tests in our laboratory were established based on inputs from the clinicians and were in concordance with the national figures. This study analyzed the incidence of critical values, the most common analytes with critical values, TAT, and clinical action taken in our hospital, and compared them with published literature. The total incidence of critical values over a 6-month period was 0.50%, which was well within the range observed in the literature (0.08–0.96%[9,16-23]; Table 7). This wide difference in the incidence of critical values may be explained by the remarkable interlaboratory differences in the critical values notification list and the threshold values.[9,16-23] The rate of critical value also depends on the type of patients studied, with lower rates observed in studies involving outpatients[23] and high rates in studies involving patients in the emergency department or the ICU.[16] Our study included a heterogenous mix of patients from outpatients, emergency department or ICU, and inpatients. Moreover, being a tertiary care hospital, many patients are referred from smaller centers in critical condition, causing a moderate rate of reporting of critical values. The most commonly notified critical results in our laboratory were for potassium (55.9%), sodium (19.3%), and calcium (15.7%). The analytes with the maximum critical alerts described in the literature were for potassium.[9,16-23] Other analytes were glucose, sodium, calcium, and creatinine. The average TAT for critical value notification in our laboratory was 20 minutes. The TAT described in the literature ranged from 4 minutes[20] to 2.3 hours.[16] This variability in TAT is attributed to different types of notification systems used to inform the critical alerts. The various methods of notification systems mentioned in literature are paging,[16] telephone calls with readback,[9,17,19-23] personal digital assistance (PDA) with short messaging services (SMS),[17] laboratory information systems (LIS) with popup notifications,[9,19,21-23] and e-mail.[21] The purpose of alerting a critical value is not served if there is a delay in notification. Jha and Agarwal in a quality improvement study analyzed the various reasons for prolonged TAT (incomplete test requisition form, unawareness of noting personnel, dropped calls, nonavailability of clinicians, insufficient sample for redoes, inattentiveness of laboratories, irrelevant clinical data, etc.) using a fishbone model and reduced the TAT by 30% through appropriate corrective measures.[24] The critical alerts in our hospital were intimated to hospital nursing staff or residents using intercom phones with readback, which were then informed to the consultants. This process explains the TAT obtained in our study. The TAT was significantly lower with decreased error rates in laboratories using LIS when compared with laboratories using more traditional systems.[25] Automated communication/computerized notification systems improve TAT and avoid potential errors. However, even these are not fool proof and missed critical value call backs due to middleware flaws are reported in the literature.[26]
| Sl. no. | Study | Duration | Study population | CA (%) | Parameter | Department | TAT | Clinical action taken | Informing method |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Kuperma et al.[16] | 60 d | ICU IPD | 0.96 | Hypoxemia Low platelet count |
NA | 2.3h | NA | Paging |
| 2 | Dighe et al.[17] | 12 mo | IPD ICU/ED OPD | 0.25 | Potassium | NA | 22 min | NA | Telephone call |
| 3 | Park et al.[18] | 12 mo | ICU IPD | 0.08 | Potassium | NA | 65 min | 79% | PDA phone with SMS |
| 4 | Yang et al.[19] | 12 mo | IPD | 0.96 | Potassium | Hematology Nephrology |
NA | NA | LIS notification Telephone call |
| 5 | Agarwal et al.[20] | 25 mo | IPD OPD | 0.25 | Sodium Potassium |
NA | 60 min | NA | Telephone call with read back |
| 6 | Delgado Rodriguez et al.[9] | 12 mo | ER IPD OPD | 0.1 | Glucose Potassium |
Nephrology Endocrinology |
4-17 min | IPD: 100% OPD: 54% |
LIS notification Phone Mail |
| 7 | Arbiol-Roca et al.[21] | 6 mo | IPD OPD | 0.4 | Partial O2 pressure Potassium |
NA | NA | NA | LIS notification SMS Phone |
| 8 | Li et al.[22] | 4 y | ED IPD OPD | 0.49 | Troponin BUN Potassium Creatinine |
NA | 41 min | NA | LIS notification |
| 9 | Laguna et al.[23] | 12 mo | OPD | NA | Potassium Glucose Calcium Magnesium |
Nephrology Hematology Oncology |
35 min | 49% | Telephone call |
| 10 | SVIMS 2022 | 6mo | IPD OPD | 0.5 | Potassium Sodium Calcium |
Emergency medicine Nephrology |
20 min | 91% | Telephone call |
Abbreviations: BUN, blood urea nitrogen; ED, emergency department; ER, emergency room; IPD, inpatient department; LIS, laboratory information system; OPD, outpatient department; PDA, personal digital assistant; SMS, short message service.
Failure to intimate a critical value might have a negative impact on patients’ clinical outcomes and could lead to possible legal issues for the health care system.[27], Irrespective of the notification method used, the percentage of un-notified critical alerts in the literature ranged from 0.1 to 10.2%.[28] Unsuccessful intimation of critical alerts were seen in 210 patients (10.7%) in our study. The major causes for unsuccessful intimation of critical alerts in our study were OPD investigations, inability to trace the patients, and direct investigations done by the patients at the laboratory.
Corrective clinical action (treatment initiation or change of treatment) after critical value notification reported in literature ranged from 49 to 100%.[9,23] The clinical actions taken after critical result notification were analyzed within 1 week and a corrective action was taken in 91% of the patients in our study. Documentation of critical alerts was found in all the case sheets. Most of the time, these critical results were documented in the nurses’ chart as ward nurses were available round the clock and treatment was initiated immediately by consulting the doctor on duty. Lack of corrective action was seen in 9% of the patients, which was attributed to outpatient requests and patients with chronic kidney disease who were already on dialysis. The rate of corrective clinical action depends on various factors like the place of sample collection (IPD/OPD), the parameters analyzed, and the population studied. The probability for corrective clinical action was higher in inpatients than in outpatients.[9] The impact of corrective action varied across the analytes studied. The highest clinical impact of corrective action was seen in patients with hypokalemia, hyponatremia, and hypomagnesemia. A lower clinical impact was seen in patients with hypoglycemia, hyperkalemia, and calcium (hypocalcemia, hypercalcemia).[23] The literature suggests having different threshold values for hypoglycemia in diabetic and nondiabetic patients to increase clinical impact.[23,29] Patients with hyperkalemia had other confounding factors like chronic kidney failure, high blood pressure, heart failure, and use of drugs that interfere with potassium metabolism, leading to decreased clinical impact.[30]
Quality in laboratory testing includes all aspects of the socalled “brain-to-brain loop,” from the “preanalytical” phase through the “analytical” phase to the “postanalytical” phase.[31] Errors in the analytical phase have shown a drastic drop over the last few decades following significant improvements in the analytic techniques, reagents, instrumentation, and advancements in information technology, along with quality control and assurance methods.[32] However, the preanalytical phase (ordering, collection, identification, transportation, and separation) and the postanalytical phase (receiving, interpreting, and using these results for patient management) are more error prone.[33] Critical value notification is an essential component in the postanalytical phase of the loop.
In the wake of our study, to improve compliance with the critical alert notification protocol, the following actions are recommended. Begin by reviewing and updating the list of critical values, and then collaborating with the clinicians and referencing professional bodies to establish appropriate cutoff limits based on the patient population. Ensure accessibility through version control. Next, focus on reducing the TAT by identifying and addressing factors causing delays, streamlining processes, improving communication channels, and regularly evaluating the TAT performance while implementing quality improvement initiatives. Introduce an automated notification system by integrating an LIS with notification systems for efficient and timely delivery. Enhance staff training and awareness by providing comprehensive training on the protocol, emphasizing procedures, responsibilities, workflows, and the impact on patient outcomes and legal implications. Foster interdisciplinary discussions and joint training sessions. Finally, maintain a record of incidents, outcomes, and protocol improvements; share experiences with the stakeholders; contribute to scientific literature; and collaborate with other institutions. Continually reassess and adjust the protocol to ensure ongoing improvement. Remember to adapt these recommendations to your laboratory’s specific context and resources.
To standardize the notification of critical values in laboratories, take the following steps:
Assess current methods: Evaluate the effectiveness of existing notification methods considering factors such as reliability, speed, and potential for errors.
Select optimal method: Choose the most suitable method like phone calls, intercom, or digital platforms.
Develop guidelines: Establish protocols specifying who initiates and receives notifications, response times, and backup plans for nonresponses.
Train staff: Teach laboratory personnel the standard notification method, ensuring they understand all procedures.
Standardize documentation: Implement a uniform process for documenting notifications, recording time, and parties involved.
Encourage communication: Promote feedback between the laboratory staff and the health care professionals to address any issues.
Through these steps, you can enhance consistency, efficiency, and effectiveness in critical alert notifications, promoting prompt clinical responses and better patient care.
Based on the findings of our study, we proposed and implemented a series of changes in the critical alert notification protocol at our tertiary care center. The first step involved raising awareness of these changes among all clinical laboratory in charges, duty residents, and technicians. In an effort to streamline communication, technicians in the clinical laboratory are now required to alert the resident posted in the laboratory of any delays in reporting critical alerts. Similarly, residents in the laboratory are expected to inform the clinical laboratory in charge in case of such delays. If required, the laboratory resident may trace the patient through the Medical Records Department (MRD). A crucial part of this process is the role of the clinical laboratory in charge, who is tasked with supervising and monitoring the process until the information has been conveyed. In the cases where the patient cannot be traced despite these efforts, the issue is escalated to the Head of the Department (HOD). To further enhance communication, the Hospital Medical Superintendent has issued a circular mandating that a list of on-duty residents from all departments be provided daily to the laboratories. The MRD team has also been instructed to assist in tracing patients when requested by the laboratories. If all other measures fail, the HOD of the laboratories is authorized to inform the HOD of the department from which the investigation was originally requested.
We are also planning to introduce a new Hospital Information Management System (HIMS). This system is designed to instantly notify the requesting department’s HIMS with a popup message when a critical result is reported. Additionally, these critical results will be disseminated via SMS to the consultant and residents of the department that made the initial request. This forms a part of our strategy to improve the TAT for critical result notification in instances of delay, as illustrated in Figure 2.
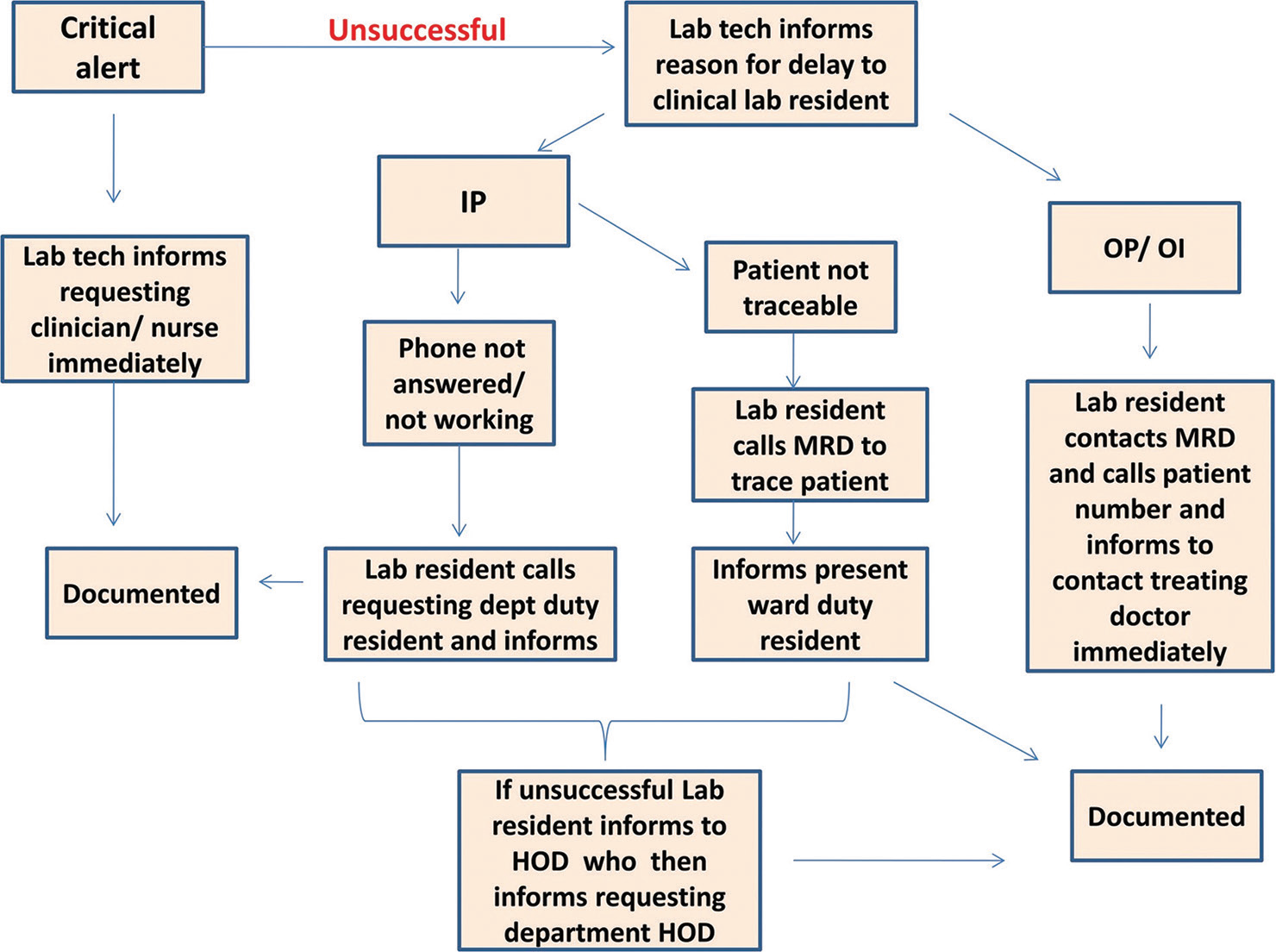
- Flowchart for optimizing the turnaround time (TAT) in delayed critical result notifications. HOD, head of department; IP, inpatients; MRD, medical record department; OI, other hospital investigations; OP, outpatients.
With the implementation of these changes, we expect to see improvements in our operations, which we will be monitoring as part of an ongoing, systematic study. This will allow us not only to validate our methods but also to continuously refine our processes based on what we learn. Our primary goal remains optimizing the TAT for critical result notifications using this long-term study for consistent improvements and evidence-based adjustments.
CONCLUSIONS
Critical value reporting is indispensable to patient care and safety. Our study evaluated the current protocol of telephonic notification of critical results at our tertiary care teaching hospital and revised the protocol for successful notification in the defined time frame. Recommendations include revising the critical value notification list based on sample collection setting (IP/OP) and implementing an LIS with automated communication systems to reduce TAT. Overall, our findings highlight the need for regular self-evaluation, continuous improvement, and compliance with the critical result notification protocol so that clinical needs are met without raising the risk of information overload.
Author Contribution
S.T. conceived and designed the study, conducted experiments, performed data collection, analyzed data, provided technical support, and wrote the manuscript.
A.R.B. conceived and supervised the project, critically reviewed the manuscript, and provided guidance throughout the study. All the authors read and approved the final version of the manuscript.
Approvals
The research protocol was reviewed and technical approval was given by Medical Research Committee of Sri Venkateswara Institute of Medical Sciences.
The institutional ethics committee of Sri Venkateswara Institute of Medical Sciences reviewed the protocol and approved the project vide IEC No1232.
Conflict of Interest
None declared.
Funding
None.
References
- Critical (panic) value notification: an established laboratory practice policy (parameter) JAMA. 1990;263:709.
- [CrossRef] [PubMed] [Google Scholar]
- Management of Critical and Significant-Risk Results CLSI GP47 Document (1st ed). Wayne, PA: CLSI; 2015. p. :17.
- [Google Scholar]
- Towards harmonisation of critical laboratory result management: review of the literature and survey of Australasian practices. Clin Biochem Rev. 2012;33:149-160.
- [Google Scholar]
- International Organization for Standardization (ISO) ISO 15189:2012. In: Medical Laboratories: Requirements for Quality and Competence. Geneva: International Organization for Standardization; 2012.
- [Google Scholar]
- National Accreditation Board for Testing and Calibration Laboratories. In: Document 112: Specific Criteria for Accreditation of Medical Laboratories. Gurugram, India: NABL; 2022. Accessed June 16 2023 at: https://nabl-india.org/nabl/file_download.php?filename-201905031045NABL-112-effective-from-01.06.2019-doc.pdf
- [Google Scholar]
- Critical laboratory values communication: summary recommendations from available guidelines. Ann Transl Med. 2016;4:400.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing the turnover time of critical value in hospitals. Clin Investig (Lond). 2019;9:17-19.
- [Google Scholar]
- Assessment of a laboratory critical risk result notification protocol in a tertiary care hospital and their use in clinical decision making. Biochem Med (Zagreb). 2019;29:30703.
- [CrossRef] [PubMed] [Google Scholar]
- Critical value of the clinical laboratory test in Thailand. J Med Assoc Thai. 2010;93:S22-S27.
- [Google Scholar]
- What alert thresholds should be used to identify critical risk results: a systematic review of the evidence. Clin Chem. 2016;62:1445-1457.
- [CrossRef] [PubMed] [Google Scholar]
- A survey of laboratory 'critical (alert) limits' in the UK. Ann Clin Biochem. 2003;40:181-184.
- [CrossRef] [PubMed] [Google Scholar]
- Harmonization of critical result management in laboratory medicine. Clin Chim Acta. 2014;432:135-147.
- [CrossRef] [PubMed] [Google Scholar]
- Global trends in critical values practices and their harmonization. Clin Chem Lab Med. 2011;49:167-176.
- [CrossRef] [PubMed] [Google Scholar]
- Laboratory critical values policies and procedures: a college of American Pathologists QProbes Study in 623 institutions. Arch Pathol Lab Med. 2002;126:663-669.
- [CrossRef] [PubMed] [Google Scholar]
- How promptly are inpatients treated for critical laboratory results? J Am Med Inform Assoc. 1998;5:112-119.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of laboratory critical value reporting at a large academic medical center. Am J Clin Pathol. 2006;125:758-764.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluating the short message service alerting system for critical value notification via PDA telephones. Ann Clin Lab Sci. 2008;38:149-156.
- [Google Scholar]
- Analysis of laboratory repeat critical values at a large tertiary teaching hospital in China. PLoS One. 2013;8:e59518.
- [CrossRef] [PubMed] [Google Scholar]
- Study of variables affecting critical value notification in a laboratory catering to tertiary care hospital. Indian J Clin Biochem. 2015;30:89-93.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of laboratory critical values at a referral Spanish tertiary university hospital. Biochem Med (Zagreb). 2019;29:10704.
- [CrossRef] [PubMed] [Google Scholar]
- Enhance the effectiveness of clinical laboratory critical values initiative notification by implementing a closed-loop system: a five-year retrospective observational study. J Clin Lab Anal. 2020;34:e23038.
- [CrossRef] [PubMed] [Google Scholar]
- Notification of biochemistry critical results and its clinical impact on outpatient care: experience in a Spanish tertiary hospital. Clin Chem Lab Med. 2021;59:1777-1783.
- [CrossRef] [PubMed] [Google Scholar]
- Quality tools and strategy for critical alerts process improvements to ensure patient safety. J Lab Physicians. 2022;14:471-478.
- [CrossRef] [PubMed] [Google Scholar]
- Improving patient safety by repeating (read-back) telephone reports of critical information. Am J Clin Pathol. 2004;121:801-803.
- [CrossRef] [PubMed] [Google Scholar]
- Missed critical value callbacks due to middleware flaw. Clin Biochem. 2021;96:71-74.
- [CrossRef] [PubMed] [Google Scholar]
- Failure to follow-up test results for ambulatory patients: a systematic review. J Gen Intern Med. 2012;27:1334-1348.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of effectiveness of a computerized notification system for reporting critical values. Am J Clin Pathol. 2009;131:432-441.
- [CrossRef] [PubMed] [Google Scholar]
- Critical limits of laboratory results for urgent clinician notification. EJIFCC. 2003;14:11-18.
- [Google Scholar]
- Laboratory critical values: automated notification supports effective clinical decision making. Clin Biochem. 2014;47:1163-1168.
- [CrossRef] [PubMed] [Google Scholar]
- The brain-to-brain loop concept for laboratory testing 40 years after its introduction. Am J Clin Pathol. 2011;136:829-833.
- [CrossRef] [PubMed] [Google Scholar]
- The detection and prevention of errors in laboratory medicine. Ann Clin Biochem. 2010;47:101-110.
- [CrossRef] [PubMed] [Google Scholar]
- Exploring the iceberg of errors in laboratory medicine. Clin Chim Acta. 2009;404:16-23.
- [CrossRef] [PubMed] [Google Scholar]



