
Translate this page into:
Fine Needle Aspiration Cytology of Eccrine Spiradenoma of Back: Report of a Rare Case
Address for correspondence: Dr. Jyoti Prakash Phukan, E-mail: drjyotiphukan@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Eccrine spiradenoma is an uncommon benign adnexal tumor. Cytological features of eccrine spiradenoma have been described very rarely in English literature. In the present case, we are describing a case of eccrine spiradenoma of back, which was diagnosed by fine-needle aspiration cytology and subsequently confirmed by histopathology. Its cytology revealed tight multilayered clusters of uniform benign cuboidal epithelial cells along with spindle-shaped myoepithelial cells and occasional lymphocytes.
Keywords
Adnexal tumor
eccrine spiradenoma
fine-needle aspiration cytology

INTRODUCTION
Eccrine spiradenoma is an uncommon benign adnexal tumor, arises from intra-dermal part of the duct of eccrine sweat gland.[12] It commonly presents as a painful, nodular, slow-growing mass at trunk, proximal extremities and head and neck region in adult age.[3] Though histopathology of eccrine spiradenoma is well-established, cytological features are very rarely reported in English literatures.[12] Here, we are reporting a case of cytological diagnosis of eccrine spiradenoma of back in a 32-year-old male, which was later on confirmed by histopathological examination.
CASE REPORT
A 32-year-old male visited to surgery outpatient department of our institute with complaints of slow-growing painful nodular swelling at back for last 6 months [Figure 1]. He had no history of trauma to the local site. On clinical examination, it was a tender, nodular swelling of 2 cm × 1 cm dimension. It has restricted mobility and overlying skin showed bluish hue at apical region. Clinically, it was diagnosed as epidermal cyst and fine-needle aspiration cytology was advised. Fine-needle aspiration was done with 22-gauge needle attached with 10 cc disposable plastic syringe. Aspirate was blood mixed. Air-dried smears are stained with Leishman–Giemsa stain and alcohol fixed smears stained with Papanicolaou (PAP) stain. Cytology showed cohesive multilayered clusters of uniform round to oval epithelial cells admixed with few spindle-shaped cells and mature lymphocytes in the background of red blood cells [Figure 2a and b]. The epithelial cells had scanty cytoplasm, round nuclei and inconspicuous nucleoli. The myoepithelial cells were spindle to oval with darker hyperchromatic nuclei and very scanty cytoplasm. On pap stained smear, the epithelial cells, and myoepithelial cells are easily differentiated as epithelial cells are large and pale staining, while myoepithelial cells are small and darkly stained [Figure 3a]. Occasional rosette-like structures were also identified [Figure 3b]. Cyto-morphology was diagnosed as benign adnexal tumor, possibly eccrine spiradenoma.

- Clinical photograph showing small nodular swelling with bluish hue over back
![Fine-needle aspiration cytology showing (a) cohesive multilayered clusters of round to oval epithelial cells with few myoepithelial cells (Leishman–Giemsa[LG], ×100); (b) high power view showing round to oval pale epithelial cells (black arrow), spindle to oval myoepithelial cells having darker nuclei and scanty cytoplasm (white arrow) and occasional lymphocytes red arrow)(LG, ×400)](/content/164/2014/6/2/img/JLP-6-130-g002.png)
- Fine-needle aspiration cytology showing (a) cohesive multilayered clusters of round to oval epithelial cells with few myoepithelial cells (Leishman–Giemsa[LG], ×100); (b) high power view showing round to oval pale epithelial cells (black arrow), spindle to oval myoepithelial cells having darker nuclei and scanty cytoplasm (white arrow) and occasional lymphocytes red arrow)(LG, ×400)
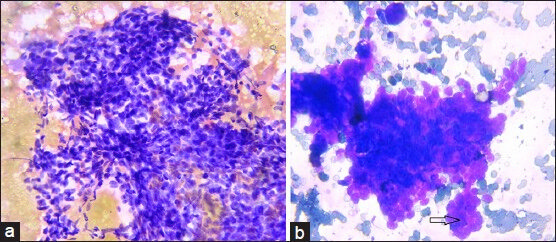
- Fine-needle aspiration cytology showing (a) admixture of pale large epithelial cells and darker spindle to oval myoepithelial cells and occasional lymphocytes (Papanicolaou, ×100); (b) tumor cells arranged around perivascular space forming a rosette-like structure (arrow)(Leishman– Giemsa, ×400)
Excision of the tumor done under local anaesthesia and specimen was sent to Pathology Department for histopathological examination. On gross examination, the tumor was well-circumscribed, firm and attached with a skin tag, measuring 2 cm × 1 cm × 1 cm. In cut section, it was solid, gray-white. Histopathology of the tumor revealed sharply demarcated lobular mass in dermis, comprised tightly packed small basaloid cells arranged parallely in cords, sheets, nests and branched trabeculae alongwith numerous hyalinised stroma and blood vessels [Figure 4a]. On high power view, two distinct types of cells were identified;–peripherally placed small darker cells with hyperchromatic nuclei and central area containing larger pale cells with a moderate cytoplasm and vesicular nuclei [Figure 4b]. Arrangement of neoplastic cells surrounding eosinophilic hyaline material gave rise to pseudo-rosettes. Scattered lymphocytes were seen within the tumor tissues. Histomorphology confirmed the cytological diagnosis as eccrine spiradenoma. In the postoperative period, wound was healthy. The patient was followed-up for 1 year and no recurrence was noted during this period.
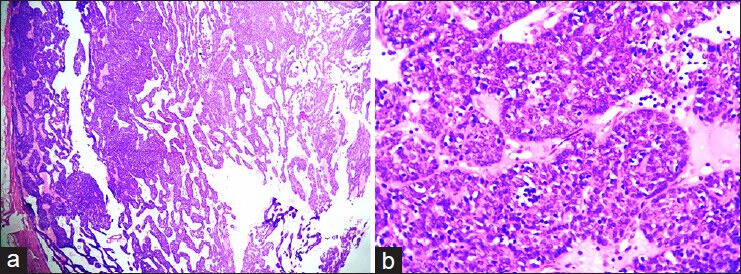
- Section showing (a) typical feature of eccrine spiradenoma with a sharply demarcated lobular tumor mass in the dermis composed of tightly packed basaloid cells arranged parellely in cords, sheets, nests and branched trabeculae with hyalinised stroma(H and E, ×40); (b) tumor cells in high power (H and E, ×400)
DISCUSSION
Eccrine spiradenomas are rare benign adnexal tumors, which arise from intraductal part of the duct of eccrine sweat gland.[34] It was first extensively studied and described by Kersting and Helwing in 1956.[5] Spiradenomas commonly occur at head and neck region, upper part of trunk and extremities, but other uncommon sites are also reported.[13] Eccrine spiradenomas have equal gender distribution and these commonly present as small, slow-growing, painful, nodular subcutaneous masses.[34] Similarly in the present case, it was a small, nodular, subcutaneous, tender mass at back. Most of the cases of eccrine spiradenoma are 1-2 cm in size but cases of large size (giant) also have been documented.[3] Malignant transformation of eccrine spiradenomas are extremely rare but documented.[34]
Though histopathology of eccrine spiradenomas is well established, cytological diagnostic criteria are still lacking. Very few cases of cytological diagnosis have been reported till date.[12] Cytology of eccrine spiradenoma comprises of tight clusters of multilayered uniform cuboidal bland epithelial cells arranged surrounding hyalinized material. Tubules and pseudo-rosette formation by epithelial cells alongwith spindle-shaped myoepithelial cells, many scattered bared nuclei and small lymphocytes are the key components of cytology of eccrine spiradenomas.[67] In the present case, cytology revealed tight clusters of multilayered uniform cuboidal cells alongwith spindle cells, scanty lymphocytes and occasional pseudo-rosettes.
Cytologically eccrine spiradenomas should be differentiated from adenoid cystic carcinoma, glomus tumor and other eccrine adnexal tumors (hidradenoma, cylindroma, chondroid syringoma) and spiradenocarcinoma. Kolda et al. described a case of eccrine spiradenoma mimicking adenoid cystic carcinoma in cytology.[2] Cytology of adenoid cystic carcinoma contains a single type of cells and hyaline globules in contrast to epithelial-myoepithelial–lymphocytic cells in eccrine spiradenomas.[2] Vidyavathi et al. have reported a case of glomus tumor of forearm, cytologically misinterpreted as eccrine spiradenoma.[8] Uniformity of epithelial looking cells, presence of basement membrane like material and overlooking endothelial cells in a painful lesion were the causes of misdiagnosis.[8] Care should be taken on the presence of endothelial cells, lack of three types of cells in cytology smears, lack of tight multilayered clusters in glomus tumor to distinguish from eccrine spiradenoma. Cytology of hidradenoma composed of cohesive clusters of polygonal cells with moderate clear to pale eosinophilic cytoplasm. Nuclei are oval with smooth nuclear membrane and distinct nucleoli.[6] On cytological evaluation of cylindroma, smears show pallisaded arrangement of small basaloid cells alongwith few light staining cells and hyaline globules.[6] Cytologically chondroid syringoma is synonymous to the pleomorphic salivary adenoma, which comprises of two types of cells (epithelial and myoepithelial) with a chondro-myxoid ground substances.[9] All the three benign adenexal tumors lack lymphocytes in the cytological smears.
Distinction from its malignant counterpart is possible, which shows of cellular atypia, open chromatin in nucleus, conspicuous nucleoli.[10] Other features of malignancy such as mitosis and cellular pleomorphism are also absent in eccrine spiradenomas.[11]
Histologically eccrine spiradenoma composed of lobules of packed neoplastic cells. In higher magnification, two distinct populations of cells are exhibited–peripherally placed darker basaloid cells with hyperchromatic nuclei and larger pale cells with ample of cytoplasm and vesicular nucleoli. Stroma intervening the lobules may exhibit edematous or hydropic degeneration with lymphocytic infiltration.[34] The diagnosis of eccrine tumors sometimes cannot be made definitely on cytology or even on histology also.[6] In these cases, immunohistochemistry can play an important role.[12] Immunohistochemically eccrine spiradenomas show cytokeratin (CK) positivity (epithelial marker), carcino embryonic antigen reactivity (tubules) and lymphocytes exhibit T-cell phenotype.[1] Syringoma shows positivity for CK6 and CK10, while spiradenoma shows positivity for CK7.[6]
Treatment of eccrine spiradenoma is surgical excision. Local recurrence is uncommon and malignant transformation is rare.[13] In conclusion, eccrine, spiradenoma is a rare benign adnexal tumor and very rarely evaluated by cytology. Though histopathology is a gold standard, cytology can diagnose a case of eccrine spiradenoma and can guide the surgeon regarding management. We hope that the present case report will help in further evaluation of cytodiagnosis of such a rare appendageal tumor.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Chondroid Syringoma and Eccrine Spiradenoma. Online J Health Allied Sci. 2011;10:10.
- [Google Scholar]
- Eccrine spiradenoma mimicking adenoid cystic carcinoma on fine needle aspiration. A case report. Acta Cytol. 1997;41:852-8.
- [Google Scholar]
- Eccrine spiradenoma arising in the breast misdiagnosed as an epidermal inclusion cyst. Korean J Radiol. 2011;12:256-60.
- [Google Scholar]
- Fine needle aspiration cytology of eccrine skin adnexal tumours. J Cytol Histol. 2011;2:129.
- [Google Scholar]
- Fine needle aspiration cytology of eccrine spiradenoma; Report of a case. Korean J Cytopathol. 2005;16:98-101.
- [Google Scholar]
- Glomus tumor mimicking eccrine spiradenoma on fine needle aspiration. J Cytol. 2009;26:46-8.
- [Google Scholar]
- Chondroid syringoma: A diagnosis by fine needle aspiration cytology. J Cutan Aesthet Surg. 2012;5:222-5.
- [Google Scholar]
- Malignant eccrine spiradenoma (spiradenocarcinoma): A clinicopathologic study of 12 cases. Am J Dermatopathol. 2000;22:97-103.
- [Google Scholar]
- Immunohistochemical differentiation of four benign eccrine tumors. J Cutan Pathol. 2009;36:190-6.
- [Google Scholar]



