
Translate this page into:
Granulicatella adiacens abscess: Two rare cases and review
Address for correspondence: Dr. Sangita Gupta, Department of Microbiology, Room No. 108, OPD Block, First Floor, ESI Hospital, Basaidarapur, New Delhi - 110 015, India. E-mail: sangitagupta1@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Granulicatella adiacens is a nutritionally variant streptococcus species. These bacteria are rarely isolated in the laboratory due to their fastidious growth requirements. These have been mostly reported from bloodstream infections, infective endocarditis, infections of orbit, nasolacrimal duct and breast implants. Here, we are reporting two cases of subcutaneous abscesses caused by G. adiacens. In first case, it was isolated from abscess around elbow joint and second case was a suprapatellar abscess. We have also reviewed the published data concerning diagnosis and antimicrobial susceptibility pattern of Granulicatella infections and included some Indian cases.
Keywords
Granulicatella adiacens
nutritionally variant streptococcus
suprapatellar abscess

Introduction
Granulicatella adiacens is a nutritionally variant streptococcus (NVS) which requires pyridoxal or other additional agents to be incorporated into standard media for its successful laboratory isolation.[1] These bacteria were transferred from Streptococcus to a separate genus, Abiotrophia[2] and later on, this genus was divided into the genera Abiotrophia and Granulicatella (species Granulicatella adiacens, Granulicatella elegans, and Granulicatella balaenopterae) on the basis of 16S rRNA gene sequencing.[3]
Despite being a part of the oral, gastrointestinal, and urogenital commensal flora, G. adiacens is rarely implicated in infections due to their difficult isolation and differentiation techniques as compared to other streptococci. These have been mostly reported to cause bacteremia and endocarditis and less commonly seen in device associated infections such as postinstrumentation meningitis, infections of breast implants, and of peritoneal dialysis-related peritonitis.[1] There are very few reports of localized pyogenic infections, and most of them are in patients with underlying pathology like diabetes or other systemic illnesses. Here, we are reporting two cases of subcutaneous abscesses caused by G. adiacens. To the best of our knowledge, this is the first case report from India describing subcutaneous abscesses due to G. adiacens in healthy adult persons.
Case Reports
Case 1
A 30-year-old previously healthy male presented to the hospital casualty with complaints of pain and swelling in the right knee for 7 days. There was no history of fever, trauma, or any surgical procedure. Local examination revealed an erythematous, diffuse, warm, and tender swelling over the right knee joint. It was associated with restricted and painful movements of knee.
Investigations
Laboratory investigations revealed leukocytosis with neutrophilia (TLC-11,300 with 77% neutrophils). All other hematological, liver and kidney function tests were within normal limits. Blood sugar and GTT was normal.
Management
A diagnostic tap from the swelling yielded frank pus. Provisional diagnosis of septic arthritis of right knee was made. Next day, the patient was taken for arthrotomy of knee joint. During surgery, it was found to be a localized abscess situated above quadriceps femoris muscle in suprapatellar region. The abscess was drained and 2nd sample of pus was sent for culture and susceptibility. The final diagnosis of suprapatellar abscess was made. The patient was treated with intravenous cefotaxime 1 g 12 hourly. Wound was healthy by 5th day. The patient was discharged on cefuroxime 500 mg for 7 days. On follow-up after 2 weeks, the patient was in healthy condition.
Microbiological examination of pus
Both the samples gave similar results. On gross examination, both pus samples were thick and yellow in color. Gram stained smears showed many polymorphonuclear cells with a few Gram-positive (GP) pleomorphic cocci arranged in pairs and small chains. Samples were inoculated on sheep blood agar (SBA), MacConkey agar, and chocolate agar (CA) and incubated at 37°C. For enrichment, samples were also inoculated in BacTalert® FA (aerobic) and FN (anaerobic) (BioMerieux, France) culture bottles. None of the culture plates showed any growth up to 7 days of incubation, but BacTalert culture bottles beeped positive after 28 h in first and 32 h in the second sample. Gram staining from bottles showed Gram-positive pleomorphic cocci in pairs and small chains. Subculture from the positive bottles on SBA and CA showed growth of pinpoint, transparent, α-hemolytic colonies after 24 h of incubation. These were catalase and oxidase negative, optochin resistant, and bile sensitive. Gram staining of colonies showed GP cocci and coccobacilli in chains. Isolate was identified as G. adiacens by automated bacterial identification (ID) system Vitek 2 compact® (BioMerieux, France) using GP ID card with 99% confidence. Minimum inhibitory concentrations (MICs) were determined using antimicrobial susceptibility (AST) ST01 card of Vitek and interpreted as per Clinical and Laboratory Standards Institute (CLSI) breakpoints.[4] The isolate was found to be susceptible to penicillin, cefotaxime, ceftriaxone, erythromycin, clindamycin, levofloxacin, and vancomycin.
Case 2
An 18-year-old healthy male presented to the hospital OPD with right elbow abscess. A single pus soaked swab was received and plated on SBA, CA and MacConkey agar. Faint, tiny, translucent colonies grew on SBA and CA after 48 h incubation in candle jar. Vitek GP card identified isolate as G. adiacens and on MIC testing by E Test strip, isolate was found to be susceptible to penicillin, cefotaxime, ceftriaxone, clindamycin, levofloxacin and vancomycin, and resistant to erythromycin. This patient could not be followed up as he never returned to collect his report.
Discussion
Nutritionally variant streptococci (NVS) are named so as they grow best on media supplemented with thiol or pyridoxal.[1] With the increased use of commercial media like BacT Alert® culture bottles that contain pyridoxal and L-cystein, their isolation rate has increased. In most of the cases we reviewed, NVS were isolated from automated culture bottles.[56789] However, on subculture from these positive bottles growth is generally either delayed or/and very faint. Colonies can be identified by satellitism around colonies of Staphylococcus aureus, typical Gram stain picture of pleomorphism and increased growth on thiol containing media. Phenotypic ID is technically demanding and unreliable but automated ID systems like Vitek® or API Strep® panels have been successfully used as an easy alternative with good sensitivity and specificity. 16S rRNA gene sequencing is confirmatory but is feasible only in reference labs.
Clinically, Nutritionally variant streptococci (NVS) has been associated with up to 2.3% of cases of streptococcal bacteremia and up to 5% cases of streptococcal endocarditis.[10] Localized pyogenic infections are rare. There are a few isolated reports of septic arthritis, vertebral osteomyelitis and discitis. Out of 101 NVS isolates studied by Christensen and Facklam, the clinical diagnosis was endocarditis in 58% of patients, septicemia or bacteremia in 26% of patients and only single patient had scrotal abscess.[1]
In 2007, CLSI published guidelines (M45) for AST testing for NVS along with other fastidious microorganisms.[4] It recommended broth microdilution method (BMD) using cation-adjusted Mueller–Hinton broth supplemented with 2.5%–5% lysed horse blood and 0.001% pyridoxal HCl. The lack of disc diffusion breakpoints, FDA approved automated susceptibility systems, and limited availability of BMD in clinical laboratories makes it difficult to accurately report susceptibility pattern of these bacteria. E test on different media has been compared with BMD and has shown variable results in different studies.[1112]
There are only a few studies on AST pattern of NVS and most of these have used breakpoints for Streptococcus viridans to interpret their data.[10] In the largest study on susceptibility pattern of NVS, Alberti et al. tested 132 isolates (37 A. defectiva, 90 G. Adiacens, and 5 G. elegans) by BMD using CLSI M45 guidelines.[13] Only 38.9% of G. adiacens isolates were found susceptible to Penicillin, however, a large number (47.8%) of isolates were intermediate susceptible. Susceptibility to other antibiotics was cefotaxime (18.9%), ceftriaxone (43.3%), erythromycin (52.2%), clindamycin (84.5%), and levofloxacin (91.9%) but all G. adiacens isolates were 100% susceptible to meropenem and vancomycin. Both of our isolates were also susceptible to penicillin, cefotaxime, ceftriaxone, clindamycin, levofloxacin, and vancomycin except erythromycin resistance shown by one.
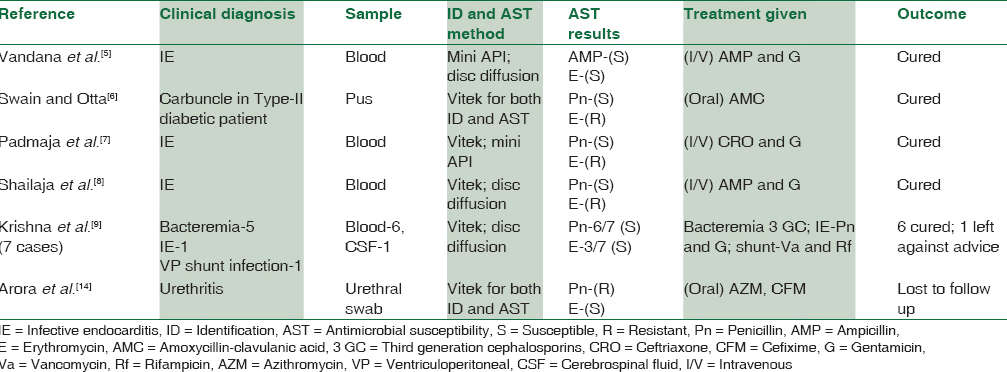
We could not find any well documented Indian research study on AST pattern of NVS except for a few case reports and a case series comprising of seven cases. In most of these reports, NVS was grown in BacT alert® bottle, identified by Vitek® and AST was performed either by disc diffusion method or Vitek® and interpreted using CLSI breakpoints for viridans streptococci [Table 1]. We also could not perform BMD due to nonavailability of required media supplements. Erythromycin resistance was reported in 7 out of 12 isolates reviewed by us, but penicillin resistance was less with only 2 isolates being resistant. Both of our isolates were also penicillin susceptible, but one was erythromycin resistant.[14]
On the basis of susceptibility data and clinical outcome of various cases, it is recommended to treat NVS related endocarditis like enterococci with penicillin and aminoglycoside.[6] However, pyogenic infections have been treated successfully with various antibiotics such as penicillin, cefotaxime, and erythromycin. Linezolid or vancomycin resistance has never been reported so far.
Conclusion
NVS is an important but under-reported cause of bacteremia and endocarditis and a rare cause of pyogenic infections. The use of automated culture and ID systems can definitely help in better isolation of these fastidious bacteria. More studies are required using standard methods of ID and AST to assess their susceptibility pattern, especially from India.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Granulicatella and Abiotrophia species from human clinical specimens. J Clin Microbiol. 2001;39:3520-3.
- [Google Scholar]
- Transfer of Streptococcus adjacens and Streptococcus defectivus to Abiotrophia gen. nov. as Abiotrophia adiacens comb. nov. and Abiotrophia defectiva comb. nov. respectively. Int J Syst Bacteriol. 1995;45:798-803.
- [Google Scholar]
- The genus Abiotrophia (Kawamura et al.) is not monophyletic: Proposal of Granulicatella gen. nov. Granulicatella adiacens comb. nov. Granulicatella elegans comb. nov. and Granulicatella balaenopterae comb. nov. Int J Syst Evol Microbiol. 2000;50 Pt 1:365-9.
- [Google Scholar]
- Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria. In: CLSI Guideline M45 (3rd). Wayne, PA: Clinical and Laboratory Standards Institute; 2015.
- [Google Scholar]
- Native valve endocarditis and femoral embolism due to Granulicatella adiacens: A rare case report. Braz J Infect Dis. 2010;14:634-6.
- [Google Scholar]
- Granulicatella adiacens – An unusual causative agent for carbuncle. Indian J Pathol Microbiol. 2012;55:609-10.
- [Google Scholar]
- Infective endocarditis due to Granulicatella adiacens: A case report and review. J Infect Dev Ctries. 2014;8:548-50.
- [Google Scholar]
- Infective endocarditis caused by Granulicatella adiacens. Indian Heart J. 2013;65:447-9.
- [Google Scholar]
- Granulicatella adiacens isolated from sterile body fluids: A case series from India. Int J Case Rep Imag. 2014;5:802-7.
- [Google Scholar]
- Granulicatella infection: Diagnosis and management. J Med Microbiol. 2012;61(Pt 6):755-61.
- [Google Scholar]
- Evaluation of E test as a rapid method for determining MICs for nutritionally variant streptococci. J Clin Microbiol. 1994;32:2318-20.
- [Google Scholar]
- Performance of E test for antimicrobial susceptibility testing of Abiotrophia defective and Granulicatella species. J Clin Microbiol. 2016;54:2194-6.
- [Google Scholar]
- Antimicrobial susceptibilities of Abiotrophia defectiva, Granulicatella adiacens and Granulicatella elegans. Antimicrob Agents Chemother. 2016;60:1411-20.
- [Google Scholar]
- Granulicatella adiacens: An unusual isolate from urethral discharge. Indian J Med Microbiol. 2016;34:403-5.
- [Google Scholar]



