
Translate this page into:
Hospital Acquired Infections: Preventable Cause of Mortality in Spinal Cord Injury Patients
Address for correspondence: Dr. Purva Mathur, E-mail: purvamathur@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
There is an alarming rate of morbidity and mortality observed in the trauma victims who suffer spinal cord injuries (SCI). Such patients are admitted immediately and stay for longer periods of time and thus are at risk of acquiring nosocomial infections.
Aims:
The aim of this study is to analyze the primary cause of mortality in SCI patients.
Design:
Retrospective study.
Materials and Methods:
We conducted a retrospective 4 year analysis of the postmortem data of 341 patients who died after sustaining SCI at a tertiary care apex trauma center of India. Epidemiological data of patients including the type of trauma, duration of hospital stay, cause of death and microbiological data were recorded.
Results:
On autopsy, out of 341 patients, the main cause of death in the SCI patients was ascertained to be infection/septicemia in 180 (52.7%) patients, the rest 161 (47.2%) died due to severe primary injury. Respiratory tract infections (36.4%) were predominant followed by urinary tract infections (32.2%), blood stream infections (22.2%), wound infections (7.1%) and meningitis reported in only 5 (2.1%) cases. Acinetobacter sp (40%) was the predominant organism isolated, followed by Pseudomonas sp (16.3%), Klebsiella sp (15.1%), Candida sp (7.8%), Escherichia coli (6.9%), Staphylococcus aureus (6.9%), Proteus sp (3.3%), Enterobacter sp and Burkholderia sp (two cases each) and Stenotrophomonas sp (one case). A high level of multidrug resistance was observed.
Conclusions:
Hospital acquired infections (HAI) are leading cause of loss of young lives in trauma patients; hence efforts should be made to prevent HAIs.
Keywords
Hospital acquired infections
level of injury
multidrug resistance
respiratory tract infections
spinal cord injury
urinary tract infections

INTRODUCTION
The consequences of a spinal cord injury (SCI) leave behind a trail of tragic events in the patient's life resulting in negativity in all parameters of their life including physical, emotional, social and financial cost.[1] Majority of the cases of SCI are reported after road traffic accidents (RTA) and falls.[2] These traumatic events primarily take their toll on the young economically productive population of the country. Impairments associated with SCI predispose them to infections during the acute as well as chronic stages leading to premature deaths of the victims. They are at an increased risk of developing hospital acquired infections (HAI) especially with multidrug resistant organisms (MDRO) as they stay for prolonged periods in the hospital and are thus exposed to a number of antibiotics.[345] Hence, the health professionals must be cognizant of the fact that infections in these patients are inevitable and should be dealt with stringency to have a positive influence in the lives of these patients. There is a growing burden of trauma morbidity in India, but literature regarding mortality in SCI is scarce from our country. Though there has been a lot of research across the world on the long term survival of patients with SCI, there is a dearth of the literature on the acute causes of mortality in such patients. It has been observed that improvements in the acute critical care lead to a higher life expectancy of these patients.[6] Hence, this study was undertaken to obtain a preliminary overview of the epidemiological profile and the acute causes of mortality in SCI patients.
MATERIALS AND METHODS
The study was conducted at the Jai Prakash Narayan Apex Trauma Center, a 152 bedded level-1 trauma center of the All India Institute of Medical Sciences, which is a tertiary referral and teaching hospital of India.
It is a retrospective 4-year analysis of the postmortem data of all patients who had sustained traumatic SCI and succumbed to it. For each patient, the epidemiological features, the type of trauma, duration of hospital stay and the cause of death and the microbiological data of infections were noted from the clinical records and the autopsy files. Various infections were defined according to the microbiological reports and associated clinical features of patients. The percentage resistance of the isolated organisms to the commonly available drugs was observed. MDRO were defined as microorganisms that were resistant to one or more therapeutic classes of antimicrobial agents.[7]
RESULTS
During the study period of 2008-2011, autopsy was conducted for a total of 341 patients who had succumbed to SCI. The mean age of the study population was 37.03 years. We observed male gender predominance with 288 (84.45%) males in the study group.
The major causes of SCI were fall from heights in 151 (44.3%) cases, RTA in 144 (42.2%) cases followed by fall of heavy object in 16 (4.7%), firearm injuries in 10 (2.9%), train accident in 9 (2.6%), electrocution in 6 (1.8%), assault in 2 (0.6%), stab injuries in 2 (0.6%) and hit by a bull in 1 (0.3%) cases.
The primary site of SCI was cervical in 259 (75.9%), thoracic in 51 (14.9%), lumbar in 24 (7.0%) cases and thoracolumbar in 7 (2.1%) cases. Concomitant injuries to the head were present in 109 (31.9%) cases, injuries to chest in 62 (18.2%) cases, abdomen in 76 (22.2%) cases, lower limb in 20 (5.8%), upper limb in 14 (4.1%) and face or neck in 9 (2.6%) cases.
Out of the 341 fatal cases, the main cause of mortality was analyzed to be due to be septicemia infection, being reported in 180 (52.78%) subjects. Amongst the rest 161 (47.21%) patients, severe primary injury was the cause of mortality, with 41 out of them brought dead to the hospital.
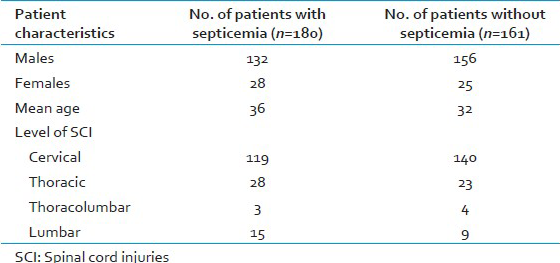
Amongst the cases with mortality due to infection and those without any evidence of infection, there was no significant difference observed in age, gender or level of SCI as elaborated in Table 1.
Out of 180 septicemia cases, 169 (93.8%) cases had a duration of stay of more than 48 hours in the hospital and had no evidence of any past infection or any infection incubating at the time of admission to the hospital. They were defined as having HAI. A review of the microbiological reports revealed that, a total of 239 episodes of infection were reported in these 180 cases. Of these, the maximum episodes of infections were found to be respiratory tract infections (RTI) in 87 (36.40%), followed by 77 (32.2%) episodes of urinary tract infections (UTIs), 53 (22.2%) blood stream infection episodes, 17 (7.1%) episodes of wound infections and 5 (2.1%) episodes of meningitis. A total of 245 organisms were isolated from these 239 episodes of infections. The predominant organism was the Acinetobacter sp isolated in 98 (40%) episodes. Other organisms isolated were the Pseudomonas sp in 40 (16.3%) episodes, Klebsiella sp in 37 (15.1%) episodes, Escherichia coli in 17 (6.9%) episodes, Proteus sp in 8 (3.3%) episodes, Enterobacter sp and Burkholderia sp in 2 (0.8%) episodes each and Stenotrophomonas sp in 1 episode. The Gram positive organisms isolated were Staphylococcus sp in 17 (6.9%) episodes and Enterococcus sp in 4 (1.6%) episodes. Candida sp was isolated in 19 (7.8%) episodes. A high level of resistance amongst the Gram negative as well as Gram positive bacteria to the commonly used antibiotics was observed in the deceased cases. The percentage of multidrug resistance observed is shown in Figure 1. Vancomycin resistance was not observed in any of Staphylococcus species and Enterococcus species.
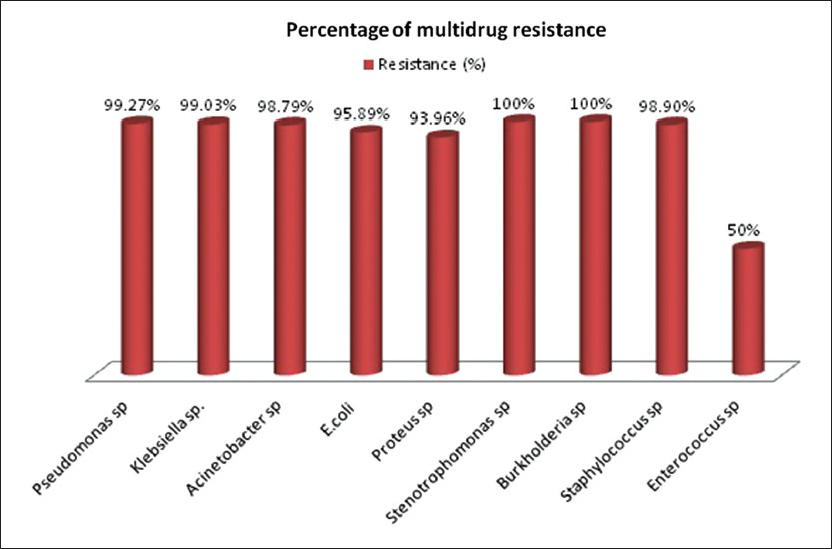
- Multidrug resistance observed in isolated organisms (X-axis: Distribution of organisms; Y-axis: Percentage resistance)
DISCUSSION
Over the years, improvement in the availability of pre-hospital treatment to trauma victims has had a significant impact on the number of people reaching the hospital alive. In the Indian scenario, every year there are approximate 20,000 new cases of SCI in trauma victims.[8] Hence, this study was conducted to see the primary causes of mortality in SCI patients once they reach the hospital alive so that some expeditious measures can be taken to deter the fatal outcome of these patients.
Out of 341 SCI patients, HAI were observed in 169 cases, ultimately leading to septicemia and mortality. Many of studies have acknowledged HAIs as a common complication in persons with SCI, either occurring during initial hospitalization after injury or during subsequent hospitalizations for long-term care of injuries and other problems. This frequent and often prolonged hospitalization leads to increased risk of acquiring antibiotic-resistant micro-organisms.[35]
Recent literature shows that leading cause of early mortality in SCI patients is pneumonia and septicemia.[9] In the present study also, we observed that infections are an important cause of mortality in these patients, with the RTI being the most common factors that predispose patients with SCI to develop pneumonia or other RTIs include weakness of the diaphragmatic and intercostal muscles, that would impair the capacity to clear respiratory secretions; indwelling respiratory devices, such as endotracheal or tracheostomy tubes and aspiration provoked by either associated head injury, the state of unconsciousness or due to illicit drug ingestion.[10] Hence, there should be increased clinical vigilance oriented toward measures to prevent these factors leading to RTIs. The second most common infection in our study group was the UTIs. This population is vulnerable to develop UTIs due to bladder catheterization and urinary stasis, hence leading to impaired emptying of the bladder, giving rise to localized infection and thus serving as a potential source of septicemia.[11]
We also analyzed that infections are an independent predictors of mortality since others epidemiological factors such as age, gender or level of injury showed no significant difference in patients with and without septicemia.
There is a dearth of literature on the epidemiology of HAI in SCI patients and one such study by Evans et al. concluded that the most common organisms isolated were the Gram positive organisms followed by the Gram negative organisms, most common being the Pseudomonas sp.[5] However, we observed the predominance of Gram negative organisms compared with Gram positive organisms and Acinetobacter sp was the most common isolate. To the best of our knowledge, no such studies have been performed in the Indian set up. We also noticed a very high level of resistance in our study with most of the organisms being multidrug resistant. Due to prolonged stay in the hospitals, these patients are at an increased risk of developing infections with resistant microorganisms.[35]
The neurological assessment or the spinal level of injury is valuable to ascertain clinical diagnosis, monitoring and prediction of functional outcomes. It has been reviewed that tetraplegics are more likely to die as compared with paraplegics.[12] In our study amongst the fatal cases of SCI, we had patients with cervical injuries in almost 75.9% of the cases highlighting the fatal prognosis of these cases.
In all Indian series, fall from height rates highest among the etiological factors, whereas, in advanced countries, the major culprits are the RTA.[13] Hence we need preventive measures and strategies to target both falls and RTAs to reduce the frequencies of SCI. The most common age group affected from various parts of India and World is from 20 to 29 years, signifying higher incidence in young, active and productive population of the society.[1415] An almost similar trend was observed in our study group also. Higher incidence in males can be explained by the fact that they are more exposed to risk factors owing to their much more travelling and other activities making them vulnerable to falls and RTAs.
Nearly, 32% of our study population suffered concomitant head injuries and it has been established previously that such patients have a further heightened level of morbidity, requiring complex rehabilitation.[16] Those who are injured in traffic accidents and falls run a particular risk of sustaining a concomitant head injury and they are especially associated with cervical SCI.[2]
CONCLUSION
There should be diligent enforcement of all practices to alleviate the burden of HAI in SCI patients who are especially prone to them. This study would be beneficial to understand the epidemiology of SCI in our society. Further research is required in this area to help assist the proper allocation of resources to improve the prognosis of these patients in remediable circumstances.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Epidemiology map of traumatic spinal cord injuries: A global overview. Int J Caring Sci. 2012;5:335-47.
- [Google Scholar]
- Traumatic spinal cord injuries: Incidence, mechanisms and course. Tidsskr Nor Laegeforen. 2012;132:831-7.
- [Google Scholar]
- Infections in patients with spinal cord injuries. Clin Infect Dis. 1997;25:1285-90. 1291
- [Google Scholar]
- Long-term outcomes from nosocomial infections in persons with spinal cord injuries and disorders. Am J Infect Control. 2007;35:393-400.
- [Google Scholar]
- Epidemiology of hospital-acquired infections in veterans with spinal cord injury and disorder. Infect Control Hosp Epidemiol. 2008;29:234-42.
- [Google Scholar]
- Survival after spinal cord injury: A systematic review. J Neurotrauma. 2010;27:1517-28.
- [Google Scholar]
- Taumatic spinal cord injuries in Haryana: An epidemiological study. Indian J Community Med. 2003;28:10-2.
- [Google Scholar]
- Mortality in patients with traumatic spinal cord injury: Descriptive analysis of 62 deceased subjects. J Spinal Cord Med. 2011;34:482-7.
- [Google Scholar]
- Incidence of respiratory complications following spinal cord injury. Arch Phys Med Rehabil. 1994;75:270-5.
- [Google Scholar]
- Urinary tract infection in spinal cord injury. Arch Phys Med Rehabil. 1989;70:47-54.
- [Google Scholar]
- Long-term survival in spinal cord injury: A fifty year investigation. Spinal Cord. 1998;36:266-74.
- [Google Scholar]
- Review paper: Epidemiology of traumatic spinal cord injury: Comparisons between developed and developing countries. Asia Pac J Public Health. 2010;22:9-18.
- [Google Scholar]
- Manual of Patna model for the care of spinal cord injury patients. Patna: SPARSH; 2000. p. :9-13.
- [Google Scholar]
- Traumatic spinal cord injuries in Turkey: A nation-wide epidemiological study. Spinal Cord. 2000;38:697-701.
- [Google Scholar]
- The therapeutic challenges of dual diagnosis: TBI/SCI. Brain Inj. 2004;18:1297-308.
- [Google Scholar]
- Management of multidrug-resistant organisms in health care settings, 2006. Am J Infect Control. 2007;35:S165-93.
- [Google Scholar]



