
Translate this page into:
In Vitro Susceptibility of Burkholderia pseudomallei Isolates to Cefiderocol and Ceftazidime/Avibactam from Odisha, India
 , Gayatree Nayak1, Srujana Mohanty1, Ashoka Mahapatra1, Prashanth Purushotham1, Anjuna Radhakrishnan1, Manaswiny Tripathy1
, Gayatree Nayak1, Srujana Mohanty1, Ashoka Mahapatra1, Prashanth Purushotham1, Anjuna Radhakrishnan1, Manaswiny Tripathy1
Address for correspondence: Bijayini Behera, MD Microbiology, Department of Microbiology, All India Institute of Medical Sciences (AIIMS), Bhubaneswar, Odisha 751019, India (e-mail: drbinny2004@gmail.com).
-
Received: ,
Accepted: ,
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction and Objectives
The availability of a limited arsenal of antibacterial agents effective against Burkholderia pseudomallei, the causative agent of melioidosis, together with sporadic reports of emergence of resistance necessitates an evaluation of in vitro activity of new antimicrobials against clinical B. pseudomallei isolates. Cefiderocol (CFDC), a novel siderophore cephalosporin, and ceftazidime-avibactam (CZA), a new β lactam combination agent, have shown promising results for the treatment of difficult-to-treat Gram-negative bacilli infections with limited treatment options. This study was conducted to determine the in vitro activity of CFDC and CZA against a contemporary collection of 60 B. pseudomallei clinical isolates.
Materials and Methods
Minimum inhibitory concentrations (MIC) of CFDC and CZA were determined by broth microdilution and E-test, respectively. The performance of disk diffusion was also evaluated for CFDC.
Results
All B. pseudomallei isolates were susceptible to CFDC and CZA with MIC range of 0.125 to 2 mg/L and 0.19 to 1 mg/L, respectively. Zone diameters for CFDC ranged from 31 to 40 mm.
Conclusion
CFDC and CZA exhibited excellent in vitro activity against 60 B. pseudomallei isolates. Further pharmacokinetic-pharmacodynamics studies and clinical trials are needed to prove the clinical efficacy of CFDC and CZA in the treatment of melioidosis.
Keywords
Burkholderia pseudomallei
Cefiderocol
Ceftazidimeavibactam

Introduction
Melioidosis, with myriad clinical manifestations encompassing acute, rapidly progressing septicemic infection with or without underlying focus to chronic, persistent, localized infections, often confounds initial diagnostic assessment, and thus initiation of appropriate antimicrobial therapy. The antimicrobial therapy is biphasic with an initial intensive phase with intravenous ceftazidime or carbapenem with or without co-trimoxazole depending upon the site and extent of disease involvement. The duration of the intensive phase ranges from 2 to 8 weeks and is again determined by extent, site of disease along with the duration of blood culture positivity.[1] The eradication phase is aimed at preventing relapse and requires at least 3 months of treatment with oral co-trimoxazole as the first choice and amoxicillin-clavulanic acid or doxycycline as alternatives.[2] The limited arsenal of antibacterial agents available for the intensive phase is due to the robust intrinsic resistance mechanisms of B. pseudomallei. There are sporadic reports of the emergence of resistance to ceftazidime as well as carbapenems, mostly during treatment and occasional reports of de novo resistance to these drugs, from various endemic countries including India.[3–7] Resistance to ceftazidime can be mediated by upregulation or amino acid substitution of the β-lactamase-encoding gene penA or the deletion of penicillin-binding protein 3 (PBP3).[2] Mutations in the multidrug resistance-nodulation-division efflux pump regulators often account for decreased meropenem susceptibility.[8]
Cefiderocol (CFDC) a novel siderophore cephalosporin employs an undercover trojan horse like strategy to gain access to the periplasmic space thus overcoming resistance barriers like porin loss, efflux pump in Gram-negative bacilli (GNB).[9] Ceftazidime-avibactam (CZA) is a new β lactam combination agent. Ceftazidime coupled with non-β-lactam β-lactamase inhibitor avibactam (CZA) diminishes the availability of active site of β-lactamases for hydrolysis.[10] Both CFDC and CZA have shown promise for the treatment of difficult to treat GNB infections with limited treatment options, including nonfermenting GNB (NF-GNB).[9,10] There are only a handful of literature available regarding the activity of CFDC and CZA against clinical B. pseudomallei isolates, and none from India. Hence, this study was conducted to determine the in vitro activity of CFDC and CZA against a contemporary collection of B. pseudomallei isolates.
Method
Bacterial Isolates
A total of 60 stored clinical B. pseudomallei isolates (recovered from 60 patients with culture-confirmed melioidosis, from 2018–21, kept in glycerol stocks at −80°C) were revived by inoculating in tryptic soy broth, and incubation at 37°C for 5 to 7 days. Subcultures were performed on Sheep blood agar, MacConkey agar, and Ashdown agar, and plates were incubated at 37°C. Isolate identification was confirmed by conventional-polymerase chain reaction targeting a type III secretion system gene cluster.[11] The collection composed primarily of bloodstream (46.6%,28/60), followed by skin and soft tissue (41.6%,25/50), and respiratory (7/60,11.6%) isolates. Out of 60 patients, a favorable outcome was noted in 46 (47/60,76.6%), eight patients succumbed to the disease (8/60,13.3%), and three patients each had relapsed and left hospital against medical advice. The antimicrobial susceptibility of the isolates to ceftazidime, imipenem, meropenem, co-trimoxazole, doxycycline, and amoxicillin-clavulanic acid was determined by E-test. There was no association between drug resistance and mortality. The study was approved by the Institute Ethics Committee [T/IM-NF/Micro/21/177, dated 31.03.22].
CFDC MIC Determination
Pure powder of CFDC was obtained from Chemscene India Pvt Ltd. CFDC stock solution (1,000 μg/mL) was prepared in normal saline, and a range of working concentrations (0.125–16 µg/mL) were made by serial twofold dilutions. For CFDC minimum inhibitory concentrations (MIC) determination, iron-depleted cation adjusted Muller Hinton broth (ID-CAMHB) was prepared as per Clinical & Laboratory Standards Institute (CLSI) recommendations.[12,13] Iron-chelating agent [Chelex 100 sodium, Sigma Aldrich: C7901-25G] was added in a ratio of 1:10 to double strength CAMHB (Sigma Aldrich:90922) with continuous stirring in a magnetic stirrer for 2 hours. Calcium (22.5 mg/L as Ca2+), magnesium (11.25 mg/L as Mg2+), and zinc (10 µM as ZnSO4) corresponding to 0.65 mg/L as Zn2+) were added to the ID- CAMHB to replenish the desired cations. Final concentrations of ions (iron, calcium, magnesium, and zinc) of the prepared ID-CAMHB were measured using atomic emission spectrometry for iron and zinc and inductive coupled plasma-optical emission spectrometry for calcium and magnesium. ID-CAMHB after cation reconstitution was sterilized by 0.22µm hydrophilic polytetrafluoroethylene syringe filter and the pH was adjusted to (7.2–7.4) with 1N hydrochloric acid. For CFDC broth microdilution (BMD), in order to achieve 100 µL of volume in each well of the 96-well polystyrene plate, 25 µL of reconstituted CFDC of various concentration, 25 µL B. pseudomallei inoculum of concentration (5 × 105 CFU/mL), and 50 µL of ID-CAMHB were added and incubated at 35 ± 2°C for 16 to 20 hours. MIC was interpreted as the lowest concentration of CFDC that completely inhibited visible growth of B. pseudomallei in the wells as detected by the unaided eye.
CZA MIC Determination
CZA E-test was performed by using CZA MIC-strips (CZA 256, Biomerieux, Diagnostics, USA) on Muller Hinton agar (MHA) as per manufacturer's instructions. In the CZA E-test strip, ceftazidime concentrations range from 0.016 to 256 μg/mL and the concentration of avibactam is fixed at 4 μg/mL. E-test end-points were interpreted visually by the unaided eye.
CFDC Disk Diffusion
Disk diffusion (DD) was performed on unsupplemented MHA using 30μg Cefiderocol disk (FDC 30 µg, Liofilchem, s.r.l., Roseto Degli Abruzzi, Teramo, Italy) as per CLSI recommendations.[12,13]
Control Strains
Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as control strains for BMD, E-TEST, and DD.
Result Interpretation
CLSI-approved CFDC MIC clinical breakpoints for Enterobacterales, P. aeruginosa, and Acinetobacter species (≤4 mg/L [susceptible], 8 mg/L [intermediate], and ≥16 mg/L [resistant]) were used. For CZA, MIC less than or equal to 4 mg/L were regarded as susceptible, and MIC more than 8 mg/L were regarded as resistant as per CLSI clinical susceptibility breakpoints against Enterobacteriaceae and P. aeruginosa.
Results
CFDC MIC of B. pseudomallei
All isolates were susceptible to CFDC based on CLSI breakpoints of CFDC against Enterobacterales, P. aeruginosa, and Acinetobacter species. MIC range of 60 B. pseudomallei isolates was 0.125 to 2 mg/L. Of the 60 isolates, 54 (54/60, 90%) were inhibited at CFDC concentration of less than or equal to 0.5 mg/L and the remaining 6 (6/60,10%) were inhibited at 1 and 2 mg/ L. Both MIC50 and MIC90 were 0.5mg/L (►Table 1).
| B. pseudomallei (n = 60) | No. of isolates at cefiderocol MIC (mg/L) (≤4 mg/L [susceptible], 8 mg/L [intermediate], and ≥16 mg/L [resistant])a |
|||||||
|---|---|---|---|---|---|---|---|---|
| 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | |
| 5 | 23 | 26 | 4 | 2 | 0 | 0 | 0 | |
Abbreviations: CLSI, Clinical & Laboratory Standards Institute; MICs, minimum inhibitory concentrations.
a CLSI cefiderocol MIC clinical breakpoints for Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter species. MIC clinical breakpoints for B. pseudomallei is currently not available.
CZA MIC of B. pseudomallei
All isolates were susceptible to CZA based on CLSI breakpoints of CZA against Enterobacterales, and P. aeruginosa. CZA MIC range of 60 B. pseudomallei isolates were 0.19 to 1 mg/L. Of the 60 isolates, 32 (32/60, 53.3%) were inhibited at CZA concentration of less than or equal to 0.5 mg/L and the remaining 28 (28/60,46.6%) were inhibited at 0.75 and 1 mg/ L. CZA MIC50 was 0.5mg/L (►Table 2). CZA E test of an isolate is depicted in ►Fig. 1.

- Ceftazidime-avibactam E test showing MIC of 0.5 mg/L.
| B. pseudomallei (n = 60) | No. of isolates at ceftazidime-avibactam MIC (mg/L): (≤4 mg/L [susceptible], and ≥8 mg/L [resistant])a |
||||||
|---|---|---|---|---|---|---|---|
| 0.19 | 0.25 | 0.38 | 0.5 | 0.75 | 1 | 1.5 | |
| 2 | 3 | 8 | 19 | 20 | 8 | 0 | |
Abbreviations: CLSI, Clinical & Laboratory Standards Institute; MICs, minimum inhibitory concentrations.
a CLSI ceftazidime-avibactam MIC clinical breakpoints against Enterobacteriaceae and Pseudomonas aeruginosa. MIC clinical breakpoints for B. pseudomallei is currently not available.
CFDC Disk Diffusion
All isolates were susceptible to CFDC based on CLSI CFDC DD breakpoints of against Pseudomonas aeruginosa, Acinetobacter baumannii. Zone diameters ranged from 31 to 40 mm. Correlation between CFDC zone diameter and MIC is presented in ►Fig. 2. MIC ranges of 60 clinical B. pseudomallei isolates to ceftazidime, carbapenem (imipenem and meropenem), Co-trimoxazole, amoxicillin-clavulanic acid and doxycycline, along with CFDC and CZA, are depicted in ►Table 3. All isolates retained susceptibility to all the antimicrobials tested, except two isolates which had high meropenem MIC. Those isolates were obtained from patients without meropenem treatment history and retained susceptibility to imipenem.
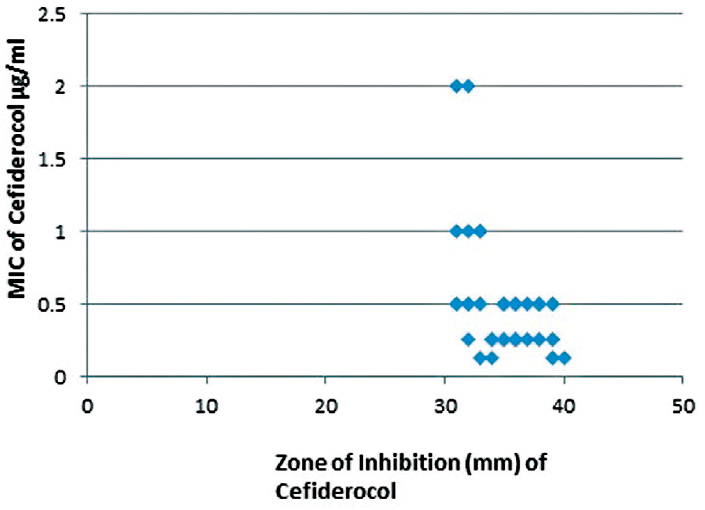
- Correlation of CFDC disc inhibition zone diameters and MIC values in 60 Burkholderia pseudomallei isolates.
| Serial no. | Antimicrobials and MIC breakpoints | MIC range (mg/L) | % susceptibility |
|---|---|---|---|
| 1 | Cefiderocol (≤4mg/L [S], 8 mg/L [I], ≥16 mg/L [R]) | 0.125–2 | 100 |
| 2 | Ceftazidime-avibactam (≤4mg/L [S], ≥8 mg/L [R]) | 0.19–1 | 100 |
| 3 | Ceftazidime (≤8 mg/L [S], 16 mg/L [I], ≥32 mg/L [R]) | 0.5–4 | 100 |
| 4 | Imipenem (≤4mg/L [S], 8 mg/L [I], ≥16 mg/L [R]) | 0.125–3 | 100 |
| 5 | Meropenem (≤4mg/L [S], 8 mg/L [I], ≥16 mg/L [R]) | 0.25–32 | 96.6 |
| 6 | Co-trimoxazole (≤2/38 mg/L [S] ≥4/76 mg/L [R]) | 0.032–2 | 100 |
| 7 | Amoxicillin-clavulanic acid (≤8/4mg/L [S], 16/8 mg/L [I], ≥32/16 mg/L [R]) | 1–4 | 100 |
| 8 | Doxycycline (≤4mg/L [S], 8 mg/L [I], ≥16 mg/L [R]) | 0.5–2 | 100 |
Abbreviations: I, intermediate; MIC, minimum inhibitory concentration; R, resistant; S, susceptible.
Discussion
Given the limited therapeutic choices during the intensive phase of melioidosis treatment, and sporadic reports of resistance to the first line antimicrobial agents, evaluation of efficacy of novel antimicrobial agents against clinical B. pseudomallei isolates becomes extremely justified. In our setting, two such recently launched therapeutic agents, CFDC and CZA, were found to have excellent in vitro activity against a contemporary collection of 60 clinical B. pseudomallei isolates. In the absence of CLSI clinical breakpoints for B. pseudomallei, we used the for Enterobacterales, P. aeruginosa, and Acinetobacter species for MIC interpretation of B. pseudomallei isolates (12,13). CFDC MIC50 and MIC 90 of 60 B. pseudomallei isolates in our study were 0.5 mg/L, slightly higher than MIC90 values of 0.125 mg/L of 246 clinical isolates of Burkholderia pseudomallei from Queensland, Australia, and MIC90 of 0.25 mg/L obtained from a study of 30 USAMRIID B. pseudomallei isolates.[14,15] In the Australian study, four isolates (1.6%, 4/246) were categorized as nonsusceptible based on MIC more than 4 mg/L, in isolates without a prior treatment history with CFDC.[14] However, those isolates were from patients with significant co-morbidities, prior exposure to multiple antibiotics including β- lactams and also had co-expression of resistance to multiple antibiotics used for melioidosis treatment.[14] In our setting, though most of the B. pseudomallei isolates were from patients with multiple underlying risk factors and comorbidities, and two isolates had high meropenem MIC, all of them retained susceptibility to CFDC. BMD for CFDC is technically demanding, and requires careful monitoring at various steps including cation depletion, cation replenishment, and final pH adjustment.[12,13] The agreement and error rates of CFDC DD with BMD depend upon manufacturers of CFDC disc and CA-MHB as well as Genera of GNB.[16–18] In our study, overall zone diameters ranged from 31 to 40 mm. For B. pseudomallei isolates with MIC more than 0.5 mg/L, zone diameters did not exceed 33 mm. In the study by Burnard et al, for B. pseudomallei isolates with MICs between 1 and 4 mg/L, zone diameters ranged between 35 and 25 mm.[14] Relationship between CFDC zone diameter and MIC values can be better ascertained by including resistant isolates and isolates with wider MIC distribution.
In this study, CZA MIC range of 60 clinical B. pseudomallei isolates was 0.19 to 1 mg/L. In the study from Thailand by Sribenjalux et al, CZA MIC50 of 28 clinical B. pseudomallei isolates was 0.75 mg/L.[19] Ceftazidime resistance in clinical B. pseudomallei isolates remains low, and there is a chance of underestimation of ceftazidime resistance during therapy. A recent study concluded that ceftazidime-resistant isolates with underlying PBP3 deletion fail to grow on routine laboratory media unless supplemented with glycerol and thus during or after ceftazidime therapy, samples can be plated onto glycerol containing media such as Ashdown to promote the growth of ceftazidime-resistant variants.[4] In a study by Chirakul et al, ceftazidime resistance in a clinical B. pseudomallei isolate had been shown to be completely reversed in vitro by addition of avibactam.[20] In this study, CZA MIC of 60 clinical B. pseudomallei isolates were two to fourfold lower than that of ceftazidime alone. These in vitro studies including ours show a promising role of CZA in therapy of ceftazidime-resistant B. pseudomallei as a carbapenem sparer agent.[19,20]
This study, conducted on 60 isolates from a single tertiary center healthcare facility, provides the in vitro activity of cefiderocol and CZA, for the first time for B. pseudomallei isolates from India. Further pharmacokinetic-pharmacodynamics studies and clinical trials are needed to prove clinical efficacy of cefiderocol and CZA in the treatment of melioidosis.
Conflict of Interest
None declared.
Funding
None.
References
- 2020 Review and revision of the 2015 Darwin melioidosis treatment guideline; paradigm drift not shift. PLoS Negl Trop Dis. 2020;14(09):e0008659.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanisms of antibiotic resistance in Burkholderia pseudomallei: implications for treatment of melioidosis. Future Microbiol. 2012;7(12):1389-1399.
- [CrossRef] [PubMed] [Google Scholar]
- Characterization of ceftazidime resistance mechanisms in clinical isolates of Burkholderia pseudomallei from Australia. PLoS One. 2012;7(02):e30789.
- [CrossRef] [PubMed] [Google Scholar]
- Antimicrobial resistance to ceftazidime involving loss of penicillin-binding protein 3 in Burkholderia pseudomallei. Proc Natl Acad Sci U S A. 2011;108(41):17165-17170.
- [CrossRef] [PubMed] [Google Scholar]
- Development of ceftazidime resistance in an acute Burkholderia pseudomallei infection. Infect Drug Resist. 2012;5:129-132.
- [CrossRef] [PubMed] [Google Scholar]
- Development of ceftazidime resistance in Burkhoderia pseudomallei in a patient experiencing melioidosis with mediastinal lymphadenitis. Ann Acad Med Singap. 2010;39(12):945-3.
- [CrossRef] [PubMed] [Google Scholar]
- Ceftazidime resistance in Burkholderia pseudomallei: first report from India. Asian Pac J Trop Med. 2012;5(04):329-330.
- [CrossRef] [PubMed] [Google Scholar]
- Raising the Stakes: loss of efflux pump regulation decreases meropenem susceptibility in Burkholderia pseudomallei. Clin Infect Dis. 2018;67(02):243-250.
- [CrossRef] [PubMed] [Google Scholar]
- Cefiderocol: a novel siderophore cephalosporin for multidrug-resistant gram-negative bacterial infections. J Antimicrob Chemother. 2021;76(06):1379-1391.
- [CrossRef] [PubMed] [Google Scholar]
- Ceftazidime-avibactam: a review in the treatment of serious gram-negative bacterial infections. Drugs. 2018;78(06):675-692.
- [CrossRef] [PubMed] [Google Scholar]
- Improved detection of Burkholderia pseudomallei from non-blood clinical specimens using enrichment culture and PCR: narrowing diagnostic gap in resource-constrained settings. Trop Med Int Health. 2017;22(07):866-870.
- [CrossRef] [PubMed] [Google Scholar]
- Performance Standards for Antimicrobial Susceptibility Testing; Twenty Ninth Informational Supplement. Wayne, PA: Clinical and Laboratory Standards Institute; 2019. p. :M100-S29.
- [Google Scholar]
- 2020. Performance Standards for Antimicrobial Susceptibility Testing; Thirtieth Informational Supplement. Wayne, PA: Clinical and Laboratory Standards Institute; 2020. p. :M100-S30.
- [Google Scholar]
- Burkholderia pseudomallei clinical isolates are highly susceptible in vitro to cefiderocol, a siderophore cephalosporin. Antimicrob Agents Chemother. 2021;65(02):e00685-e20.
- [CrossRef] [PubMed] [Google Scholar]
- S-649266, a novel siderophore cephalosporin: in vitro activity against biothreat pathogen. Open Forum Infect Dis. 2016;3(Suppl 1):1832.
- [CrossRef] [Google Scholar]
- Cefiderocol antimicrobial susceptibility testing against multidrug-resistant gram-negative Bacilli: a comparison of disk diffusion to broth microdilution. J Clin Microbiol. 2020;59(01):e01649-e20.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of disk diffusion, MIC test strip and broth microdilution methods for cefiderocol susceptibility testing on carbapenem-resistant enterobacterales. Clin Microbiol Infect. 2022;28(08):1156-e1-1156.e5.
- [CrossRef] [PubMed] [Google Scholar]
- Cefiderocol: EUCAST criteria for disc diffusion and broth microdilution for antimicrobial susceptibility testing. J Antimicrob Chemother. 2022;77(06):1662-1669.
- [CrossRef] [PubMed] [Google Scholar]
- In vitro susceptibility of Burkholderia pseudomallei isolates from Thai patients to ceftolozane/tazobactam and ceftazidime/avibactam. J Glob Antimicrob Resist. 2022;28:8-11.
- [CrossRef] [PubMed] [Google Scholar]
- Burkholderia pseudomallei acquired ceftazidime resistance due to gene duplication and amplification. Int J Antimicrob Agents. 2019;53(05):582-588.
- [CrossRef] [PubMed] [Google Scholar]



