
Translate this page into:
Isolated Plexiform Neurofibroma of the Tongue
Address for correspondence: Dr. Abhishek Sharma, E-mail: abhshk79@rediffmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Neurofibromas (NF) are benign tumors of neural origin, of which roughly 90% appear as solitary lesions. They are classified into cutaneous, subcutaneous, and plexiform subtypes. Plexiform neurofibromas are the least common variant and usually are pathognomonic for NF I. Here, we present a very rare case of isolated plexiform neurofibroma with a painless enlarging mass of the tongue of an 11-year-old girl. This rare benign tumor has the potential for malignant transformation, and the diagnosis was difficult owing to the patient's age and to the insidious clinical presentation. The present case is a diffuse isolated plexiform neurofibroma of the tongue that was not associated with neurofibromatosis that was treated with intraoral surgery.
Keywords
Hemimacroglossia
plexiform neurofibroma
tongue

INTRODUCTION
Plexiform neurofibroma is the term applied to a diffuse neurofibromatosis of nerve trunks, which is often associated with an overgrowth of the skin and subcutaneous tissues. It is a distinct type of neurofibroma that expands a nerve into a large tortuous mass of fibers that has a “bag of worms” appearance.[1] Neurofibromatosis is classified into cutaneous, subcutaneous, and plexiform subtypes. Plexiform neurofibromas are the least common variant and usually are pathognomonic for NF I. The most commonly involved sites are the temple, upper lid, back of the neck, and the tongue.[23] Oral manifestations of neurofibromatosis have been reported in only 4-7% affected persons, in which the tongue was the most commonly involved site.[4]
This systemic process, originally described by von Recklinghausen, is an autosomal dominant disorder caused by a defect on chromosome 17. Patients usually present in childhood with numerous cutaneous or subcutaneous neurofibromas, melanotic lesions in the iris called Lisch nodules, café au lait spots, and optic gliomas.[2] Plexiform neurofibromas occur in only 17% of cases of NF I. When they occur in the setting of NF I, 91% are solitary lesions, and most of the lesions occur in the trunk, extremities, and head neck region.[2] These lesions are often locally invasive and may undergo malignant transformation. Histologically, neurofibroma consist of endoneural ground substance and Schwann cells that extend outside the perineurium. Neurofibromas may also have a sarcomatous transformation in 3-15% of cases.[5] Prognosis is usually poor because of recurrences and risk of malignant transformation. Here, we present a case of an isolated plexiform neurofibroma of the tongue in a 11-year-old girl not associated with neurofibromatosis.
CASE REPORT
An 11-year-old girl was admitted to the department of E.N.T. of our institute, with the complaint of inability to close the mouth because of a large, asymmetrical, protruding tongue. The girl had difficulty in swallowing, breathing, and clear speaking since early months of her life. On palpation, the right side of the tongue was hypertrophied and the movements of the tongue were normal, but she was unable to hold the tongue completely in the mouth because of its enormous size. The swelling was soft, nontender, nonreducible, and nonpulsatile on palpation. There was also slight generalized swelling of the right side of the base of the tongue. No neck glands were palpable and functions of V, VII, X, and XII cranial nerves were intact. A magnetic resonance image was obtained to better assess the base of tongue, which revealed a 3 × 3 × 2.5 cm heterogeneously enhancing mass with infiltration in the tongue and tongue base, this lesion was hypervascular and well-circumscribed. Under general anesthesia, a deep biopsy was taken from the tongue. Gross examination of the specimen revealed irregular surface which was soft in consistency [Figure 1]. Histopathological examination revealed well circumscribed multiple nodular lesions composed of elongated spindle wavy cells with muscle fibers in between, these wavy cells were arranged against a myxoid background. No atypia or increase in mitosis was seen [Figures 2 and 3]. An ophthalmologic examination was carried out which showed no eye lesions of neurofibromatosis (such as Lisch nodules in the iris, ephelides on eyelids, or ectopia lentis). The skin of the whole body was examined and no café au lait spots or frecklings of the axillary and inguinal region were observed. On plain radiograph, no bone pathology was found. After the diagnostic work-up, surgical treatment was planned. Under general anesthesia, the tumor was approached intraorally, and the biopsy report was consistent with plexiform neurofibroma. Postoperatively, a remarkable reduction in the size of the tongue was achieved. The movements of the tongue were preserved, and, in addition, a significant improvement in her speech was observed. The patient has been on follow-up for 10 months and no additional treatment has been necessary.

- Gross picture of neurofibroma

- H and E-stained section showing spindle wavy-shaped cells seperated by fibromyxoid stroma, ×400
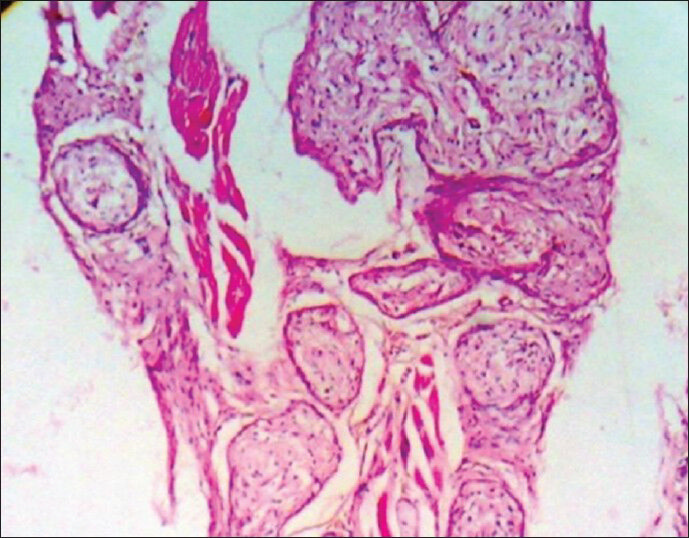
- H and E-stained section showing discrete well-circumscribed collection of spindle cells with muscle fibers in between, ×100
DISCUSSION
Neurofibromas are benign tumors of neural origin, of which roughly 90% appear as solitary lesions. Solitary plexiform neurofibromas arising outside the context of NF I, as illustrated in the patient presented here, are quite rare, with only scattered cases reported in the literature till date.
In the literature, there are only few reports of macroglossia caused by plexiform neurofibroma, and the cases are almost always associated with neurofibromatosis.[45] Hence, isolated plexiform neurofibroma is even rarer. Our patient had no eye lesion, no bone pathology, and no café au lait spots or frecklings on the skin. We could not find any other signs or symptoms other than isolated plexiform neurofibroma of the tongue to make a diagnosis of neurofibromatosis, and thus it was concluded to be a case of isolated plexiform neurofibroma of the tongue.[5] When these ill-defined tumors grow in the head and neck, they are commonly symptomatic and disfiguring, causing upper airway obstruction, swallowing or mastication difficulties, or cosmetic distortion of the face.[6] Plexiform neurofibromas mostly appear within first 2 years of life. There are two types of plexiform neurofibromas, nodular and diffuse. Diffuse plexiform neurofibroma, is also known as elephantiasis neurofibromatosa, which shows overgrowth of epidermal and subcutaneous tissue along with a wrinkled and pendulous appearance.
Neurofibromas of the large nerves, which appear clinically as soft, drooping, and doughy masses, are benign neoplasms composed of neurites, Schwann's cells and fibroblasts within a collagenous or myxoid matrix. In contrast to schwannomas, they are nonencapsulated and engulf the nerve of origin. Plexiform neurofibromas, forming tortuous cords along the segments and branches of a nerve with a tendency to grow centripetally, are poorly circumscribed tumors. It needs to be differentiated from schwannoma which is encapsulated, while plexiform neurofibroma is noncapsulated; moreover, in schwannoma there are antony A and antony B along with prescence of verocay bodies on microscopic examination. Since neurofibromas are usually multiple lesions, the whole body must be examined and investigated. In patient with oral neurofibroma, larynx and trachea must also be examined as in such a case lesions in the upper airway may cause respiratory obstruction. Plexiform neurofibromas should be monitored frequently because 5% may turn into malignant peripheral nerve sheath tumors.[3456]
Differential diagnosis of such a tongue mass must include neurofibroma, schwannoma (neurilemoma), lymphangioma, hemangioma, hamartoma, teratoma, pyogenic granuloma, nerve sheath myxoma, and cystic lesions such as mucoid cysts and dermoid cysts.
The standard treatment for neurofibromas has been surgical excision and the diagnosis can only be confirmed by histological examination. Neurofibromas have extensive vascularity and tend to bleed during surgery. Therefore, excessive bleeding should be kept in mind while attempting surgical removal. Early diagnosis in such a patient is very important and these patients need regular follow-up during their lifetime to detect recurrences. Fortunately, there were no signs of recurrence or other manifestations during the follow-up period of our patient till date.
CONCLUSION
Isolated plexiform neurofibroma of the tongue is a rare tumor. Here, we present this case for its rare site along with nonassociation with neurofibromatosis, excellent recovery, and no recurrence till date on follow-up.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Hemimacroglossia caused by isolated plexiform neurofibroma: A case report. Laryngoscope. 2006;116:151-3.
- [Google Scholar]
- Solitary oral plexiform neurofibroma: Review of literature and report of a case. Oral Oncol. 2011;47:449-51.
- [Google Scholar]
- Plexiform neurofibroma of the tongue: A case report of a child. Turk J Pediatr. 2006;48:155-8.
- [Google Scholar]
- Oral plexiform neurofibroma not associated with neurofibromatosis type I: Case report. J Oral Sci. 2006;48:157-60.
- [Google Scholar]
- Solitary plexiform neurofibroma of the oral cavity: A case report. Int J Oral Maxillofac Surg. 1996;25:379-80.
- [Google Scholar]



