
Translate this page into:
Melioidosis as a Cause of Acute Abdomen in Immuno-Competent Male from Eastern India
Address for correspondence: Dr. Sagar Khadanga, E-mail: sagar.genmed@aiimsbhopal.edu.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Though melioidosis is rare in India, it has gained importance as one of the most potent emerging infections. In India, the cases have been under-reported because of the lack of awareness. The majority of cases present with multifocal pyogenic infections with septicemia. We present an unusual case of melioidosis presenting as acute intestinal perforation. The organism was ceftazidime resistant, and we successfully treated the case with imipenem and doxycyclin. This case highlights ruling out the possibility of melioidosis in acute abdomen and existence of ceftazidime resistant cases in India.
Keywords
Burkholderia pseudomallei
ceftazidime
India
melioidosis

INTRODUCTION
The first description of melioidosis goes way back to 1911 when Indian Bacteriologist C.S. Krishnaswami, under the guidance of the pathologist Whitmore, described a “glanders-like” disease among the morphine addicts in Rangoon, Burma.[12] Since then the causative agent has been named differently at different time and at present, the causative agent is known as Burkholderia pseudomallei. Nearly, a thousand of cases have been reported all over the world, predominantly from Southeast Asian countries (Thailand, Malaysia, Indonesia) and Australia.[3] The first report of melidosis from India was by Raghavan et al., from Mumbai in 1991.[4] Since then about fifty cases of the disease have been reported predominantly from the southern part of India.[5] Recently, it has gained attention as one of the most potent emerging infection in India. Lack of awareness of this disease among the Indian clinicians and microbiologists is responsible for misdiagnosing it as tuberculosis, scrub typhus, leptospirosis or brucellosis.[6]
The risk factors which have been described are diabetes mellitus, thalassemia, renal disease, chronic lung disease, chronic alcoholism, occupational exposure to soil and surface water, elderly males and immunosuppression due to any cause.[6] The incubation period is usually 1–21 days, but can be months to years.[7] Clinical presentation of melioidosis varies widely. It ranges from asymptomatic infection, acute fulminant sepsis, subacute multifocal abscesses to a chronic mild infection.[3] For confirmatory diagnosis of melioidosis serological and molecular methods have been evaluated in clinical setting but culture is still considered the gold standard.[6] In routine media like blood agar and MacConkey's agar growth takes longer than usual time (5–7 days). Ashdown's medium and modified Ashdown's medium have been described as the selective media.[8]
Melioidosis is difficult to treat as the bacteria are inherently resistant to most of the commonly used penicillins, cephalosporins, aminoglycosides, and quinolones.[9] Usual treatment is divided into two phases: Intensive phase, consisting of in-patient treatment for at least 10–14 days with ceftazidime or carbapenems (imipenem or meropenem) and eradication phase, consisting treatment with oral doxycyclin or cotrimoxazole (trimethoprim-sulfamethoxazole) for 3–6 months.[9]
CASE REPORT
A 48-year-old male from West Bengal, in eastern part of India, presented to the emergency department with complaints of sudden onset of pain and distension of abdomen for 2 h. The patient was having low-grade fever and cough with scanty expectoration for last 1-month along with weight loss of 3 kg during this period. With this clinical picture and bilateral upper zone opacities in X-ray chest [Figure 1], the patient was put on anti-tubercular therapy in another center (Directly Observed Treatment Shortcourse-Category I) though the sputum was negative for acid fast bacilli on Ziehl–Neelson stain on two occasions. On admission, his general examination revealed pulse rate was 112/min and regular, blood pressure was 134/86 mm of Hg, respiratory rate was 36/min and temperature was 100°F. Abdomen was distended, tender with rigidity and guarding. Tenderness was aggravated by movement and cough. Percussion note was tympanitic all throughout the abdomen. On examination of the respiratory system, there was vesicular breath sounds of diminished intensity with coarse crackles bilaterally over infraclavicular areas. Cardiovascular system and central nervous system examination did not reveal any significant abnormality. A diagnosis of perforated hollow viscous abdomen was made provisionally. Routine hematological investigations revealed hemoglobin 110 g/L, total leukocyte count -11.2 × 109/L, neutrophil 68% and lymphocytes 27%. Peripheral smear showed the polymorphonuclear leukocytosis without any parasite or premature cell. Liver enzymes were mildly elevated; aspartate transaminase -64 U/L, alanine transaminase-78 U/L, and alkaline phosphatase -156 U/L. Random plasma glucose was 98 mg/dL, blood urea nitrogen -12 mmol/L and creatinine -1.1 μmol/L. Sodium - 134 mEq/L and potassium -3.4 mEq/L. Serum amylase and lipase study was normal. Routine urine examination was normal. HbSAg, anti-hepatitis C virus and HIV tests were negative. Review of old chest radiograph showed infiltrations in bilateral upper zones with increased broncho vascular markings. X-ray abdomen in an erect posture showed free gas under the diaphragm. Ultrasonography of the abdomen revealed intraperitoneal gaseous distension with intraperitoneal free fluids having internal echogenicity. Patient was urgently shifted to the operation theater for exploratory laparotomy. A midline incision was given. On opening the abdomen, we found around 500 ml of purulent fluid and two small perforations 1cm apart about 20 cm proximal to the ileocaecal junction. After collecting pus sample for microbiological study thorough peritoneal lavage was done, and the perforations were sealed with omental fat. A pelvic drain was given and the incision was closed in a single layer. Postoperative period was eventful as the patient's tidal volume remained low and there was respiratory distress. The patient was shifted to intensive care unit and ventilated mechanically. Patient was treated with intravenous (I/V) piperacillin-tazobactam and amikacin. Gram staining of the pus showed Gram-negative bacilli with bipolar staining. The pus culture showed lactose fermenting pink colonies in MacConkey's agar on 2nd day which turned dry and wrinkled on day 4. The blood agar showed dry and wrinkled colonies on day 4 suspicious of B. pseudomallei [Figure 2]. The antibiotic was changed over to ceftazidime 2 g 8 h along with Amikacin. On 6th postoperative day, the organism was confirmed to be B. pseudomallei by the above-mentioned culture characteristics and standard biochemical methods (positive oxidase and nitrate reduction test, arginine dihydrolase activity, oxidation of glucose and lactose). The organism was sensitive to imipenem, doxycyclin, and cotrimoxazole. Antibiotic was switched over to imipenem 1 g 8 h along with doxycyclin 100 mg twice daily. On 9th postoperative day, we could wean off the ventilator and the patient was put on T-piece ventilation with oxygen. On 12th postoperative day, T-piece was removed, and the oxygen saturation was maintained in room air. Imipenem and doxycyclin were continued for a period of 14 days and then the patient was put on cotrimoxazole (160 + 800 mg). The patient was discharged from the hospital on 24th postoperative day with advice to continue cotrimoxazole for 4 months. On the follow-up of the patient after 6 months, the patient was doing fine, and there was no relapse.
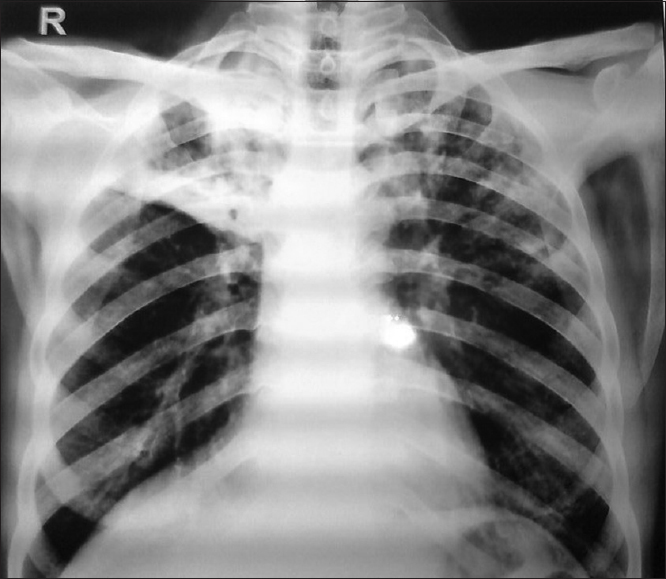
- Chest X-ray showing bilateral upper zone opacities
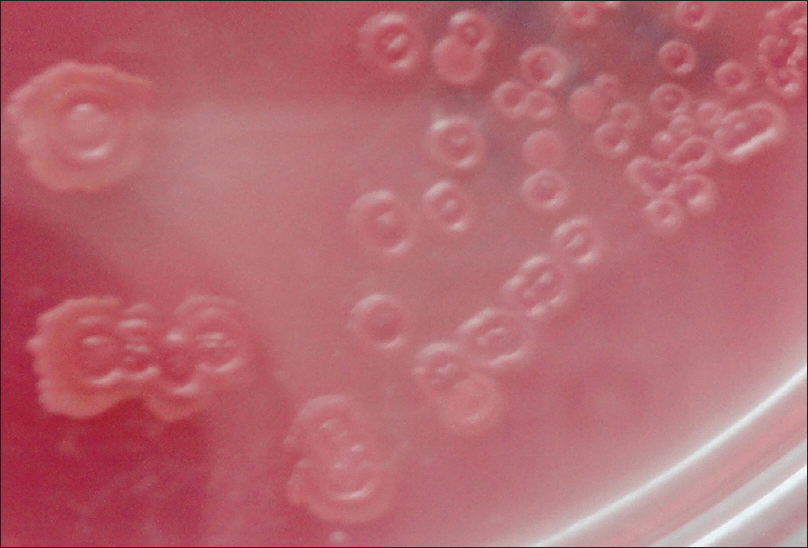
- MacConckey's agar showing dry and wrinkled colonies
DISCUSSION
Our case belonged to West Bengal in the eastern coastal belt of India, from where many cases have already been reported.[51011] Though most of the reported cases are either diabetic (76%) or immuno-compromised, our case was immuno-competent.[51012] Being a farmer, probably, he acquired the pathogen by inhalation of contaminated droplet or direct contact with contaminated soil or water through penetrating wounds and existing skin abrasions or ingestion.[9] The most common early presentation is community-acquired pneumonia.[6] However, many patients presenting with prolonged fever, weight loss, and suspicious chest X-ray findings, are misdiagnosed as tuberculosis and may get anti-tubercular therapy.[6] The other reported manifestations being multiple abscesses at varying locations like soft tissue (lower limb, scalp, psoas abscess, gluteal abscess), joint, liver, spleen, orbit and genitourinary tract.[613] But what was atypical in our case was the presentation as acute abdomen. Though many cases have been reported as liver and splenic abscess, we did not get any case presenting as acute intestinal perforation even after searching the world literature extensively.[514] Ceftazidime has been the most sensitive drug for B. pseudomallei in the literature and it has been used from two to 6 weeks in various studies.[415] Some cases of ceftazidime resistant B. pseudomallei have already been reported from India like that of ours.[4] Though the conventional intensive regimen consists of I/V ceftazidime or carbapenems with oral doxycyclin or cotrimoxazole, a recent study proves no significant difference in single versus combination therapy.[3] We successfully treated the case with combination of imipenem and doxycyclin as intensive regimen for 14 days followed by 4-month coarse of cotrimoxazole as eradication therapy.
CONCLUSION
There has been an upsurge of melioidosis cases in India.[5] Being one of the most potent emerging infections in India, the clinicians and microbiologists should be suspicious of this organism in any suppurative lesions at multiple sites.[13] Though B. pseudomallei has been most commonly reported in diabetic and immune compromised hosts, immuno-competency does not rule out its presence. All suspicious samples should be incubated for 5–7 days to isolate the organism. This case highlights the possibility of melioidosis in cases of acute abdomen and existence of ceftazidime resistant cases in India.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- An account of a glanders-like disease occurring in Rangoon. J Hyg (Lond). 1913;13:1-341.
- [Google Scholar]
- An account of the discovery of a hitherto underscribed infective disease occurring among the population of Rangoon. Indian Med Gaz. 1912;47:262-7.
- [Google Scholar]
- Orbital infection caused by Burkholderia pseudomallei: A mini review. J Infect Dis Antimicrob Agents. 2011;29:99-103.
- [Google Scholar]
- Melioidosis: An emerging infection in India. J Assoc Physicians India. 2013;61:612-4.
- [Google Scholar]
- Laboratory Diagnosis of Infectious Diseases Essentials of Diagnostic Microbiology. Philadelphia, USA: Lippincot Williams and Wilkins; 2008. p. :330.
- [Google Scholar]
- Melioidosis: Epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005;18:383-416.
- [Google Scholar]
- Isolation of Burkholderia pseudomallei from a case of septicaemia – A case report. Indian J Med Microbiol. 2003;21:129-32.
- [Google Scholar]
- Melioidosis presenting as genitourinary infection in two men with diabetes. J Postgrad Med. 2007;53:108-10.
- [Google Scholar]
- Melioidosis: An under-diagnosed entity in western coastal India: A clinico-microbiological analysis. Indian J Med Microbiol. 2007;25:245-8.
- [Google Scholar]
- Burkholderia pseudomallei infection in a patient with diabetes presenting with multiple splenic abscesses and abscess in the foot: A case report. Cases J. 2008;1:224.
- [Google Scholar]
- Multiple visceral abscess in a case of melioidosis. Indian J Med Sci. 2006;60:68-70.
- [Google Scholar]



