
Translate this page into:
Multilocular Cystic Renal Cell Carcinoma: A Rare Entity with Review of Literature
Address for correspondence: Dr. Shailja Puri Wahal, E-mail: drshailjadoe_11@ymail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Multilocular cystic renal cell carcinoma (MCRCC) represents a rare variant of clear cell renal cell carcinoma (RCC). MCRCC has been recognized as a separate subtype of RCC in the 2004 World Health Organization (WHO) classification of adult renal tumors. MCRCC is diagnosed on the basis of strict histological criteria according to 2004 WHO classification. The chief differentials diagnosis to be considered include cystic nephroma, cystic clear cell carcinoma, clear cell papillary renal cell carcinoma and tubulocystic carcinoma. Only few cases of MCRCC are reported in literature. This case is being highlighted for its rarity and so as to avoid a misdiagnosis as conventional RCC.
Keywords
Multilocular cystic renal cell carcinoma
clear cell RCC
kidney

INTRODUCTION
The 2004 World Health Organization (WHO) classification of kidney tumors recognizes multilocular cystic renal cell carcinoma (MCRCC) as a rare variant of clear cell carcinoma with a good prognosis.[1] MCRCC is also known as multilocular clear cell RCC and multicystic clear cell carcinoma.[2] These tumors comprise approximately 1-2% of all renal tumors.[3] It is important to differentiate this entity from the clear cell RCC since it is associated with good prognosis. There are other entities from which MCRCC has to be differentiated – cystic nephroma, cystic clear cell carcinoma, clear cell papillary renal cell carcinoma and tubulocystic carcinoma. We report this rare entity in 55–year–old male patient.
CASE REPORT
A 55–year–old male presented with pain in left lumbar region and hematuria since 2 months. Ultrasonography revealed a mass in the cortex of the middle part of the left kidney. Contrast enhanced computed tomography (CECT) showed a heterogeneously enhancing, well–defined–, encapsulated mass lesion in middle part of left kidney: most likely mitotic pathology. Left nephrectomy was performed. Grossly, the left nephrectomy specimen measured 13 × 6 × 3 cm and included left kidney with peri–nephric fat, ureter measuring 6 cm in length and left adrenal. Cut–surface of the left kidney showed a well circumscribed, well encapsulated growth measuring 2.5 × 2 × 2 cm situated in the cortex in the middle of the kidney [Figure 1]. Cut–surface of the growth was multiloculated, cystic with thin septae in between the cysts. The cysts were filled with brown colored gelatinous material and clots. The ureter was grossly free from any growth. Left adrenal measured 3.5 × 2 × 1 cm. Cut–surface of adrenal was within normal limits grossly. Microscopic examination of the growth revealed a complex cystic tumor comprising of variably sized non–communicating cysts separated by septae containing tumor cells showing uniform, hyperchromatic nucleus, inconspicuous nucleoli (Furhman nuclear grade 1), and abundant clear cytoplasm with distinct cell borders [Figure 2]. Mitotic figures were scarce. Lumen of the cysts contained eosinophilic secretions/hemorrhage. Septae between the cyst contain also contains cords and clusters of similar tumor cells. The ureteric resection margin, peri-nephric fat and renal vessels were free from tumor cell invasion. Adjacent renal parenchyma showed degenerative changes in the form of focal glomerular hyalinization and sclerosis, tubular casts, interstitial fibrosis, and chronic inflammatory cell infiltrate [Figure 3]. The adrenal was within normal histological limits. The histomorphology was compatible with MCRCC, Fuhrman nuclear grade 1. The patient is well without any recurrence.

- Left nephrectomy specimen showing an encapsulated growth with multiloculated, cystic growth. The cysts are filled with gelatinous material and are separated by thin septae
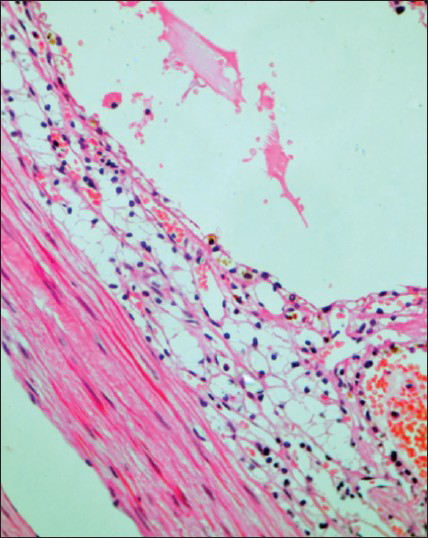
- Cyst wall lined by clear cells with uniform hyperchromatic nuclei, inconspicuous nucleoli, clear cytoplasm and well–defined cell borders (H and E, ×40)
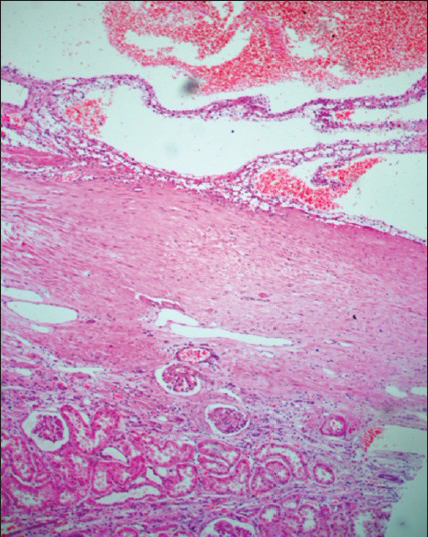
- Cysts filled with hemorrhagic material with adjacent renal parenchyma showing degenerative changes–hyalinized glomeruli, interstitial fibrosis, and chronic inflammatory cell infiltrate. (H and E, ×40)
DISCUSSION
The 2004 WHO classification recognizes MCRCC as a rare variant of clear cell RCC with a good prognosis.[1] MCRCC is also known as multilocular clear cell RCC and multicystic clear cell carcinoma.[2] These tumors comprise approximately 1-2% of all renal tumors.[3] RCC account for 80-85% of primary malignant neoplasms of the kidney.[4] It usually presents as a solid mass; however, in 10-22% of cases, RCC appears as a unilocular or multilocular cystic mass on imaging studies.[4] Four mechanisms have been described to account for RCC with cystic features: intrinsic unilocular cystic growth (papillary cystic adenocarcinoma): Intrinsic multilocular cystic growth, tumor necrosis resulting in cyst formation (pseudocyst), and tumor arising in a preexisting simple renal cyst.[4] While cysts are common in clear cell RCC, only rarely is the tumor entirely composed of cyst. The term MCRCC should be used exclusively to identify cystic RCC with a small volume (25% or less) of neoplastic clear cells in the cyst walls.[2] The male to female ratio for MCRCC is 3:1. The mean age of incidence is 51 years.[5] Diagnostic criteria for MCRCC were defined by the 2004 WHO classification of kidney tumors based on previous reports and suggestions of Ebin and Bonsib.[6] These histological criteria are presence of circumscribed, non–communicating, expansile nodule composed entirely of cysts and septa. Cysts should be lined by single layer of low grade clear cells. No papillary growth should be identified. The cysts should be separated by fibrous septae. The septae may have groups of low grade clear cells. These groups must not be expansile nodules and must not show infiltrative growth. Nuclei should be of low grade (1 or 2). The tumor should extensively sampled to make this diagnosis.[5] The presence of any expansile nodules of clear cells in the septa between the cysts indicate an ordinary, fully malignant, clear cell carcinoma with cystic change. The differential diagnosis of MCRCC consists of other cystic lesions of kidney, primarily cystic nephroma, extensively cystic clear cell RCC, clear cell papillary RCC, and tubulocystic carcinoma. While cystic nephroma may have atleast some clear cells lining the septa, the lining clear cells tend to be focally rather than diffusely distributed, and there are no clusters of clear cells in the walls. The ovarian-like stroma in cystic nephroma, if present, distinguishes it from multilocular cystic RCC by the fact that solid areas may be evident grossly, or expansile nodules of clear cells are observed microscopically. Clear cell papillary RCC is usually cystic and the cyst walls are lined by clear cells; however, much of the tumor exhibits papillary architecture, a feature not found in MCRCC.[6] Tubulocystic carcinoma differs from MCRCC in that the cystic spaces are lined by flat cuboidal and sometimes hobnail-type cells with eosinophilic cytoplasm and variable nuclear atypia, typically with nucleolar prominence in the range of Fuhrman grade 2 or 3, a feature incompatible with MCRCC. In addition the septal structures of tubulocystic carcinoma do not harbor clusters of clear cells.[7] Halat et al. conducted a study in 2010 in which they performed fluorescence in situ hybridization (FISH) analysis for 3p deletion on samples from MCRCC and compared the findings with those from a population of similarly low grade conventional clear cell RCC. Deletion of 3p was observed in 74% of MCRCC and in 89% of clear cell RCC with no statistically significant difference in the incidence of 3p deletion, between the groups.[8] Hence, proving that MCRCC is a subtype of clear cell RCC. To date, this tumor has never been shown to metastasize.[9] However, Walsh et al. in 2010 have reported the first case of MCRCC metastasizing to one out of seven intra-aortocaval lymph nodes.[10]
We report this case because of its rarity and good prognosis and to avoid a misdiagnosis as conventional clear cell RCC.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Multilocular cystic renal cell carcinoma. Pathology and Genetics of Tumors of Urinary system and male genital organs. In: Eble JN, Sauter G, Epstein JI, Sesterhenn IA, eds. World Health Organization Classification of Tumors. Lyon, France: IARC Press; 2004.
- [Google Scholar]
- Multilocular cystic renal cell carcinoma: A series of 12 cases and review of literature. Urology. 2002;60:421-7.
- [Google Scholar]
- Cystic renal cell carcinoma: Biology and clinical behavior. Urol Oncol. 2004;22:410-4.
- [Google Scholar]
- Tumors of the Kidney, Bladder, and Related Urinary Structures. AFIP Atlas of Tumor Pathology; Fourth Series, Fascicle 1. Washington, DC: American Registry of Pathology; 2004. p. :121-3.
- [Google Scholar]
- Extensively cystic renal neoplasms: Cystic nephroma, cystic partially differentiated nephroblastoma, multilocular cystic renal cell carcinoma and cystic hamartoma of renal pelvis. Semin Diagn Pathol. 1998;15:2-20.
- [Google Scholar]
- Clear cell papillary renal cell carcinoma: A distinct histopathologic and molecular genetic entity. Am J Surg Pathol. 2008;32:1239-45.
- [Google Scholar]
- Tubulocystic carcinoma of the kidney: Clinicopathologic analysis of 31 cases of a distinctive rare subtype of renal cell carcinoma. Am J Surg Pathol. 2009;33:384-92.
- [Google Scholar]
- Multilocular cystic renal cell carcinoma is a subtype of clear cell renal cell carcinoma. Mod Pathol. 2010;23:931-6.
- [Google Scholar]
- Multilocular Cystic Renal Cell Carcinoma: A Report of 45 cases of a Kidney Tumor of Low Malignant Potential. Am J Clin Pathol. 2006;125:217-22.
- [Google Scholar]
- Metastatic Multilocular Cystic Renal Cell Carcinoma – Malignant cells clearly a treatment dilemma. Br J of Urol Int 2010
- [Google Scholar]



