
Translate this page into:
Postmortem diagnosis of melioidosis: A rare case report highlighting diagnostic challenges and the role of autopsy
 , Rishabh Kumar Chandela1,, Arneet Arora1, Niranjan Sahoo1, Mrinal Patnaik2, Ayush Gupta3
, Rishabh Kumar Chandela1,, Arneet Arora1, Niranjan Sahoo1, Mrinal Patnaik2, Ayush Gupta3
*Corresponding author: Rishabh Kumar Chandela, Department of Forensic Medicine and Toxicology, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India. rishabhk.jr2022@aiimsbhopal.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Sangita M, Chandela RK, Arora A, Sahoo N, Patnaik M, Gupta A. Postmortem diagnosis of melioidosis: A rare case report highlighting diagnostic challenges and the role of autopsy. J Lab Physicians. 2024;16:570-4. doi: 10.25259/JLP_148_2024
Abstract
Melioidosis, caused by Burkholderia pseudomallei, is a severe infectious disease prevalent in tropical regions such as Southeast Asia and northern Australia, with an increasing incidence in South Asia, particularly India. The disease often goes undiagnosed due to nonspecific symptoms and limited medical awareness. This report presents the case of a 42-year-old male who died from complications following a head injury. An autopsy revealed melioidosis, with B. pseudomallei detected in blood cultures. The patient had a history of fever and loss of consciousness before his fatal incident, indicating a missed diagnosis. This case underscores the importance of considering melioidosis in differential diagnoses, especially in endemic regions, and the critical role of postmortem microbiology in identifying such infections. It highlights the need for heightened clinical awareness, improved diagnostic facilities, and comprehensive postmortem investigations to understand better and manage melioidosis. Enhanced recognition and early intervention could significantly reduce morbidity and mortality associated with this often-overlooked disease.
Keywords
Autopsy
Melioidosis
Infectious
Bacteria
Diagnosis

INTRODUCTION
Whitmore’s illness, also known as melioidosis, is an infectious disease that can affect both people and animals. Burkholderia pseudomallei is the bacteria that causes the illness. Most cases of melioidosis occur in tropical regions, particularly in Southeast Asia and northern Australia.[1] An estimated 44% of the world’s cases of melioidosis are found in South Asia. Bangladesh and Sri Lanka are thought to be endemic for melioidosis among South Asian nations. In the past years, there has been a rise in melioidosis instances in India. The bacteria are naturally found in soil and can enter the body through the skin, the respiratory system, or the digestive system.[2] Due to limited laboratory assistance and doctors’ ignorance of the condition’s appearance, the reported occurrences in India appear to be irregular and random. Melioidosis-related deaths mostly happen in the villages of low- and middle-income countries, where patients arrive at the hospital during the last severe stages of the illness.[3] Most Indians work in agriculture and reside in rural areas, where they are more likely to get infected through direct contact with soil and water. They rarely have access to reputable hospitals with diagnostic microbiological laboratories and medical professionals. Ignorance of the diagnosis and improper medication administration are other consequences of little knowledge of the clinical disease among doctors and microbiologists.[4] In India, most cases are reported from South India, with occasional reports coming from the nation’s eastern, western, and coastal regions.[4]
The symptoms of melioidosis can range from acute bacteremic forms with pneumonia, many disseminated abscesses, and septic arthritis to chronic forms with localized abscesses and osteomyelitis. Melioidosis can be localized or disseminated.[5] Because of its nonspecific symptoms, it is often treated with inappropriate antibiotics. Immunocompromised people, diabetics, and chronic alcoholics are more likely to contract the disease.[6] Although neuro-melioidosis is uncommon, it is linked to more excellent death rates.[7] The infection may stay subclinical and nonsymptomatic, making diagnosis and estimation of prevalence difficult. It is even more challenging to diagnose melioidosis in postmortem cases because of unreliable history. Furthermore, postmortem microbiology is less frequently adopted in countries like India as an ancillary investigation for routine postmortem examination. This case report emphasizes the need for increased clinical awareness, upgraded diagnostic capabilities, and thorough postmortem studies to better understand and treat melioidosis. This will also further help in assessing the prevalence of melioidosis and the antimicrobial sensitivity of the organism.
CASE REPORT
The present case is of a 42-year-old male who was healthy with no known comorbidities and had a sudden loss of consciousness and fall, because of which he succumbed to a head injury. There was a subdural hematoma and subarachnoid hematoma in the right cerebral hemisphere, and surgical intervention was done. The patient received treatment for a head injury for 10 days and died during treatment. He was unconscious throughout the treatment. Following the surgery, the antibiotics given were Intravenous: ceftazidime-avibactam (2.5 g Ter die sumendum (TDS)) and amikacin (1 g Once daily (OD)). Other medications, such as levipil and mannitol, were also received during the treatment. No fever charting was maintained, and no antipyretics were received. One month before this unfortunate episode, he had visited a coastal city in India and stayed there for around a month. During his stay there, he had a fever and an episode of loss of consciousness. However, the deceased had never undergone medical evaluation or treatment for the same.
The case presented as a case of head injury for a medicolegal autopsy. The informant and the investigating officer gave no history of fever during the hospital stay. They provided a few clinical documents that mentioned only the treatment provided, which is discussed above. An autopsy was conducted 24 h after the declaration of death, of which the body was kept in cold storage for 19 h and maintained at a temperature of 4°C. On autopsy, there were signs of surgical intervention evident, with a burr hole over the right parietal region of the calvarium [Figure 1], and the sub-scalp above it was ecchymosed. The cerebrospinal fluid (CSF) was light yellowish-tinged. Subdural and subarachnoid hemorrhages were present [Figure 2]. There was a partially healed abrasion over the dorsolateral aspect of the right forearm, corresponding to the time since the incidence. There was no other significant external injury. Both lungs were congested and edematous, and the lower lobe of the right lung was consolidated [Figure 3]. Since there was a history of prolonged hospitalization, a blood sample was collected to rule out any infection. 10 ml of blood was collected with aseptic techniques recommended by Riedel[8] and Fernández-Rodríguez et al.[9] from the heart as blood from peripheral vessels could not be procured. The collected sample was placed in BacT/Alert 3D medium bottles and then transferred for bacteriological investigation using VITEK-2 (Biomerieux, France) and Matrix assisted laser desorption ionization-time of flight (MALDI-TOF) (Biomerieux, France), and B. pseudomallei was detected. Because of unspecific autopsy findings, organ tissues were not kept for culture. Hence, B. pseudomallei was detected only in the blood culture. Histopathological examination of the brain showed parenchymal hemorrhages with no features suggestive of abscess [Figure 4]. No bacterial colony was seen on histopathological examination. The cause of death was given as head injury and its complications.
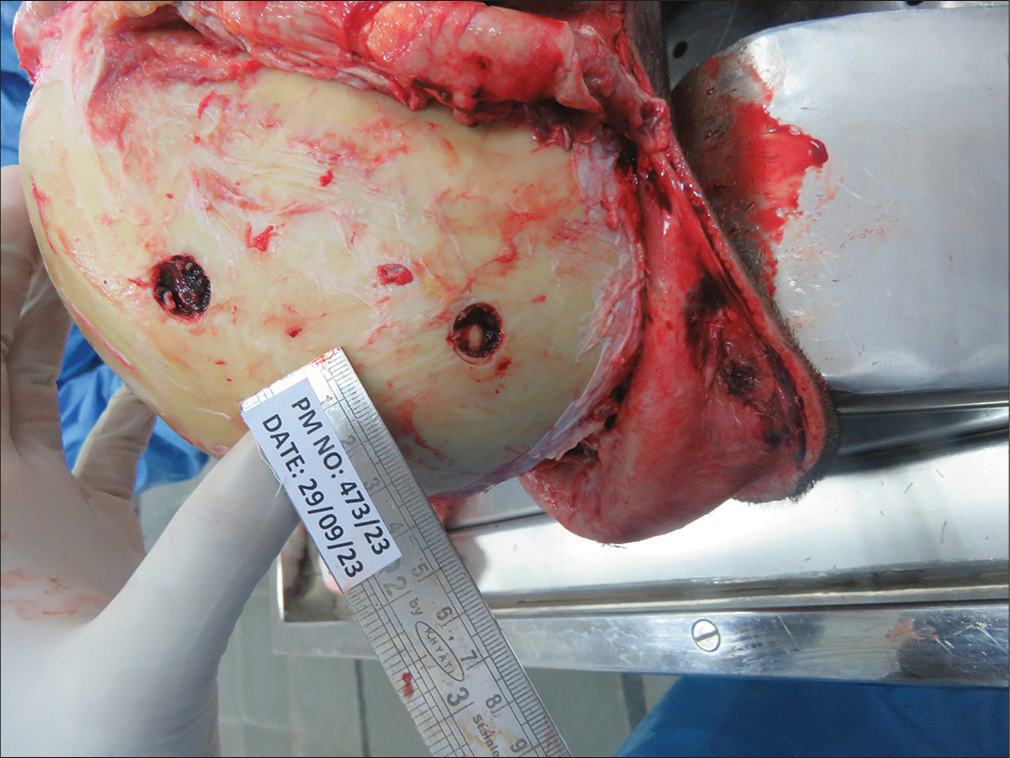
- Burr hole seen in the right parietal region from surgical intervention.
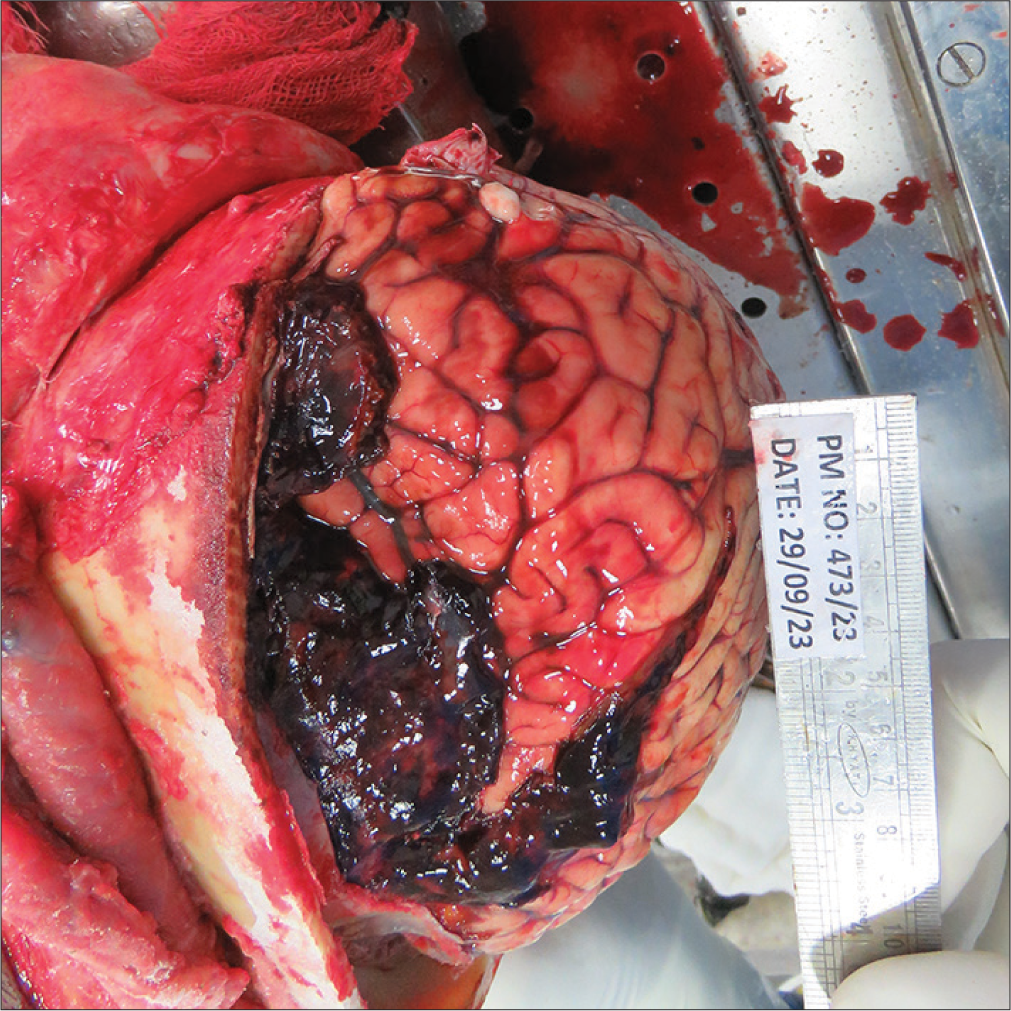
- Subdural and subarachnoid hemorrhage.
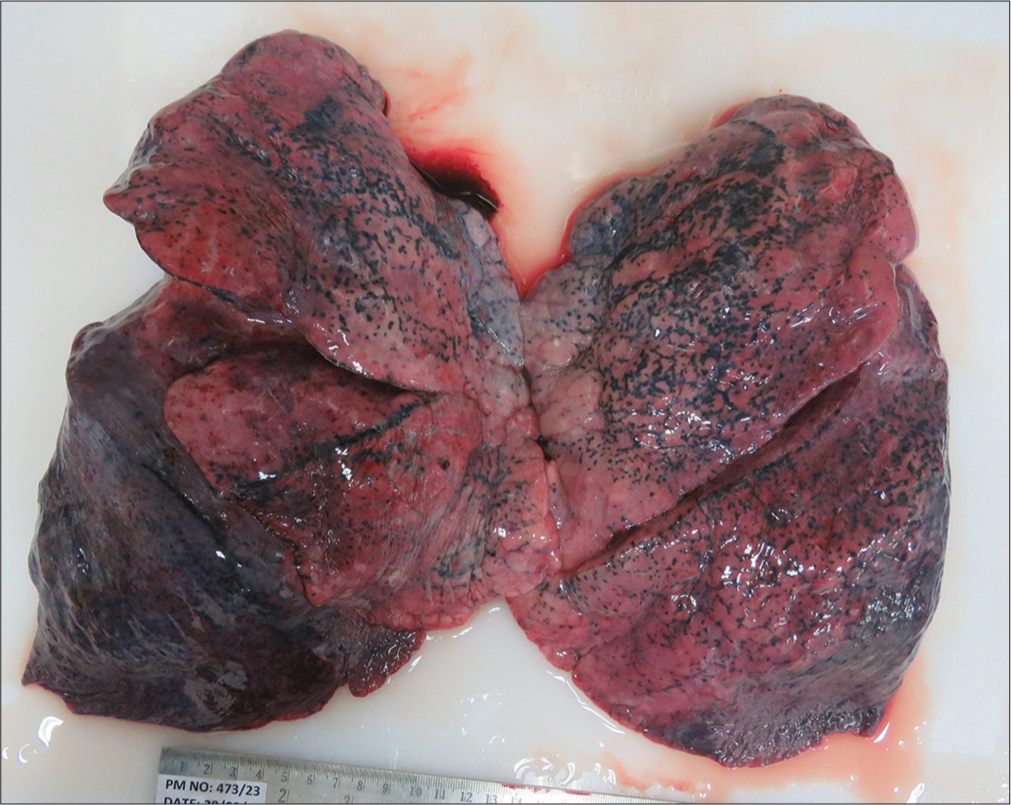
- Edematous, congested, and consolidated lungs.
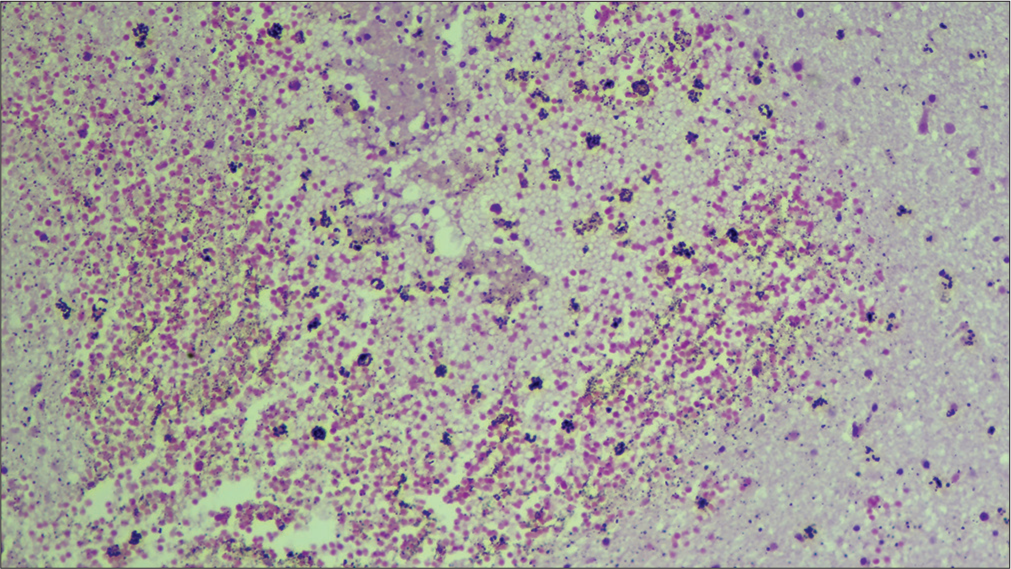
- Brain parenchymal hemorrhage (10X, Hematoxylin and eosin stain).
After a meticulous autopsy, a perusal of the postmortem ancillary investigation and the history of prolonged stay in a coastal city ignite a perspective of exposure to endemic water. The history of fever and loss of consciousness during his stay in the seaside town indicate a missed diagnosis of melioidosis, which was diagnosed as an incidental finding on postmortem microbiological investigation during a medicolegal postmortem examination.
DISCUSSION
Melioidosis, caused by B. pseudomallei, is a multifaceted infectious disease with a wide range of clinical manifestations. This case report, highlighting the postmortem diagnosis of melioidosis in a 42-year-old male, underscores the diagnostic challenges and the importance of considering this disease in differential diagnoses, particularly in endemic regions. B. pseudomallei is even considered a potential bioterror threat. The infection often spreads, leading to diverse symptoms, with septic shock being the most severe. Management is complex due to slow fever clearance, requiring extended antibiotic treatment, and resulting in high relapse rates if therapy is incomplete. Mortality rates from melioidosis septic shock remain high despite proper antimicrobial care.[10] A healthy 27-year-old man Kuwaiti who visited Kuala Lumpur had a sudden onset of fever and vomiting and died 2 days later without seeking medical attention. On autopsy, there was ventricular dilatation and consolidation of the lower lobe of the right lung. Blood and CSF showed a positive culture of B. pseudomallei.[11] This case, like the present report, underscores the rapid progression and severe outcomes associated with untreated melioidosis. Although a few cases of musculoskeletal melioidosis have been described, most of them involve soft tissues, and the condition is not widespread in India. A study conducted in India reported musculoskeletal melioidosis in five cases. Each patient had septic arthritis, recurrent osteomyelitis, or multifocal osteomyelitis at presentation. Multiorgan failure and septicemia caused the early death of one patient. Every patient received surgical debridement, and a course of antibiotics after a positive pus culture was reported.[12]
The present case involved a patient who succumbed to complications following a head injury, with an autopsy revealing B. pseudomallei in blood cultures. This finding aligns with the known pathophysiology of melioidosis, which can involve acute bacteremia. The patient’s history of fever and loss of consciousness before the fatal incident suggest a missed diagnosis of melioidosis, highlighting the nonspecific symptoms and the difficulty in clinical recognition. The autopsy findings showed bilateral congested and edematous lungs with consolidation in the lower lobe of right lung which indicated lung pathology. The typical presentation of pulmonary melioidosis is often characterized by pneumonia and lung abscesses. However, a lung abscess was not present in the current case. Histopathological examination of the brain showed parenchymal hemorrhages, further complicating the clinical picture and pointing to the potential for severe systemic involvement in melioidosis cases.
The case studied had no known comorbidities, though diabetes mellitus is the most common preexisting condition associated with an altered immune response that is frequently affected by melioidosis. Melioidosis progresses faster in cases with diabetes mellitus.[13] Melioidosis septic shock is the most severe clinical manifestation and is commonly linked to lung pathology such as pneumonia and the spread of germs to other locations.[10] Most often, especially after much rain, melioidosis appears with bacteremia or pneumonia acquired in the community. India’s status as a melioidosis-endemic country has been confirmed by the high seropositivity rate (29%) in Karnataka and the isolation of B. pseudomallei from Tamil Nadu and Kerala environments. At the same time, it is uncertain how far distributed the organism is.[4] Mumbai saw the discovery of the first native case from India in 1991.[14] In a study conducted at a tertiary hospital in South India, among patients who survived melioidosis presented with re-occurrence, it was found that 75% were reinfection and 25% as relapse.[15] Melioidosis is being treated, yet in endemic areas, recurrence of the illness has frequently been recorded, even with extended antibiotic therapy.[16] The periplasmic β-lactamases PenB and AmpC, or the membrane-bound PenA, confers acquired and innate resistance to β-lactam antibiotics, depending on the type of Burkholderia.[17] In this case, the patient was receiving ceftazidine-avibactam and amikacin. Histopathological examination of tissues from cases of melioidosis shows necrotizing and suppurative pneumonia with inflammatory cells in the lungs and intramural and subserosal necrotizing, suppurative, and granulomatous inflammation in stomach tissue.[18] However, in this case, histopathological examination of the brain showed parenchymal hemorrhages with no features suggestive of the abscess.
Furthermore, the role of autopsy in diagnosing melioidosis cannot be overstated. Postmortem microbiological investigations are crucial in identifying infections that were not diagnosed ante-mortem, thereby providing valuable insights into melioidosis’s epidemiology and clinical characteristics. Autopsies can reveal the true prevalence of melioidosis in endemic regions, which is often underestimated due to underdiagnosis and misdiagnosis during the patient’s life.
CONCLUSIONS
Melioidosis’s vague symptoms, which frequently stay subclinical or asymptomatic, make diagnosis difficult. Postmortem diagnosis is uncommon since there are usually insufficient signs and symptoms to arouse suspicions and an inadequate history available during a medicolegal autopsy. Overcoming these obstacles can be facilitated by getting a thorough medical history and being aware of the symptoms. This case study shows the importance of postmortem microbiology in detecting these illnesses. Through microbiological investigations, particularly culture techniques, melioidosis is diagnosed and confirmed by considering the case’s history and other postmortem findings. An autopsy can reveal a case of melioidosis and contribute to assessing the prevalence of melioidosis and the antimicrobial sensitivity of the organism. This emphasizes how important it is to encourage the growing role of ancillary studies in postmortem examinations.
Author contributions
MS: Manuscript and conceptualization;
RKC: Manuscript and references;
AA: Manuscript review;
NS: Conducted autopsy;
MP: Sample collection;
AG: Sample processing and result interpretation.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Available from: https://www.cdc.gov/melioidosis/index.html [Last accessed on 2024 Jul 04]
- Burden of melioidosis in India and South Asia: Challenges and ways forward. Lancet Reg Health Southeast Asia. 2022;2:100004.
- [CrossRef] [PubMed] [Google Scholar]
- A call to action: Time to recognise melioidosis as a neglected tropical disease. Lancet Infect Dis. 2022;22:e176-82.
- [CrossRef] [PubMed] [Google Scholar]
- Melioidosis in South Asia (India, Nepal, Pakistan, Bhutan and Afghanistan) Trop Med Infect Dis. 2018;3:51.
- [CrossRef] [PubMed] [Google Scholar]
- The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20-year Darwin prospective study. PLoS Negl Trop Dis. 2010;4:e900.
- [CrossRef] [PubMed] [Google Scholar]
- Neuromelioidosis: A single-center experience with emphasis on imaging. Indian J Radiol Imaging. 2021;31:57-64.
- [Google Scholar]
- The value of postmortem microbiology cultures. J Clin Microbiol. 2014;52:1028-33.
- [CrossRef] [PubMed] [Google Scholar]
- Post-mortem microbiology in sudden death: Sampling protocols proposed in different clinical settings. Clin Microbiol Infect. 2019;25:570-9.
- [CrossRef] [PubMed] [Google Scholar]
- Melioidosis: Insights into the pathogenicity of Burkholderia pseudomallei. Nat Rev Microbiol. 2006;4:272-82.
- [CrossRef] [PubMed] [Google Scholar]
- Septicemic melioidosis: A forensic autopsy case report. J Forensic Sci Med. 2018;4:229-32.
- [CrossRef] [Google Scholar]
- Burkholderia pseudomallei musculoskeletal infections (melioidosis) in India. Indian J Orthop. 2010;44:216-20.
- [CrossRef] [PubMed] [Google Scholar]
- Melioidosis: An emerging infection with fatal outcomes. Indian J Crit Care Med. 2017;21:397-400.
- [CrossRef] [PubMed] [Google Scholar]
- Melioidosis: Reinfection going incognito as relapse. Indian J Med Microbiol. 2017;35:593-6.
- [CrossRef] [PubMed] [Google Scholar]
- Melioidosis: Acute and chronic disease, relapse and reactivation. Trans R Soc Trop Med Hyg. 2000;94:3014.
- [CrossRef] [PubMed] [Google Scholar]
- Antibiotic resistance in Burkholderia species. Drug Resist Updat. 2016;28:82-90.
- [CrossRef] [PubMed] [Google Scholar]
- A graphical overview of the histopathology of human melioidosis: A case series. Open Forum Infect Dis. 2023;10:ofad367.
- [CrossRef] [PubMed] [Google Scholar]



