
Translate this page into:
Primary Nasal Tuberculosis: Resurgence or Coincidence − A Report of Four Cases with Review of Literature
Address for correspondence: Dr. Sujata Jetley, E-mail: drjetley2013@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Primary nasal tuberculosis (TB) is a rare form of TB even in areas with high TB incidence. It is timely diagnosis and proper management are often delayed due to its rarity and nonspecific clinical presentation.
Aim:
The aim of the study was to review histopathologically diagnosed cases of nasal TB over a period of 1 year and to describe its clinical presentation, diagnostic workup, the importance of histopathological diagnosis along with a brief review of the literature.
Materials and Methods:
This was a retrospective study done in the Department of Pathology of a Tertiary Care Hospital of Delhi over a period of 1 year where all the cases with histopathological diagnosis of nasal TB were reviewed. Patients' clinical details, investigations and treatment details along with follow-up were obtained from the medical records section. For each case, routine hematoxylin and eosin stain were studied along with Ziehl–Neelson staining.
Results:
A total of four patients were diagnosed with nasal TB histopathologically. Patients' age ranged from 5 to 34 with an equal male to female ratio. All patients were immunocompetent. Primary nasal TB was seen in all of the four cases. None of the cases, it was clinically suspected, and histopathology was the mainstay of diagnosis. All the cases were treated with antituberculous treatment and showed considerable improvement.
Conclusions:
Although nasal TB is rare, it should be considered in the differential diagnosis of chronic nasal symptoms and granulomatous lesions of the nose. Histopathology plays an important role in the diagnosis of these clinically unsuspecting cases of nasal TB.
Keywords
Histopathology
nasal tuberculosis
primary

INTRODUCTION
Tuberculosis of the nose is so infrequent that it has virtually become a forgotten disease entity among young clinicians. However, it still remains an important clinical entity which should be kept in mind especially in developing countries. Usually, sinonasal tuberculosis (TB) occurs secondary to pulmonary TB by inhalation of infected particles. Primary nasal TB is very rare mainly due to the protective actions of sinonasal mucosa. Only forty cases are reported worldwide until date and they may be caused by inhalation of infected particles or traumatic digital inoculation.[1]
Nasal TB was first described in 1761 by the Italian anatomy professor Giovanni Morgagni while reporting the autopsy findings of a young man with pulmonary TB, who had ulcerations of the nose, soft palate, and nasopharynx.[2] The clinicians fail to diagnose primary nasal TB as symptoms and signs of this specific nasal inflammation mimic other nonspecific nasal inflammatory conditions and therefore, its diagnosis and treatment is often delayed.[3] However, histopathology of the nasal lesions plays an important role in the timely diagnosis of sinonasal TB.
We report our experience of four cases of nasal TB, which presented over a period of 1 year along with description of the clinical case, diagnostic workup, and importance of histopathologic diagnosis for treatment planning along with a brief review of the literature.
MATERIALS AND METHODS
Retrospective review of cases of nasal TB was done in the Department of Pathology over a 1 year period. A total of 2296 cases were seen in the histopathology laboratory in 1 year out of which four cases of nasal biopsy were diagnosed with nasal TB. In all the cases, formalin fixed paraffin embedded sections were stained with both hematoxylin and eosin stain as well as Ziehl–Neelson (ZN) stain. Here, we present four cases of primary nasal TB in immunocompetent patients diagnosed histopathologically in our department over a period of 1 year.
PATIENTS AND RESULTS
Case 1
A 30-year-old female presented with complaints of epistaxis and nasal obstruction since 15 days. There was no history of contact or family history of TB or any other chronic illness. On examination, bilateral polypoidal nasal mass was seen. Her laboratory investigations revealed hemoglobin – 12.3 g%, total leukocyte count – 9800 cells/cumm, differential leukocyte count – P64 L26E08M02, platelet count – 3.12 lac, blood sugar – 93 mg%, and blood urea – 23 mg/dl. Chest X-ray was normal. Thus, a clinical diagnosis of bilateral ethmoidal polyposis with sinusitis was made. The patient received intravenous antibiotics for 3 days without any relief. Then the patient was taken up for nasal endoscopy with biopsy. Endoscopy showed bilateral edematous nasal mucosa with whitish? Granulomatous patches. Multiple punch biopsies were taken from pale granulomatous mucosa of nasal cavity and anterior ethmoids. Histopathology showed edematous mucosa showing few epithelioid granulomas and foci of necrosis [Figure 1]. ZN staining revealed few acid-fast Bacilli. Subsequent investigations for other foci of TB were negative. The patient was given antitubercular treatment. She underwent regular follow-up including nasal endoscopy and presently remains disease-free at 11 months follow-up.
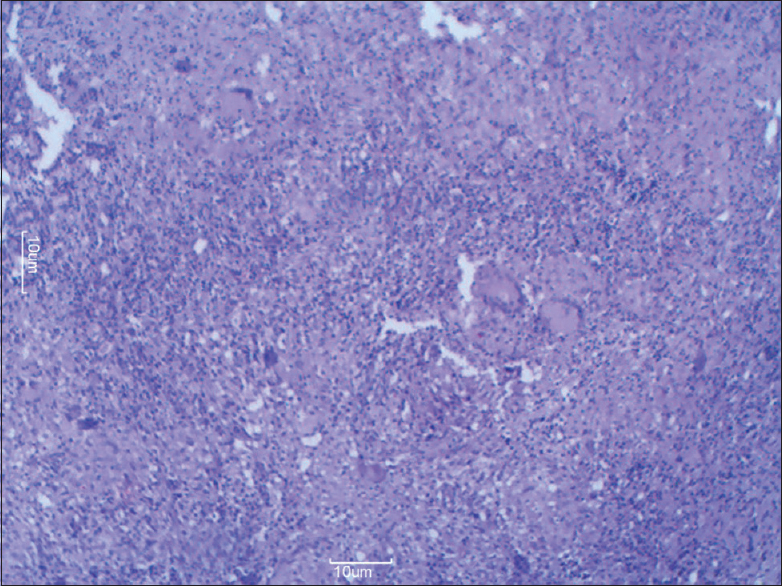
- Low power view showing edematous nasal mucosa along with granuloma (H and E, ×10)
Case 2
A 5-year-old male child presented with complaint of discharge from the right ear since 2–3 months along with right eye proptosis. The patient also complained of cervical swelling with rigidity and fever for the past 15 days. History of weight loss and low-grade fever was also present. On examination, right ear purulent discharge was seen. Right sinus tenderness and right eye proptosis was also present along with cervical lymphadenopathy.
Investigations showed hemoglobin – 9 g%, total leukocyte count – 6000 cells/cumm, polymorphs 58%, lymphocytes 36%, eosinophils – 4%, monocytes – 2%, platelet count – 4.3 lac/cumm, erythrocyte sedimentation rate (ESR) – 20, and C-reactive protein negative. Contrast enhanced computed tomography was done which revealed fungal sinusitis with mastoiditis and cervical abscess. Endoscopic nasal biopsy with neck node biopsy was done under general anesthesia. On endoscopy, right nasal cavity showed the presence of ethmoidal mucosal edema with minimal pus. Pus was sent for microbiological examination. It was positive for Gram-positive cocci but negative for acid fast Bacilli. Sputum for acid-fast bacillus (AFB) was negative, and findings on chest X-ray were normal. Histopathology of nasal biopsy showed epithelioid granulomas which were also seen in lymph node [Figure 2]. ZN stain was positive in lymph node; however, it was negative in nasal biopsy tissue. The patient was started on standard four-drug antitubercular therapy and showed considerable symptomatic improvement on follow-up.
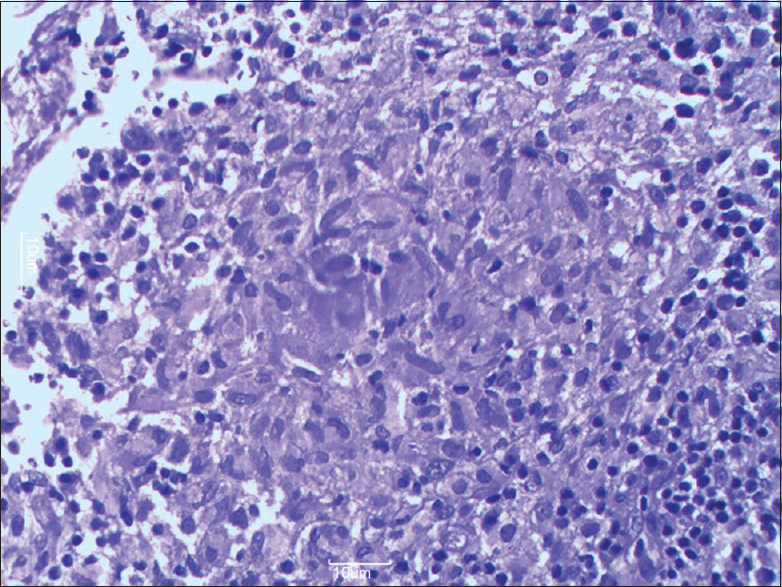
- Photomicrograph showing aggregates of epithelioid cells and peripheral lymphocytes forming well circumscribed granuloma (H and E, ×40)
Case 3
A 20-year-old male presented with nasal pain, epistaxis, and nasal obstruction since 15 days. There was no history of fever, weight loss, or any other chronic illness in the past.
Local examination revealed swelling and tenderness over dorsum of the nose. Investigations revealed normal hemogram. However, ESR was raised – 50 mm in 1st h. Mantoux test was positive. Sputum for AFB was negative, and chest X-ray was normal. Anterior rhinoscopy showed the presence of raw and friable mucosa. Computed tomography scan was suggestive of ethmoid sinusitis with edematous septum. The patient was taken up for nasal endoscopy which revealed friable and extremely tender septal mucosa. Both middle turbinates and ethmoid sinuses were also edematous. Biopsy was taken and sent for histopathological examination which showed granulomatous inflammation without necrosis. ZN stain did not reveal any acid-fast Bacilli. The patient was put on antituberculous therapy and 2 months later showed resolution of nasal symptoms.
Case 4
A 34-year-old female presented with left sided nasal obstruction and occasional epistaxis since past 6 weeks. Local examination revealed a polypoidal lesion in the left nasal cavity almost obliterating it. Investigations revealed raised ESR, i.e., 30 mm in 1st h. Her sputum smear was negative for acid-fast Bacilli, as were subsequent cultures. X-ray of the paranasal sinuses showed increased soft-tissue density and mucosal thickening in the left maxillary antrum. Nasal endoscopy revealed a sessile polypoidal mass in the left nasal cavity. The lesion was not friable or bleeding. The mucosa over the septum and the turbinate was thickened and inflamed. The lesion was biopsied and the specimen sent for histopathological examination which showed caseating epithelioid granuloma with the presence of Langhans giant cells. Tissue section was positive for acid fast Bacilli on Ziehl–Neelsen staining [Figure 3]. These findings suggested a diagnosis of TB. As no other focus of the disease was identified, a diagnosis of primary nasal TB was established. The patient was started on antituberculous treatment and few months later showed complete remission of nasal lesions.
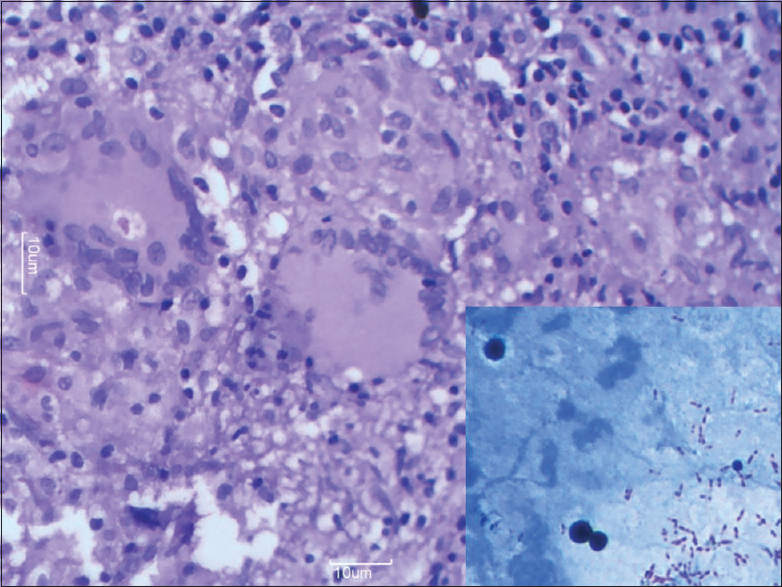
- High power view showing numerous Langhans' giant cells and dispersed epithelioid cells (H and E, ×40). Inset shows many acid fast Bacilli (ZN, ×100)
DISCUSSION
Tuberculosis of the head and neck area is rare and constitutes only 2–6% of extra-pulmonary TB and 0.1–1% of all forms of TB.[4] In the last two decades, the incidence of extrapulmonary TB is gradually increasing mainly due to human immunodeficiency virus co-infection.[5] Despite the increase in extrapulmonary TB, nasal TB is extremely rare even in countries where the incidence of TB is very high.[6] The first case of nasal TB was reported by Giovanni Morgani in 1761 while reporting the autopsy findings of a young man with pulmonary TB, who had ulcerations of the nose, soft palate, and nasopharynx.[2] The first case of primary TB of the upper respiratory tract and nose was presented to the Pathological Society of London by Clarke in 1852.[2] Later in the 18th century, reviews published by Herzog described twenty cases of primary nasal TB among eighty cases of nasal TB.[2] In a review of the 20th century medical literature published in 1997, Butt found only 35 cases of nasal TB.[5] Moon et al. examined the relative frequency of head and neck lesions in 220 patients with TB and reported that only two cases involved sinonasal cavities.[7]
We reviewed the literature of past 15 years from 2000 to 2015 and found 29 cases of primary TB [Table 1]. The largest number of cases of sinonasal TB reported by a single institution is eight, only two of which involved both the nasal cavity and the sinus and six of these patients had primary nasal TB.[8] We report four cases of nasal TB, which surprisingly presented within a span of 1 year. Sudden increase in the number of cases of nasal TB may be partly attributed to the increase in the number of extrapulmonary cases of TB and partly to a sudden increase in the number of ENT patients in our hospital due to recently upgraded infrastructure and faculty. However, it remains to be seen whether it was just coincidence or an actual resurgence of TB cases.

The TB of the nose occurs infrequently; the occurrence of primary sinonasal TB being much rarer. The reason for the scarcity of nasal TB is not clearly established. Its rarity is probably due to the self-protective functions of the nose, such as ciliary movement, bactericidal action of nasal secretion, mechanical filtering by vibrissae and inherent resistance of the nasal mucosa to mycobacterial growth.[9] The nasal mucosa is inherently very resistant to tubercle bacillus but trauma and atrophic changes usually facilitate successful lodging of Bacilli within the nasal lining as the protective mechanism of mucosa and cilia is breached.
Nasal TB occurs either secondary to pulmonary TB or lupus vulgaris of facial skin or it can be primary, that is, with no prior evidence of pulmonary TB.[10] Primary disease is rare as compared to secondary nasal TB and is caused by either inhalation of infected particles or traumatic digital inoculation. Primary nasal TB was seen in all of our four cases as there was no evidence of pulmonary TB or any focus of TB anywhere else in the body. All of these cases were seen in immunocompetent individuals. Most of the reported cases of nasal TB have occurred in patients between the ages of 20 and 84 years.[11] However, in our study one patient was a young, 5-year-old male child without any evidence of pulmonary TB. It has been reported that nasal TB occurs more often in females than males. In our case, equal incidence was noted among both the sexes.
Nasal TB remains silent and asymptomatic until advanced. The most common presenting symptom of the disease is nasal obstruction followed by nasal discharge, nasal discomfort, epistaxis, crusting, eye watering, postnasal discharge, recurrent nasal polyps, and ulceration.[5] Sometimes, septal perforation, cleft of the nasal ala, or facial abscesses may be present.[12] In our study, one of the patients had an atypical presentation in which there were no nasal symptoms, and he presented only with ear discharge and proptosis. Lesions may be ulcerative, infiltrative, or proliferative, and most cases are unilateral. The most commonly involved site is the nasal septum and can also involve the inferior turbinate.[5]
The diagnosis of primary sinonasal TB is difficult because the symptoms and signs of the various causative conditions are similar and nonspecific. In almost all our cases, nasal TB was not suspected clinically. Nasal endoscopy has an important role in diagnosis of the disease as it helps in a thorough examination of the nasal cavity and also facilitates tissue sampling from suspected areas.[13] Nasal secretions and nasal swab are not used for the diagnosis due to a low yield.[9] Smears for acid-fast bacilli and cultures tend to be negative in nasal TB.
Tissue biopsy plays an important role in the diagnosis of nasal TB. Beltran et al. proposed that the diagnosis of sinonasal TB should be based on the following criteria: The absence of a clinical response to empirical antibiotics, the presence of caseous granulomatous inflammatory lesions on histopathology, and identification of Mycobacterium TB in the surgical specimen.[14] The main diagnostic problem is that nasal TB mimics other granulomatous diseases of nose and malignancy. On histology, both caseating and noncaseating granulomas have been described. Histological examination mostly reveals caseating granuloma and Langerhans-type giant cells. Biopsies of noncaseating granulomas are often confused with other granulomatous diseases of the nose.
Differential diagnosis includes Wegner's granulomatosis, sarcoidosis, fungal infection, leprosy, rhinoscleroma, rhinosporidiosis, foreign bodies, carcinoma, natural killer-T-cell lymphoma, midline malignant reticuloma.[15] The numbers of Langhans' giant cells and epithelioid cells are believed to be greater in TB than in other granulomas.[2] If the physician fails to consider the possibility of TB, the diagnosis of nasal TB may be difficult or delayed, resulting in an unfavorable outcome.
The treatment of nasal TB usually follows the general guidelines established for the treatment of extrapulmonary TB. These guidelines usually consist of a short initial bactericidal regimen (often three or more drugs) followed by a prolonged sterilizing regimen (at least two drugs).[16] Surgery is not required when the disease is localized in nose and the standard anti- TB therapy is usually sufficient to treat the disease. Some patients of nasal TB may later develop pulmonary TB and/or extrapulmonary TB in adjacent sites such as the larynx.[9] Therefore, it is imperative that the physician looks for these concomitant manifestations during both the initial workup and subsequent follow-up of nasal TB patients.
CONCLUSION
Nasal TB though not very frequent, still remains an important clinical entity which should be kept in mind especially in developing countries. Histopathological examination is very important for the diagnosis of nasal TB and planning of therapy options. Given current trends in the incidence of TB, it would be preferable if clinicians remain aware of this infection as a potential cause of unusual lesions in the head and neck region.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Primary nasal tuberculosis – A case report. Indian J Otolaryngol Head Neck Surg. 2007;59:87-9.
- [Google Scholar]
- Extrapulmonary tuberculosis. Experience of a community hospital and review of the literature. Am J Med. 1985;79:467-78.
- [Google Scholar]
- Consensus statement. Global burden of tuberculosis: Estimated incidence, prevalence, and mortality by country. WHO global surveillance and monitoring project. JAMA. 1999;282:677-86.
- [Google Scholar]
- Tuberculosis of nose and palate with vanishing uvula. Indian J Med Microbiol. 2011;29:63-5.
- [Google Scholar]
- Tuberculosis of the maxillary sinus manifesting as a facial abscess. Ear Nose Throat J. 2002;81:102-4.
- [Google Scholar]
- A case of tuberculous sinusitis without concomitant pulmonary disease. Eur J Clin Microbiol Infect Dis. 2003;22:49-50.
- [Google Scholar]
- Tuberculosis. In: Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL, eds. Harrison's Principles of Internal Medicine (15th ed). New york: McGraw Hill; 2001. p. :1024-34.
- [Google Scholar]



