
Translate this page into:
Primary Papillary Adenocarcinoma of the Fallopian Tube with Ovarian Metastasis
Address for correspondence: Dr. Divya Sethi, E-mail: dr.divyasethi@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Primary fallopian tube carcinoma, although a common site of metastasis, comprises only 0.3% of all gynecological malignancies.[1] We report a case of primary fallopian tube carcinoma in a 50-year old female. Presenting its symptoms are variable and nonspecific, with preoperative diagnosis rarely entertained. It is more common for cancer to spread or metastasize, from other part of the body, such as ovaries or endometrium than for cancers to actually originate in the fallopian tube.
A 50-year old multiparous patient, married since 28 years, menopausal since 5 years, approached clinicians with the complaints of the ill-defined tender mass since last 1 year and intermittent bleeding per vaginum since last 15 days. On examination, patient was obese and her vital parameters were stable. Systemic examination was normal. Per abdominal examination revealed a firm and nontender mass arising from the pelvis on the left side. Per-vaginum examination revealed uterus to be atrophic and mobile. On the left side, solid, firm, and mobile forniceal mass was felt. Patient was admitted and investigated. All routine investigations including the liver and renal function test were within normal limits. Cytology detected inflammatory smear. Ultrasonography showed a pelvic mass of size 5 cm × 4.4 cm, of possibly ovarian origin arising from the left side. Contrast-enhanced computed tomography scan of pelvis showed a soft tissue mass in left adnexa of 4.8 cm × 4.2 cm [Figure 1]. Tumor marker CA 125 was raised (600 mL/L). Hence, presumptive diagnosis of carcinoma of ovary was made. Total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed. Grossly, endometrium, cervix, right-sided fallopian tube, and ovary were unremarkable. Left-sided ovary measured 3 cm × 2 cm × 1 cm and cut surface was solid. The left-sided fallopian tube was dilated and measured 7 cm × 3 cm. The cut surface revealed solid gray white areas measuring 3 cm × 2 cm × 1 cm with papillae formation. Histologically, the endometrium, cervix, right ovary, and fallopian tube were unremarkable. The left-sided fallopian tube showed a malignant tumour composed of cells arranged in the papillary and glandular pattern. The cells lining the papillae showed stratification, pleomorphism, and nuclear atypia. The tumor cells were seen infiltrating the underlying submucosa and muscularis propria but did not penetrate the serosal surface of the fallopian tube. Sections from the left ovary revealed nests of adenocarcinoma in an otherwise unremarkable ovarian stroma. The patient was diagnosed to be a case of primary carcinoma of the fallopian tube (stage IIa) [Figures 2 and 3].
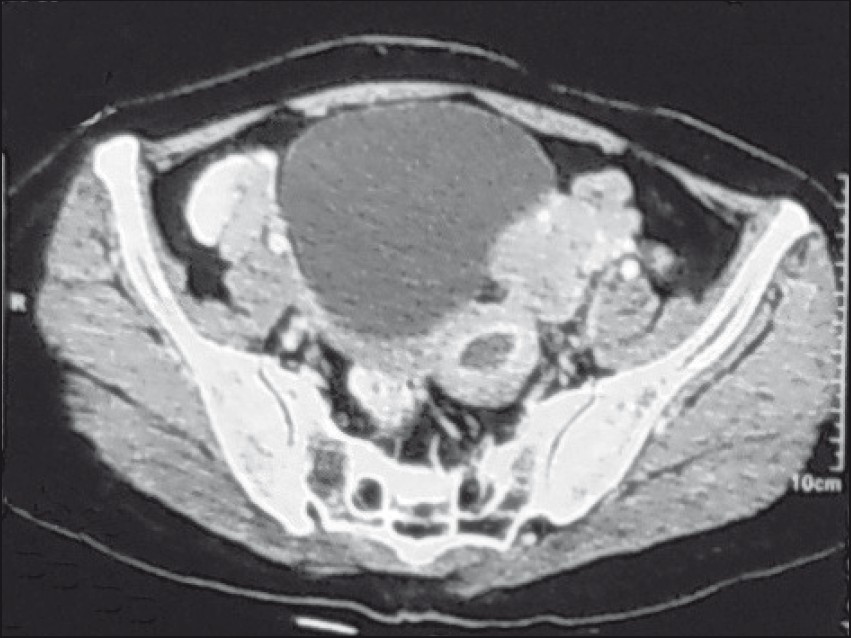
- CECT revealing soft tissue mass in left adnexa of size 4.8 cm × 4.2 cm.
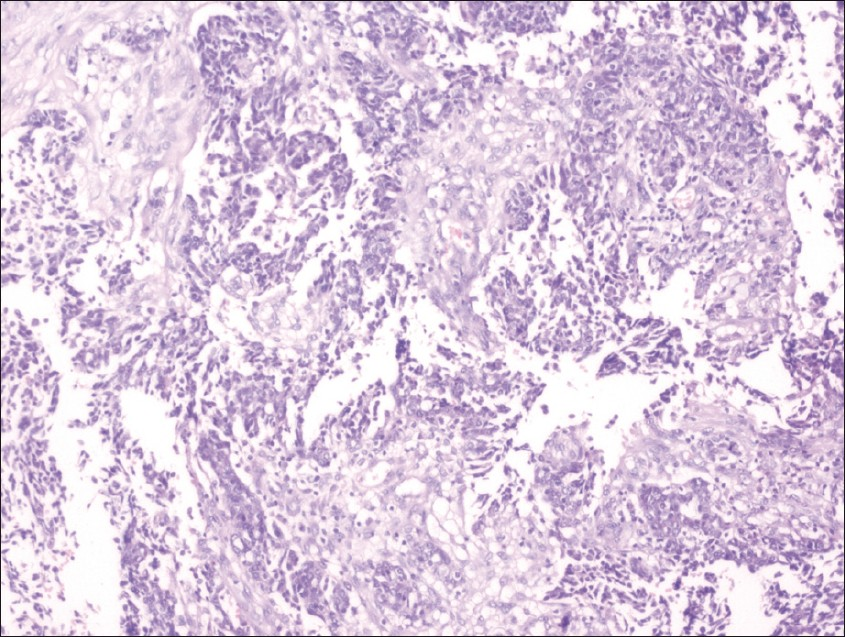
- Microsection shows predominantly papillary pattern of adenocarcinoma with glandular formation at places (H and E, ×100).
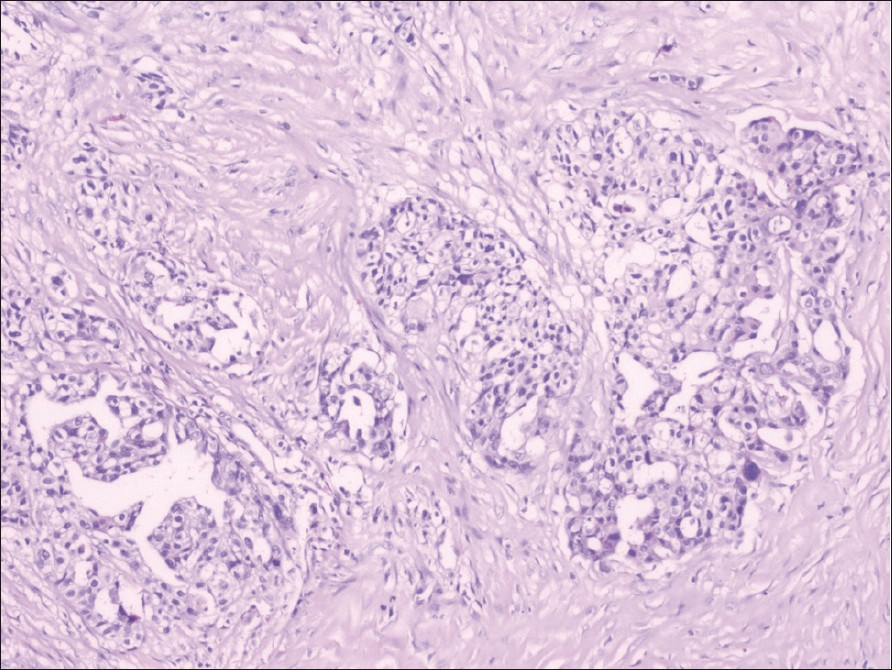
- Microsection shows nests of adenocarcinoma in an otherwise unremarkable ovarian stroma (H and E, ×100).
Approximately 80% of malignancies of the fallopian tube are from other sites, most commonly from ovary, endometrium, and gastro-intestinal tract. Frequency of primary adenocarcinoma of fallopian tube 0.3–0.5% according to various series and its aetiology remains unknown.[2] Fallopian tube carcinoma is known to be insidious and asymptomatic for prolonged and variable periods of time. Most commonly presenting symptoms are perimenopausal and postmenopausal bleeding per vagina followed by amber-coloured vaginal discharge and abdominal pain.[2] But all these features are present in 6% of cases.[3] Tubal carcinoma usually originates in the ampulla and its pattern of growth can be nodular, papillary, and infiltrative.[1] These tumors are relatively confined to the tube and may not have any alteration in size and shape of the fallopian tube, or it may feature diffuse swelling, a sausage-shape resembling hydro, hemato, and pyosalpinx. Histo-pathological examination reveals a papillary adenocarcinoma extending into submucosa and muscularis layer, as was seen in our case.[2] Preoperative diagnosis of the fallopian tube carcinoma is seldom made prior to surgery. It is suspected in fewer than 5% of cases preoperatively. Primary ovarian neoplasm is the most common preoperative diagnosis made in these patients. Since it is difficult to differentiate the primary fallopian tube carcinoma from epithelial ovarian cancer, Hu et al established diagnostic criteria for their differentiation in 1950, which were modified in 1978. Patients with at least one of the following criteria should have the diagnosis of primary fallopian tube carcinoma.[4–6]
-
The tumour arises from the endosalpinx.
-
The histological pattern reproduces the epithelium of tubal mucosa.
-
Transition from benign to malignant epithelium is found.
-
The ovaries and endometrium are either normal or contain less tumor than the tube.
The tumor spread occurs by means of contiguous invasion, transluminal migration, and hematogenous dissemination.[6] Transluminal migration may be the cause in our case. Primary adenocarcinoma of fallopian tube with papillary features is the most common histological type forming more than 90% of malignant tumour. The most important prognostic factor in the fallopian tube carcinoma is stage of disease at laparotomy. Tumor marker such as CA 125 is proving to be of help in the diagnosis of fallopian tube carcinoma. Levels of CA 125 rise with the advanced stage of disease.[2]
In conclusion, fallopian tube carcinoma is a rare type of genital cancer, which is difficult to diagnose early and carries a poor prognosis.
REFERENCES
- Primary fallopian tube adenocarcinoma with brain and lung metastasis. Indian J Pathol Microbiol. 2009;52:596-8.
- [Google Scholar]
- Bilateral primary fallopian tube carcinoma: findings on sequential MRI. AJR Am J Roentgenol. 2006;186:1046-50.
- [Google Scholar]
- Primary carcinoma of the fallopian tube. Am J Obstet Gynecol. 1950;59:58-67. illust
- [Google Scholar]



