
Translate this page into:
Renal Dysfunction in Prediabetes: Confirmed by Glomerular Hyperfiltration and Albuminuria
Address for correspondence: Alagilawada S. Shilpasree, MD, Department of Biochemistry, SDM College of Medical Sciences and Hospital, Shri Dharmasthala Manjunatheshwara University, Sattur, Dharwad 580009, Karnataka, India (e-mail: shilpasree2007@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Objectives
Prediabetes is defined as an intermediate state of hyperglycemia with glucose levels above normal but below the diagnostic cutoff of diabetes mellitus. Prediabetes is considered as an important risk factor for the development of diabetes and complications associated with diabetes. Since glomerular hyperfiltration (elevated GFR) and albuminuria represent early and reversible stages of kidney damage seen in patients with type 2 diabetes, we aim to assess the impact of hyperglycemia in prediabetic range on renal functions measured by estimated GFR and urine albumin excretion (UAE).
Materials and Methods
The study included 1,031 patients aged 30 to 70 years, attending regular health checkup. Patients were grouped as normal, prediabetes, and diabetes according to the American Diabetic Association (ADA) criteria based on fasting blood sugar and hemoglobin A1c (HbA1c). Further, the patients were grouped into multiple subgroups based on age and gender. UAE was measured by using immunoturbidimetric method, and GFR was estimated by chronic kidney disease epidemiology collaboration (CKD EPI) equation.
Statistical Analysis
Prevalence of hyperfiltration (estimated glomerular filtration rate above the age and gender specific 95th percentile), and albuminuria in prediabetes and diabetes was compared with normal controls. Odds ratio and 95% confidence interval were calculated by using logistic regression analysis to predict the occurrence of hyperfiltration in prediabetes and diabetes. Analysis of variance followed by post hoc comparison was done to assess the significance of difference, and p-value < 0.05 was considered statistically significant.
Results
Prevalence of hyperfiltration was more in prediabetes and diabetes compared with normal controls, and it increased with surging HbA1c level that was shown as higher odds ratio for hyperfiltration in both the groups. UAE was more in the prediabetes and diabetes group when compared with normal controls, but the difference was significant only in diabetes.
Conclusion
Since glomerular hyperfiltration represents an early and reversible stage of renal damage manifesting before the appearance of albuminuria, elevated GFR can be used to identify asymptomatic patients with intermediate hyperglycemia having high risk of developing nephropathy in the future. Prediabetes represents a window of opportunity to initiate preventive strategies at an early stage before the occurrence of significant renal damage.
Keywords
prediabetes
glomerular hyperfiltration
estimated GFR
urine albumin excretion

Introduction
Prediabetes is defined as an intermediate state of hyperglycemia with glucose levels above normal but below the diagnostic cutoff of diabetes mellitus. Prevalence of prediabetes is much higher compared with diabetes.[1] According to the National Health and Nutrition Examination Survey, the crude prevalence of diabetes, detected by fasting blood glucose (FBG) or 2-hour post glucose load plasma glucose, is 12.9% and the prevalence of prediabetes is 29.5% among people aged > 20 years.[2] Prediabetes is diagnosed based on impaired fasting glucose (FBG levels between 100 and 125 mg/dL) and/or impaired glucose tolerance (2-hour post glucose load blood glucose levels during 75 g oral glucose tolerance test between 140 and 199 mg/dL) and/or hemoglobin A1c (HbA1c) between 5.7 and 6.4%.[3] About 25% of patients with prediabetes will progress to type 2 diabetes mellitus (T2DM) within 3 to 5 years, and as many as 70% of individuals with prediabetes will develop overt diabetes in their lifetime. Patients with prediabetes also have an increased risk of developing microvascular and macrovascular complications associated with diabetes.[4]
Chronic kidney disease (CKD) is diagnosed based on the presence of renal damage manifesting as albuminuria (urine albumin creatinine ratio > 30 mg/g) and/or reduced renal function (glomerular filtration rate < 60 mL/min/1.73m2) for 3 months or more.[5] Glomerular hyperfiltration (elevated GFR) is a well-recognized, early, and reversible stage of kidney damage seen in patients with type 2 diabetes, and it is an independent risk factor for accelerated renal function loss and progression to CKD.[6,7] Hyperfiltration in diabetes precedes the onset of albuminuria and decline in GFR.[8]
Up to 30% of individuals with recently diagnosed diabetes mellitus present some degree of renal disease, which suggest that the effects of hyperglycemia on kidney might begin very early before the glucose levels reach diabetic range. However, the long-term influences of prediabetes on kidney functions are still unknown.[9] Various studies addressing the association of glycemic status in prediabetes with hyperfiltration and albuminuria have shown inconsistent results due to reasons such as limited population; different ethnicities; and lack of availability of age, sex, and race specific reference ranges for eGFR. With above rationale, we aim to assess the impact of hyperglycemia in prediabetic range on renal functions measured by estimated GFR (eGFR) and UAE.
Materials and Methods
A cross-sectional study was performed in patients coming for routine health checkup. After obtaining the ethical clearance from the institutional ethical committee, a total number of 1,085 patients in the age group of 30 to 70 years were enrolled for the study. Patients with history of CKD, hepatic diseases, cardiovascular diseases, and proteinuria (> 300 mg/L) were excluded from the study.
After obtaining the informed consent, approximately 5 mL of blood was drawn under aseptic precautions after overnight fasting of 12 hours, and serum separated by centrifugation was used for the estimation of FBG, urea, creatinine, and lipid profile. FBG was estimated by hexokinase method and lipid profile by enzymatic methods. Total cholesterol (TC) was estimated by cholesterol oxidase-peroxidase method, LDL-cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) by direct methods, and triglycerides (TGs) by glycerol phosphate oxidase-peroxidase method. Blood urea was measured by enzymatic urease method and serum creatinine by modified Jaffe's kinetic method traceable to international reference method (IDMS). A spot urine sample was collected in a separate urine container and used for the estimation of UAE by immunoturbidimetric method. All estimations were performed on fully automated Siemens dimension ExL instrument. About 2 mL of blood was collected in a heparinized syringe used for the estimation of HbA1c (method traceable to NGSP) on fully automated Bio-Rad D10 analyzer.
Patients were grouped into three groups: normal, prediabetes, and diabetes—based on FBG and HbA1c values. Diagnosis of prediabetes and diabetes was done based on ADA criteria:[3]
Prediabetes: Patients with FBG 100 to 125 mg/dL and/or HbA1c of 5.7–6.4%
Diabetes: Patients with FBG ≥ 126 mg/dL and HbA1c ≥ 6.5%
Normal controls: Individuals with FBG < 100 mg/dL and HbA1c < 5.7%
Normal controls were grouped into eight subgroups based on age and gender:
Group 1a: 30–39 years (male) Group 1b: 30–39 years (female)
Group 2a: 40–49 years (male) Group 2b: 40–49 years (female)
Group 3a: 50–59 years (male) Group 3b: 50–59 years (female)
Group 4a: 60–69 years (male) Group 4b: 60–69 years (female)
GFR was estimated by chronic kidney disease epidemiology collaboration (CKD EPI) equation[10] using serum creatinine, age, and gender as variables. Hyperfiltration was defined as eGFR > 95th percentile of age and gender specific eGFR in normal controls, and hypofiltration was defined as eGFR < 5th percentile of age and gender specific eGFR in normal controls. Prevalence of hyperfiltration in prediabetes and diabetes patients was compared with normal controls. Odds ratio and 95% confidence interval for hyperfiltration were calculated in prediabetes and diabetes patients using logistic regression analysis. Age, gender, FBG, HbA1c, and lipid profile were taken as independent variables to predict the occurrence of hyperfiltration. UAE in prediabetes and diabetes was compared with normal controls. ANOVA followed by post hoc comparison was done to assess the significance of difference and p-value < 0.05 was considered statistically significant.
Results
A total of 1,031 patients were included in the study after excluding 54 patients as per the above-mentioned exclusion criteria. Patients were divided into normal, prediabetes, and diabetes group according to the ADA criteria. Baseline characteristics of study participants are given in ►Table 1. The distribution of eGFR and the reference values for hyperfiltration and hypofiltration in normal controls for each 10-year age group are shown in ►Fig. 1.
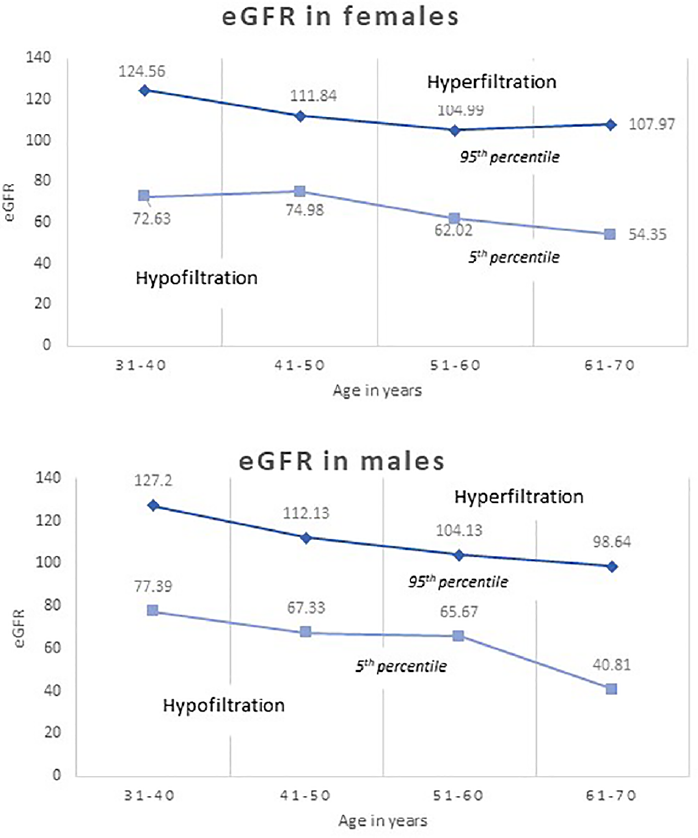
- Distribution of estimated glomerular filtration rate in normal controls by age and sex. The 95th and 5th percentile are shown in 10-year age groups.
| Normal | Prediabetes | Diabetes | |
|---|---|---|---|
| Number | 274 | 268 | 489 |
| Males | 141 (51.46%) | 165 (61.57%) | 306 (62.58%) |
| Females | 133 (48.54%) | 103 (38.43%) | 183 (37.42%) |
| Age in years | 51.1 (12.9) | 56 (12.5) | 54.9 (12) |
| FBS in mg/dL | 88.6 (9.3) | 111.3 (7.4) | 189.7 (61.7) |
| HbA1c in % | 5.3 (1.1) | 6.1 (1.3) | 8.3 (2.1) |
| Creatinine in mg/dL | 0.85 (0.22) | 1.01 (2.9) | 0.98 (0.4) |
| eGFR in mL/min/1.73 m2 | 92.4 (18.1) | 91.1 (25.8) | 84.2 (25.5) |
| UAE in mg/L | 20.7 (10.1) | 32.1 (24.2) | 60.9 (29.6) |
| Total cholesterol in mg/dL | 177 (44.9) | 165.16 (42) | 171.9 (46.2) |
| LDL cholesterol in mg/dL | 104.2 (36.6) | 101.5 (34.5) | 105.8 (39.9) |
| HDL cholesterol in mg/dL | 41.8 (10.9) | 41.1 (10.3) | 37.3 (10.9) |
| Triglycerides in mg/dL | 122.6 (68.2) | 132 (76) | 182.2 (146.4) |
| No. of people with glomerular hyperfiltration | 10 (3.6%) | 21 (7.8%) | 43 (8.7%) |
Abbreviations: eGFR, estimated glomerular filtration rate; FBS, fasting blood sugar, HbA1c, hemoglobin A1c; HDL, high density lipoprotein; LDL, low density lipoprotein; UAE, urine albumin excretion.
Note: Data expressed as mean (standard deviation) or number (%).
Kruskal–Wallis test was used to compare the prevalence of hyperfiltration among three groups followed by post hoc comparison of prevalence of hyperfiltration between the groups (►Tables 2 and 3). There was a significant difference in the prevalence of hyperfiltration among three groups. The prevalence of hyperfiltration was higher in the prediabetic and diabetic groups compared with the controls, and the difference was statistically significant (p < 0.05).
| Group | Mean rank | H statistic | p-Value |
|---|---|---|---|
| Normal | 495.12 | 6.82 | 0.03a |
| Prediabetes | 516.16 | ||
| Diabetes | 521.07 |
aSignificant at p < 0.05.
| Groups compared | Mean ranks | Z score | p-Value |
|---|---|---|---|
| Normal vs. prediabetes | 263 | −2.03 | 0.04a |
| 274 | |||
| Normal vs. diabetes | 366.62 | −2.60 | 0.009a |
| 385.78 | |||
| Prediabetes vs. diabetes | 376.66 | −0.45 | 0.65 |
| 380.28 |
aSignificant at p < 0.05.
Logistic regression was conducted to predict the presence of hyperfiltration. Age, gender, HbA1c, and the group were the significant predictors of hyperfiltration (►Table 4). The odds of having hyperfiltration was significantly greater in younger patients, females, and those with greater HbA1c. The prediabetic and diabetic patients were at significantly greater odds of having hyperfiltration (2.83 and 2.74, respectively) than the controls.
| Predictors | Odds ratio | Confidence intervals | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.949 | 0.928 | 0.971 | 0.000b |
| Males | 0.577 | 0.340 | 0.981 | 0.042a |
| FBG | 0.994 | 0.988 | 1.001 | 0.099 |
| HbA1c | 1.275 | 1.096 | 1.483 | 0.002a |
| Total cholesterol | 1.026 | 0.992 | 1.062 | 0.140 |
| HDL C | 0.968 | 0.925 | 1.012 | 0.147 |
| LDL C | 0.976 | 0.941 | 1.013 | 0.201 |
| TG | 0.995 | 0.989 | 1.000 | 0.064 |
| Ref: control group | 1 | 0.040a | ||
| Prediabetes group | 2.832 | 1.242 | 6.458 | 0.013a |
| Diabetes group | 2.745 | 1.057 | 7.127 | 0.038a |
| Constant | 0.255 | 0.205 | ||
Abbreviations: FBG, fasting blood glucose; HbA1c, hemoglobin A1c; HDL, high density lipoprotein; LDL, low density lipoprotein; TG, triglycerides.
aSignificant at p < 0.05.
bSignificant at p < 0.001.
UAE was compared between all the three groups by using ANOVA (►Table 5) followed by post hoc comparison between individual groups (►Table 6). There was a significant difference in UAE among three groups. However, in prediabetic group, it did not differ significantly from normal controls where as in diabetic group, it was significantly higher compared with normal controls and prediabetic group.
| Group | Mean amount of albumin | F statistic | p-Value |
|---|---|---|---|
| Normal | 20.66 | 18.79 | 0.000a |
| Prediabetes | 32.07 | ||
| Diabetes | 60.90 |
aSignificant at p < 0.001.
| Groups compared | Mean difference | p-Value |
|---|---|---|
| Normal vs. prediabetes | −11.40 | 0.32 |
| Normal vs. diabetes | −40.23 | 0.000a |
| Prediabetes vs. diabetes | −28.82 | 0.000a |
aSignificant at p < 0.001.
Discussion
Till recent times, appearance of small amounts of albumin in urine (30–300 mg/day), referred as microalbuminuria was considered as an earliest marker of diabetic nephropathy. However, albuminuria is nonspecific to diabetes and can be seen in many other conditions such as exercise, urinary tract infections, hypertension, and cardiac failure. It has been reported that in diabetic patients, a large proportion of renal function impairment occurs even before the appearance of microalbuminuria.[11] Due to these limitations, additional biomarkers that predict diabetic nephropathy at a very early stage, even before the appearance of microalbuminuria are needed for optimal clinical management of diabetic patients.
Glomerular hyperfiltration manifests at early stages of type 2 diabetes characterized by normoalbuminuria or microalbuminuria followed by progressive decline in GFR resulting in diabetic nephropathy, which may occur with or without worsening of albuminuria.[12] Studies have shown that glomerular hyperfiltration precedes the onset of albuminuria and decline in GFR.[13] Hence, elevated GFR can be seen in subset of diabetic patients without albuminuria. Although National Kidney Foundation and Kidney Disease Improving Global Outcomes guidelines recommend only decline in GFR and albuminuria as diagnostic markers of CKD,[14] glomerular hyperfiltration can be considered as the first and foremost manifestation of diabetic nephropathy.
Prediabetes represents an intermittent stage of hyperglycemia. About 25% of patients with prediabetes will progress to type 2 diabetes within 3 to 5 years, and as many as 70% of individuals with prediabetes will develop overt diabetes in their lifetime.[4] Although patients with prediabetes have increased risk of developing complications of diabetes, prediabetes is considered as a distinct pathological entity.[15] Various cross-sectional studies have shown the association between prediabetes and CKD.[16] The prevalence of CKD in prediabetes was as much as 70% higher compared with those with normal glycemic control,[17] but whether prediabetes predicts the onset of CKD in patients who do not develop diabetes is not clear.
Our study demonstrated the presence of glomerular hyperfiltration in prediabetes and diabetes patients. As there is no consensus on the definition of hyperfiltration and GFR varies with age, sex and race, eGFR above the age and gender specific 95th percentile was used to define hyperfiltration. Degree of hyperfiltration increased with worsening of glycemic control in both the groups. Increasing HbA1c was associated with significantly increased odds ratio of hyperfiltration on logistic regression analysis, but the same relationship was not observed for FBG indicating the effect of long-term glycemic control on glomerular filtration. However, significant amount of albuminuria was seen only in diabetic patients.
Our findings are consistent with various other studies which have demonstrated the presence of hyperfiltration in prediabetes and diabetes patients.[18,19] In a large Japanese cohort, the prevalence of hyperfiltration was high in prediabetes individuals and increased with worsening of glycemic control (increasing FBG and HbA1c).[9] In middle aged and elderly Chinese population, HbA1c was positively associated with hyperfiltration in prediabetes and newly diagnosed diabetes patients.[20] This association is assumed to be related to metabolic control, as reduction of blood glucose returns GFR to near normal levels.[15] Even obesity was associated with hyperfiltration. However, hyperinsulinemia and insulin resistance are the proposed mediators of hyperfiltration and subsequent renal injury in obesity.[21] As hyperinsulinemia and insulin resistance are noticed in early stages of diabetes including prediabetes,[22] they may contribute to the development of hyperfiltration. If hyperfiltration in prediabetes is considered as maladaptive response due to metabolic derangement as seen in diabetes, the process of kidney damage likely to start very early in the course of hyperglycemia.[13] Although the exact pathophysiologic mechanism is largely unknown, hyperfiltration is attributed to hemodynamic changes occurring at single nephron level including altered renal plasma flow, transmembrane hydraulic pressure gradient, and the ultrafiltration coefficient leading to intraglomerular hypertension. Together with vascular inflammation, it may cause elevated GFR and microalbuminuria.[8,23] Long-term hyperfiltration combined with hyperglycemia can induce podocyte stress, podocyte injury and cell apoptosis[13] and predisposes to renal damage as a result of progressive glomerular sclerosis.[18] Studies have demonstrated accelerated long-term GFR decline and progression to micro- or macroalbuminuria in patients with persistent hyperfiltration as compared with normofiltration despite of similar treatment strategies. In a meta-analysis including type 2 diabetic patients, glomerular hyperfiltration was associated with greater rate of GFR decline in addition to normal physiological age-related decline and increased risk of developing diabetic nephropathy.[15] This supports the possible role of hyperfiltration on pathogenesis of diabetic nephropathy.[7]
Our study also demonstrated the presence of albuminuria in prediabetic and diabetic individuals. However, significant amount of albuminuria was noticed in only diabetic patients but not in prediabetes. Studies have shown an increase in FBG or HbA1c in normal nondiabetic range are associated with progression of UAE.[23] The findings from the Diabetes Prevention Program Trial highlight the fact that albuminuria is multifactorial. Higher BMI is associated with albuminuria in diabetes and prediabetes patients and weight reduction can reduce the UAE.[17] Other components of metabolic syndrome such as hypertension and dyslipidemia are also associated with microalbuminuria.[24] Due to the lack of specificity and the fact that significant amount of renal function impairment occurs before the onset of microalbuminuria, elevated GFR can be used in early stages of diabetes and prediabetes to predict the risk of future nephropathy.
Although prediabetes is considered as a condition but not a disease, early intervention can yield positive outcomes. Therefore, it is essential to focus on the prevention of chronic conditions including prediabetes and diabetes that have an impact on the risk of CKD. Prediabetes may however be reversible through the implementation of lifestyle modification programs based on the adoption of healthier diet and increased levels of physical activity. Where lifestyle modifications are ineffective, medications are indicated. Early detection and effective intervention can be initiated in these patients having glomerular hyperfiltration before the occurrence of diabetes to prevent the pathophysiologic changes leading to irreversible renal damage.
Conclusion
Since glomerular hyperfiltration represents an early and reversible stage of renal damage manifesting before the appearance of albuminuria, elevated GFR can be used to identify asymptomatic patients with intermediate hyperglycemia having high risk of developing nephropathy in the future. Our study emphasizes the need to monitor the renal functions in prediabetic patients. Prediabetes represents a window of opportunity to initiate preventive strategies at an early stage before the occurrence of significant renal damage.
Note
Ethical clearance was taken by Institutional Ethical Committee (IEC/828/10/2019).
Authors’ Contributions
A.S.S. and V.S.P. participated in conception and design, acquisition of data, and analysis and interpretation of data. A.S.S., M.R., V.P.P., and D.I. assisted in drafting the article and revising it critically for important intellectual content. A.S.S., V.S.P., and M.R. provided the final approval of the version to be published.
Conflict of Interest
None declared.
Funding
None.
References
- et al The prevalence of pre-diabetes and diabetes and their associated factors in Northeast China: a cross-sectional study. Sci Rep. 2019;9(01):2513.
- [CrossRef] [PubMed] [Google Scholar]
- Full accounting of diabetes and pre-diabetes in the U.S. population in 1988-1994 and 2005-2006. Diabetes Care. 2009;32(02):287-294.
- [CrossRef] [PubMed] [Google Scholar]
- Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(01)(Suppl 1):S13-S28.
- [CrossRef] [PubMed] [Google Scholar]
- Global epidemiology of prediabetes - present and future perspectives. Clin Diabetes Endocrinol. 2019;5:5.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic kidney disease diagnosis and management: a review. JAMA. 2019;322(13):1294-1304.
- [CrossRef] [PubMed] [Google Scholar]
- et al High levels of fasting glucose and glycosylated hemoglobin values are associated with hyperfiltration in a Spanish prediabetes cohort. The PREDAPS Study. PLoS One. 2019;14(09):e0222848.
- [CrossRef] [PubMed] [Google Scholar]
- et al GFR Study Investigators. Glomerular hyperfiltration and renal disease progression in type 2 diabetes. Diabetes Care. 2012;35(10):2061-2068.
- [CrossRef] [PubMed] [Google Scholar]
- et al Glomerular hyperfiltration in diabetes: mechanisms, clinical significance, and treatment. J Am Soc Nephrol. 2017;28(04):1023-1039.
- [CrossRef] [PubMed] [Google Scholar]
- et al Renal hyperfiltration in prediabetes confirmed by fasting plasma glucose and hemoglobin A1c. Ren Fail. 2012;34(09):1084-1090.
- [CrossRef] [PubMed] [Google Scholar]
- et al CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(09):604-612.
- [CrossRef] [PubMed] [Google Scholar]
- Urinary biomarkers for early diabetic nephropathy in type 2 diabetic patients. Biomark Res. 2015;3:16.
- [CrossRef] [PubMed] [Google Scholar]
- Glomerular hyperfiltration and increased glomerular filtration surface are associated with renal function decline in normo- and microalbuminuric type 2 diabetes. Kidney Int. 2012;81(05):486-493.
- [CrossRef] [PubMed] [Google Scholar]
- et al Prediabetes and risk of glomerular hyperfiltration and albuminuria in the general nondiabetic population: a prospective cohort study. Am J Kidney Dis. 2016;67(06):841-850.
- [CrossRef] [PubMed] [Google Scholar]
- Biomarkers in chronic kidney disease, from kidney function to kidney damage. World J Nephrol. 2015;4(01):57-73.
- [CrossRef] [PubMed] [Google Scholar]
- Is hyperfiltration associated with the future risk of developing diabetic nephropathy? A meta-analysis. Diabetologia. 2009;52(04):691-697.
- [CrossRef] [PubMed] [Google Scholar]
- et al CDC CKD Surveillance Team. Prevalence of chronic kidney disease in US adults with undiagnosed diabetes or prediabetes. Clin J Am Soc Nephrol. 2010;5(04):673-682.
- [CrossRef] [PubMed] [Google Scholar]
- Prediabetes, prehypertension ... is it time for pre-CKD? Clin J Am Soc Nephrol. 2010;5(04):557-559.
- [CrossRef] [PubMed] [Google Scholar]
- Glomerular hyperfiltration in prediabetes and prehypertension. Nephrol Dial Transplant. 2012;27(05):1821-1825.
- [CrossRef] [PubMed] [Google Scholar]
- et al Glomerular hyperfiltration and increased proximal sodium reabsorption in patients with type 2 diabetes or impaired fasting glucose in a population of the African region. Nephrol Dial Transplant. 2010;25(07):2225-2231.
- [CrossRef] [PubMed] [Google Scholar]
- Association of elevated glycosylated hemoglobin A1c with hyperfiltration in a middle-aged and elderly Chinese population with prediabetes or newly diagnosed diabetes: a cross-sectional study. BMC Endocr Disord. 2015;15:47.
- [CrossRef] [PubMed] [Google Scholar]
- for the PREVEND Study Group. Fasting insulin modifies the relation between age and renal function. Nephrol Dial Transplant. 2007;22(06):1587-1592.
- [CrossRef] [PubMed] [Google Scholar]
- et al Differential role of insulin resistance and β-cell function in the development of prediabetes and diabetes in middle-aged and elderly Chinese population. Diabetol Metab Syndr. 2019;11:24.
- [CrossRef] [PubMed] [Google Scholar]
- et al Impaired fasting glucose is associated with renal hyperfiltration in the general population. Diabetes Care. 2011;34(07):1546-1551.
- [CrossRef] [PubMed] [Google Scholar]
- Albuminuria in prediabetes: time to intervene? Endocrine. 2015;48(02):355-357.
- [CrossRef] [PubMed] [Google Scholar]



