
Translate this page into:
Role of fine needle aspiration cytology in diagnosis of brown tumor secondary to parathyroid adenoma
Address for correspondence: Dr. Sandeep S. Ojha, Department of Pathology, Chirayu Medical College and Hospital, Bhopal-Indore Highway, Bairagarh, Bhopal - 462 030, Madhya Pradesh, India. E-mail: drsandy0582@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Brown tumor (BT) is caused by altered metabolism of calcium resulting from hyperparathyroidism (primary or secondary). The most common cause of hyperparathyroidism is isolated parathyroid adenoma (PA), and the most common symptoms are hypercalcemia related. BT is considered as a late manifestation of PA and usually diagnosed after surgical treatment of the bony lesion. Fine-needle aspiration cytology (FNAC) is a cheap, easy, and less traumatic procedure and should be performed in all lesions wherever possible as unnecessary surgeries may be avoided. We here report a rare case of PA presenting primarily as BT and diagnosed on FNAC.
Keywords
Brown tumor
fine-needle aspiration cytology
parathyroid adenoma

Introduction
Brown tumor (BT) (also known as osteitis fibrosa cystica) of bone is a rare benign lesion resulting from abnormal metabolism of bone in hyperparathyroidism.[1] Parathyroid adenoma (PA) is the most common cause of primary hyperparathyroidism.[2] BT is considered as a late manifestation. It commonly involves facial bones, clavicle, ribs, pelvis, and femur.[1] Increased parathyroid hormone (PTH) causes bone resorption by stimulating the osteoclastic activity. These tumors are called brown tumors because of the presence of their brown appearance resulting from vascularity, hemorrhage, and deposition of hemosiderin.[2] BT usually presents as a expansile osteolytic lesion of bone and is difficult to differentiate radiologically from other lytic lesions.
Case Report
A 62-year-old female presented with lower jaw swelling for 2 months which was painful and gradually increasing in size. There was no history of any recent dental intervention, trauma, weight loss, tobacco chewing, or smoking. The patient was not on any medication. On local examination, a firm-to-hard swelling was seen in mandibular region over midline. There was no tenderness or redness over the swelling. Mouth opening was normal and there was no ulcer in the oral mucosa. There was no cervical lymphadenopathy on palpation or on ultrasound. Clinically, the differential diagnosis considered primarily was a bony tumor possibly ameloblastoma or an odontogenic cyst. Computed tomography imaging was asked for and it showed an expansile lytic lesion in midline of the mandible causing erosion of the cortex with extension into the soft tissue in gingivobuccal sulcus [Figure 1]. Based on radiological findings, differentials of myeloma, metastasis, or giant cell tumor were suspected with other primary cystic lesions of mandible. Ultrasound-guided fine-needle aspiration cytology (FNAC) was performed to rule out a malignant process using a 23-G needle under proper aseptic precaution. Cytology smears were hemorrhagic but moderately cellular which showed many multinucleated osteoclast-like giant cells along with few spindled cells [Figures 2 and 3]. There were no epithelial cells ruling out metastasis and there was absence of plasma cells. Given the presence of many giant cells, differentials of giant cell tumor and BT were suggested. Ultrasound of the neck was suggested with simultaneous biochemical investigations. Ultrasound of the neck showed a large, well-marginated hypoechoic lesion in the inferior parathyroid gland measuring 2.2 cm × 2.1 cm. Ultrasound-guided FNAC was performed from parathyroid gland showing features of a PA. Biochemical investigations were also done showing raised serum calcium levels (3.16 mmol/L) and raised PTH levels (516 ng/L). Alkaline phosphatase, renal and liver profiles were within normal limits. Thus, the diagnosis of BT secondary to a PA was made, and parathyroid tumor was excised and sent for histopathological examination showing features consistent with PA [Figure 4]. Postoperatively, there was fall in serum parathormone levels and calcium levels. On follow-up after 1 year, the patient was doing well with no increase in jaw swelling.
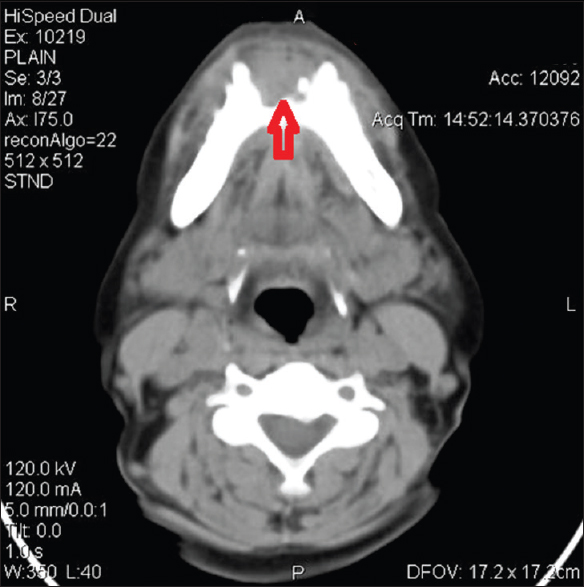
- Computed tomography scan showing lytic lesion in mandible
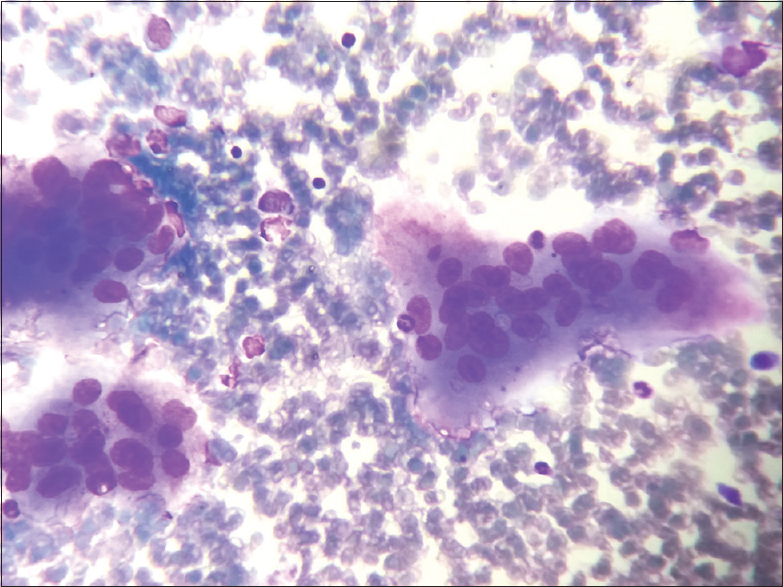
- Fine-needle aspiration cytology smears showing many multinucleate giant cells (Leishman, ×400)
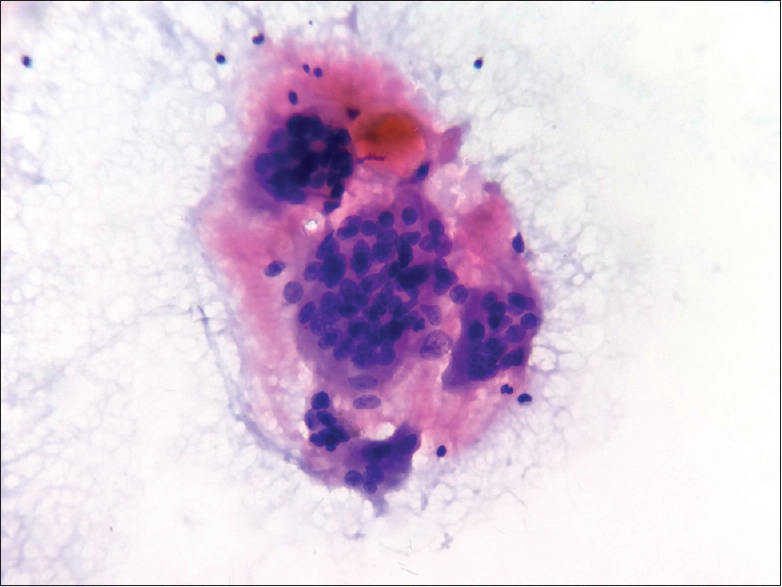
- Fine-needle aspiration cytology smears showing multinucleate giant cells amidst hemorrhagic background (Papanicolaou, ×400)
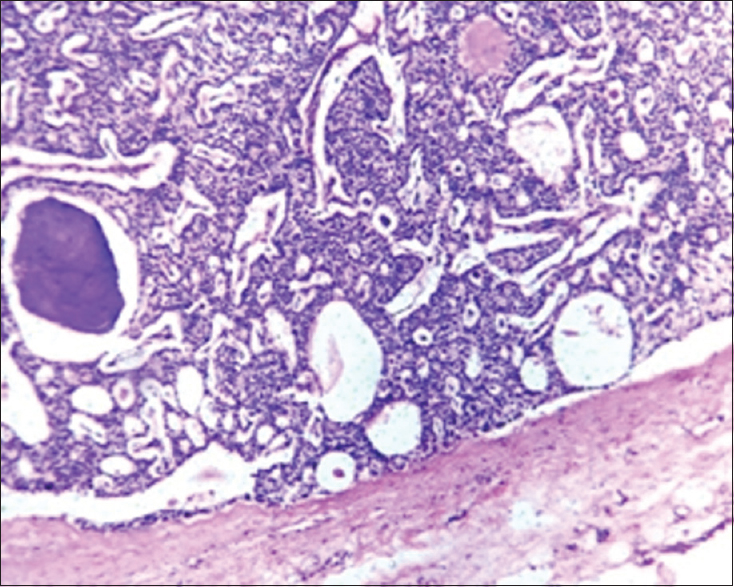
- Histopathology of parathyroid adenoma (×400)
Discussion
BT is a rare and late presentation of hyperparathyroidism, and diagnosis is usually suggested on strong clinical suspicion or after excision of the lesion. Histopathology of BT shows the presence of many multinucleated giant cells and spindle cells with or without hemorrhage and is indistinguishable from other giant cell lesions such as giant cell tumor or central giant cell granuloma. However, the diagnosis of even a giant cell lesion requires either excision or biopsy from the lesion which is more invasive, traumatic, or disfiguring procedure. There are many case reports suggesting the possibility of BT after excision or biopsy of the lesion, but the role of cytology in suggesting BT is mentioned in very few case reports.[345] First, it can rule out malignant causes of lytic lesions such as metastasis or myeloma and also can suggest the probable diagnosis without excising the lesion. Cytology in cases of BT may help in proper management of the patients as just excision of the lesion does not lead to complete treatment and patients may present later with other bony lesions because of continuous secretion of PTH. Parathyroidectomy is well known to cause resolution of lytic lesions without any surgical intervention to bone. In our case also, after 1 year of parathyroidectomy, the lesion was not increased and was mildly regressed. Other treatment options range from enucleation and curettage, resection, radiation therapy, and chemotherapy.
Conclusion
FNAC is a cheap, easy, minimally invasive, and less disfiguring technique and should be performed in any lytic lesion of bone. We report this case because it highlights the importance of cytology along with biochemical investigations in the diagnosis of BT without any surgical intervention.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Peripheral brown tumour of hyperparathyroidism in the oral cavity. Oral Oncol Extra. 2006;42:91-3.
- [Google Scholar]
- Brown tumour of the maxilla and mandible: A rare complication of tertiary hyperparathyroidism. Dentomaxillofac Radiol. 2009;38:53-8.
- [Google Scholar]
- Fine needle aspiration diagnosis of osteitis fibrosa cystica (brown tumor of bone): A case report. Acta Cytol. 2008;52:471-4.
- [Google Scholar]
- Fine-needle aspiration of brown tumor of bone: Cytologic features with radiologic and histologic correlation. Diagn Cytopathol. 2009;37:136-9.
- [Google Scholar]



