
Translate this page into:
Salmonella typhimurium infection in total knee arthroplasty: A case report with review of literature
Address for correspondence: Dr. Benu Dhawan, Department of Microbiology, All India Institute of Medical Sciences, New Delhi - 110 029, India. E-mail: dhawanb@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Salmonella enterica serotype Typhimurium is a rare cause of prosthetic joint infection (PJI). The recognized predisposing risk factors for Salmonella septic arthritis include diabetes mellitus, renal failure, human immunodeficiency virus infection and chronic corticosteroid use. We describe a case of PJI of the knee in a 74-year-old lady who was on antitubercular treatment. The patient presented with discharging sinus and raised inflammatory markers. She was successfully treated by the removal of prosthesis and debridement followed by ciprofloxacin therapy for 6 weeks. This case report highlights the potential virulence of Salmonella in immunocompromised patient with a joint prosthesis. Continuous monitoring and close collaboration of microbiologists and orthopedicians helped obtain the resolution of infection in our patient.
Keywords
Debridement
immunocompromised
nontyphoidal Salmonella
prosthetic joint infection

Introduction
Infection of the prosthesis remains one of the most devastating complications of prosthetic joint replacement surgery. Prosthetic joint infections (PJIs) of total knee arthroplasty (TKA) occur with an incidence of 2.05%–2.18%.[1] The most common causative organism in PJI is Staphylococcus, accounting for >50% of cases.[2] PJI due to Salmonella spp. is a rare condition and the literature search reveals only thirty cases to be reported worldwide.[34] In majority of these cases, immunosuppression was said to be a major contributing factor.
We describe a case of TKA infection due to Salmonella typhimurium.
Case Report
A 72-year-old lady presented to our orthopedics outpatient department with a 5-month history of severe pain, swelling and discharging sinus from the right knee. She had undergone an uncomplicated bilateral TKA for osteoarthritis four years back.
The medical history revealed diabetes mellitus, hypertension and seizure disorder. A year ago, the patient was diagnosed with tubercular meningitis for which she underwent ventriculoperitoneal shunt procedure and was started on antitubercular treatment. Physical examination showed swelling of the right knee with discharging sinus, tenderness to palpation and painful movements. The range of motion was severely limited. The sinus discharge was from two different sites; one over the distal scar margin and another from the lateral aspect of the right patella. Laboratory data included a total leukocyte count of 6200/mm3, with 61.1% polymorphonuclear leukocytes, erythrocyte sedimentation rate (ESR) of 88 mm/h and a C-reactive protein level of 51.3 mg/L. Radiographs of the right knee revealed loosening of the prosthesis. The patient was subsequently posted for implant removal, debridement and cement spacer application as Stage I procedure of staged periprosthetic infection control.
Intraoperatively, the patella was found to be dislocated and collection of frank pus was seen in superomedial pocket of the right knee. For microbiological and histological investigations, pus and three periprosthetic tissue samples were taken. The pus was drained out and all prosthesis components and cement were removed, following which thorough soft tissue debridement and insertion of nonarticulating antibiotic impregnated (gentamicin) cement spacer were done [Figure 1]. Gram stain of the drained pus showed numerous polymorphonuclear leukocytes but no organisms. The patient was empirically started on cefuroxime 1.5 g 12-hourly and levofloxacin 500 mg 24-hourly.

- Anterior-posterior (a) and lateral (b) radiographs of the right knee showing cement spacer in situ
Pus, synovial fluid and three tissue specimens were processed in accordance with recognized standard operating procedures.[5] All four specimens after 24 h of incubation yielded a pure growth of nonlactose fermenting colonies on MacConkey agar. Standard microbiological methods were followed for isolation and identification of the organism. On the basis of the battery of biochemical tests and serotyping by Salmonella antisera (SSI, Denmark), the organism was identified as Salmonella typhimurium. Antibiotic susceptibility was determined by Kirby-Bauer disk diffusion method in accordance with Clinical Laboratory Standards Institute guidelines.[6] The strain was susceptible to ampicillin, cefuroxime, ceftriaxone, ceftazidime, chloramphenicol, ciprofloxacin, levofloxacin and cotrimoxazole but resistant to nalidixic acid. According to the susceptibility pattern of the strain, the antibiotic regime was rationalized to intravenous ceftazidime 2 g 12-hourly. Postsurgical blood and stool samples were sterile. Histopathology report showed chronic inflammation with inflammatory granulation tissue. With 2 weeks of therapy, the patient showed remarkable clinical improvement and her wound was clean, dry and intact. She was discharged on oral ciprofloxacin 600 mg 12-hourly, for 6 weeks. At 8 weeks follow-up, the wound was completely dry and her inflammatory markers settled to normal. The patient was pain-free and there was no sign of infection. However, the patient was unwilling for any further reconstructive procedure.
Discussion
PJI is one of the most dreaded complications of total joint arthroplasty. Mostly, PJIs are caused by Gram-positive bacteria. Gram-negative bacteria, which are less commonly associated with PJIs, constitute <10% of all episodes.[2] PJI caused by Salmonella species is rare; so far, only nine prosthetic knee infections have been described.[37]
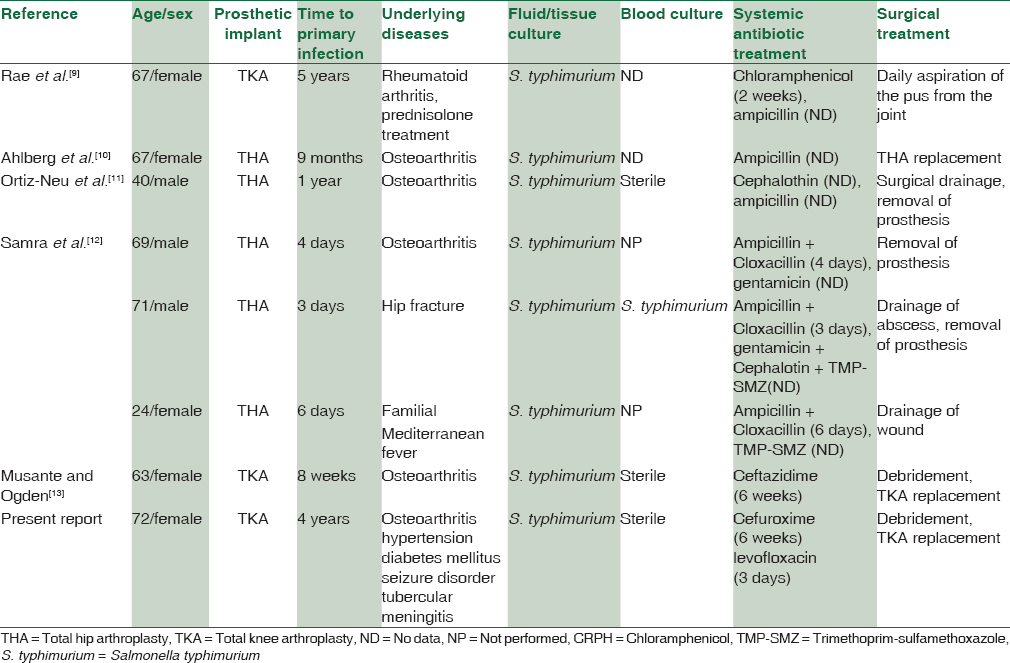
Most Salmonella serotypes can cause mild to severe infection in humans and in a variety of animal species. Septic arthritis caused by Salmonella is less frequent and accounts for only 0.1%–0.2%.[8] The most commonly encountered serotypes of Salmonella in bone infections are Salmonella enteritidis (Group B) and S. typhimurium (Group D). Till date, only seven cases of PJI due to S. typhimurium have been described in literature, of which only two were involved the knee joint [Table 1].[910111213]
Infection with nontyphoidal Salmonella most often results in self-limiting acute gastroenteritis. However, no gastrointestinal symptoms were seen in our patient. This is in concordance with the findings of other researchers who have reported Salmonella associated PJI without any overt gastrointestinal manifestation.[314]
This is a case of late onset PJI as the infection occurred after four years of primary surgery and the possibility of any intraoperative contamination is quite unlikely. Although hematogenous dissemination of Salmonella is a well-established and the most likely mechanism of PJI;[1011] in the present case, this route of dissemination was unlikely since postoperative blood cultures were sterile. However, since our patient was on antitubercular treatment for the past one year, we speculate that this could have altered the symbiotic normal intestinal flora leading to the overgrowth of inherently pathogenic organisms such as S. typhimurium. In addition to this, impairment of cell-mediated immunity in tuberculosis and infection of the macrophages by Mycobacteria may have impaired their ability to kill other intracellular pathogens such as Salmonella.
Nontyphoidal Salmonella strains with nalidixic acid resistance have emerged among human cases. The S. typhimurium strain isolated from our patient was resistant to nalidixic acid. Recommended antimicrobials for salmonella infections include chloramphenicol, ampicillin, trimethoprim-sulfamethoxazole, third-generation cephalosporins and fluoroquinolones.[15] The enhanced potency of third-generation cephalosporins and the ability of the fluoroquinolones to penetrate macrophages make them as the most preferred drug for treatment.
Conclusion
We report the first case of PJI due to S. typhimurium from India. Total joint replacement surgery is a relatively common orthopedic surgical procedure and includes a significant number of elderly and immunocompromised patients. Although the Salmonella infection in prosthetic joints is rare; nonetheless, it should be considered in symptomatic and immunocompromised patients with joint prosthesis. Early diagnosis, appropriate surgical strategy and aggressive antimicrobial therapy are necessary for the successful long-term results of Salmonella PJI without risking further recurrence.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8 Suppl):61-5.e1.
- [Google Scholar]
- One-stage revision in two cases of Salmonella prosthetic hip infection. World J Clin Cases. 2014;2:304-8.
- [Google Scholar]
- Prosthetic joint infection due to Salmonella species: A case series. BMC Infect Dis. 2014;14:633.
- [Google Scholar]
- Diagnosis of periprosthetic joint infections of the hip and knee. J Am Acad Orthop Surg. 2010;18:760-70.
- [Google Scholar]
- Clinical Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. 25th Informational Supplement M100-S25. Wayne, Pennsylvania, USA: Clinical Laboratory Standards Institute; 2015.
- Recurrent prosthetic joint infection due to Salmonella enteritidis: Case report and literature review. Eur J Orthop Surg Traumatol. 2012;22(Suppl 1):89-97.
- [Google Scholar]
- Salmonella species. In: Pegues DA, Miller SI, eds. Mandell, Douglas and Bennett's Principles and Practice of Infectious Diseases (8th ed). Philadelphia: Elsevier Saunders; 2015. p. :2567.
- [Google Scholar]
- Salmonella typhimurium arthritis in rheumatoid disease. Rheumatol Rehabil. 1977;16:150-1.
- [Google Scholar]
- Hematogenous infection in total joint replacement. Clin Orthop Relat Res. 1978;137:69-75.
- [Google Scholar]
- Nontyphoid salmonellosis in patients with total hip replacement: Report of four cases and review of the literature. Rev Infect Dis. 1986;8:978-83.
- [Google Scholar]
- Salmonella septic arthritis following total knee arthroplasty for rheumatoid arthritis in a patient receiving etanercept. J Orthop Sci. 2011;16:258-62.
- [Google Scholar]
- Antimicrobial drug resistance in Salmonella: Problems and perspectives in food- and water-borne infections. FEMS Microbiol Rev. 2002;26:141-8.
- [Google Scholar]



