
Translate this page into:
Schistosomiasis of the Appendix in a Tertiary Hospital in Northern Nigeria: A 22-Year Review
Address for correspondence: Dr. Saad A Ahmed, E-mail: sahmednl@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Schistosomiasis is one of the neglected tropical diseases caused by a trematode, Schistosoma spp, and affects many systems in the body including the gastrointestinal tract. Schistosomiasis of the appendix is a well-recognized disease and presents as a chronic granulomatous inflammation. This study aims to document the frequency and pattern of distribution of schistosomal appendicitis in our environment.
Materials and Methods:
This is a retrospective histopathological review of schistosomiasis of the appendix in the Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria - Nigeria, between January 1, 1991 to December 31, 2012.
Results:
Within the study period, there were 1,464 appendectomy specimens histologically examined in the Pathology Laboratory. Thirty of these, representing 2.1%, were diagnosed as schistosomiasis of the appendix. The male:female ratio was 6.5:1 and peak age incidence was in the 20-29 years age group. Abdominal pains, vomiting and fever were seen in 23 (76.7%) and altered bowel motion in seven (23.3%) patients.
Conclusion:
This study showed that schistosomiasis of the appendix is not rare and that its presentation is similar to other forms of appendicitis. There is a need to focus on the prevention of schistosomiasis in order to reduce morbidity among these economically viable age groups.
Keywords
Appendicitis
Nigeria
schistosomiasis

INTRODUCTION
Schistosomiasis is one of the neglected tropical diseases and the World Health Organization (WHO) estimates that 500-600 million people in tropical and subtropical countries are at risk for schistosomiasis and that over 200 million people are infected.[12] The species of major global importance are Schistosoma haematobium, S. mansoni and S. japonicum.[3] All the three species deposit eggs in the appendix, but schistosomiasis seldom cause appendicitis.[45] Schistosomiasis of the appendix is a well-recognized disease. Some reports have implicated S. haematobium, S. mansoni and S. japonicum species in having a preference for the appendix.[6789]
This study reports the frequency distribution and clinico-pathological findings of 30 cases of schistosomal appendicitis seen in a tertiary hospital in Northern Nigeria.
MATERIALS AND METHODS
The study was a retrospective histopathological study of appendectomy specimens in the Pathology Laboratory of the Ahmadu Bello University Teaching Hospital Zaria - Nigeria over a 22- year period between January 1, 1991 and December 31, 2012. Clinical data on each case were extracted from the respective copies of the request cards. All tissues had been previously fixed in formalin. The hematoxylin and eosin (H and E)-stained slides were retrieved in each case and reviewed microscopically by the authors. Where slides were missing or broken, fresh sections were taken from the paraffin-embedded tissue blocks of the specimens and stained.
Cases in whom the bio-data, clinical details, slides and/or tissue blocks were missing were excluded from the study. The results are presented in a tabular form and analyzed using simple frequency distribution.
RESULTS
Over the 22-year period, 1464 appendectomy specimens were received and 30 of these were diagnosed as schistosomal appendicitis representing 2.1% of all cases [Figure 1]. There were 26 males and four females, with male: female ratio of 6.5:1 [Table 1], with an age range of 13-55 years and a peak age incidence in the third decade. The presenting complaints were abdominal pains, vomiting and fever, seen in 23 (76.7%) and altered bowel motion in seven (23.3%) patients [Table 2].
- Frequency of Schistosomal appendicitis among appendectomy specimens


Gross examinations of the specimen showed features of acute appendicitis with fibrinopurulent exudates in five cases, serosa congestion and thickened wall in 10 case, and 15 cases were grossly unremarkable; however fecaliths were identified in 24 cases. Microscopic examinations showed that all the appendices had Schistosoma ova in the mucosa and/or different parts of the wall [Figure 2]. The ova were morphologically consistent with S. haematobium in 29 cases, while one case was consistent with S. mansoni. Morphologically, S. haematobium ova have a terminal spine while S. mansoni have lateral spine. The other tissue reactions include submucosal fibrosis, active granuloma formation with tissue eosinophilia and infiltrates of acute and chronic inflammatory cells.
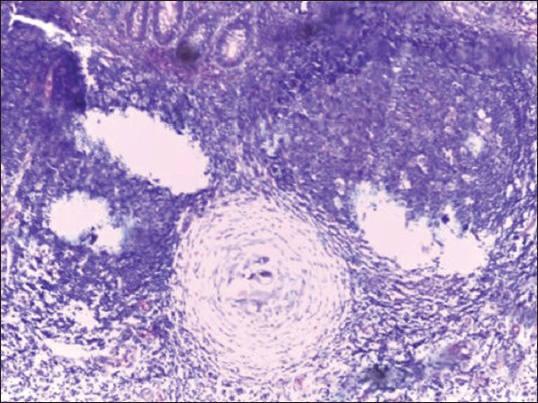
- Section showing schistosoma ova within a granuloma and surrounded by chronic inflammatory cells’ infiltrate (H and E, ×200)
DISCUSSION
Schistosomiasis is an important and highly prevalent trematode infection affecting approximately 200 million people in tropical and sub-tropical countries.[1] Schistosomiasis is endemic in many parts of Nigeria. The incidence of schistosomal appendicitis from this study is 2.1% [Figure 1], which is similar to 2.3% reported by Gali et al.[10] in Maiduguri and 2.4% observed by Adebamowo et al.[7] in Ibadan. However, our report is higher than the report by Ojo et al.,[8] with values of 0.9%, but lower than the 4.15% value observed by Badmos et al.[9] and 9% value observed by Attah et al.[11] in Ibadan. The reason for the fall in the incidence is probably due to the improvement of provision of social and medical amenities, and treatment with effective drugs in Nigeria. In developed countries like the USA, Japan and Ankara, schistosomal appendicitis is very rare, with an incidence of 0.2%, 0.34% and 0.05%, respectively.[121314] These are reports from nonendemic areas and higher socioeconomic indices as well.
Most cases were seen in the second and third decades of life, with a peak incidence in the third decade [Table 1], and this is similar to that reported by Adekunle et al.[15] and Adisa et al.[16]. However, this is higher compared with the peak age incidence of acute appendicitis observed in the second decade by Badmos et al.[9]
The clinical features are not different from other reports. Abdominal pains, vomiting and fever remain the most common initial symptoms, and were present in 23 (76.7%) of the patients, and altered bowel motion in seven (23.3%) patients was the second most common symptom [Table 2]; this is similar to other reported series.[910111215]
The histopathological findings are not quite different from reports in the subregion, except that S. haematobium was the sole agent in appendiceal schistosomiasis from this report in 29 (96.7%) cases, which is in contrast to S. mansoni as reported in some series in Nigeria.[817] This could be due to the fact that S. haematobium is endemic in this environment and it has been established that in an endemic area, it is not uncommon to be found in the appendix.[4591018] The gold standard of diagnosis is identification of the ova by either histology in a tissue or microscopy of the urine or feces; in the tissue, the basic lesions of schistosomiasis are circumscribed granuloma around eggs or a diffuse cellular infiltrate around eggs by eosinophils and neutrophils [Figure 2]. Plasma cells, lymphocytes, macrophages and giant cells are also usually present.[4] The granulomata vary in structure and the only pathognomomic feature is the contained eggs. Some eggs are surrounded by a layer of eosinophilic material, the Splendore–Hoeppli phenomenon.[45] Schistosoma egg are readily demonstrable under H and E stain.[4] Sometimes, special stains could be used to demonstrate schistosoma ova in the tissues. Because the ova are usually surrounded by periodic-acid Schiff (PAS)-positive diastase-resistant materials, these stains can be used.[19] In addition, the egg shells of S. mansoni and S. intercalatum are acid fast, while those of S. haematobium are not.[4] In the present report, special stains were not performed due to the fact that schistosoma ova were easily demonstrated morphologically in the tissue sections stained with H and E.
This report has not only confirmed the impression of some earlier authors that schistosomiasis can cause appendicitis but also confirmed that it should be considered as a differential diagnosis in patients who are in their third decade of life with features of appendicitis. In all our cases, there was no prior clinical suspicion of schistosomiasis. Also, appendectomy specimens should be sent for histopathological review so that patients could benefit from full investigation and treatment.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- World Health Organization. Schistosomiasis Control. Division of Control of Topical Diseases. Geneva: World Health Organization; 1998.
- [Google Scholar]
- Mansoni's schistosomiasis of a leiomyoma: Case report. 2007. Clinics. 62:529-30. HYPERLINK “http://www.ncbi.nlm.nih.gov/pubmed/17823718” \o “Clinics (São Paulo, Brazil)” (Sao Paulo)
- [Google Scholar]
- Clinical findings in female genital schistosomiasis in Madagascar. Trop Med Int Health. 1998;3:327-32.
- [Google Scholar]
- Schistosomiasis. In: Chapman HB, Daniel HC, eds. Pathology of Tropical and Extra Ordinary Diseases. Vol 2. Washington DC: Armed Forces Institute of Pathology; 1976. p. :482-508.
- [Google Scholar]
- Edington GM, Gilles HM, eds. Pathology in the Tropics. London: Edward Arnold Publishers Ltd; 1976. p. :149-79.
- A quantitative post mortem analysis of urinary schistosomiasis in Egypt. I. Pathology and pathogenesis. Am J Trop Med Hyg. 1974;23:1054-71.
- [Google Scholar]
- Review of the histopathological findings in appendices removed for acute appendicitis in Nigerians. J R Coll Surg Edinb. 1991;36:245-8.
- [Google Scholar]
- Schistosomiasis: A rare cause of acute appendicitis in the African American population in the United States. Am Surg. 2008;74:221-3.
- [Google Scholar]
- Schistosomal appendicitis: Incidence in Japan and a case report. World J Gastroenterol. 2009;15:1648-9.
- [Google Scholar]
- Unusual findings in appendectomy specimens: Evaluation of 2458 cases and review of the literature. Indian J Surg. 2004;66:221-6.
- [Google Scholar]
- Clinicopathological review of schistosomal appendicitis in south western Nigeria. Trop Gastroenterol. 2009;30:230-2.
- [Google Scholar]
- Pattern and outcome of acute appendicitis in semi-urban and rural African communities: A study of 125 patients. Niger Med Pract. 1998;36:8-11.
- [Google Scholar]
- Appendicitis in Kano, Nigeria: A 5-year review of pattern, morbidity and mortality. Ann Afr Med. 2004;3:38-41.
- [Google Scholar]
- Splendore-Hoeppli phenomenon. In: Chapman HB, Daniel HC, eds. Pathology of Tropical and Extraordinary Diseases. Vol 2. Washington DC: Armed Forces Institute of Pathology; 1976. p. :681-3.
- [Google Scholar]



