
Translate this page into:
Sertoliform Endometrioid Tumor of Ovary Presenting as Torsion
Address for correspondence: Dr. Prathiksha Pai, E-mail: prathikshashenvi@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Sertoliform endometrioid carcinoma of the ovary (SEC) is an uncommon variant that bears histologic similarity to sertoli and sertoli-leydig cell tumors. We report an interesting case of SEC in a 55-year-old female with a left ovarian mass with torsion. Histology revealed an SEC, featuring foci of typical endometrioid carcinoma, and areas composed of uniform, small, hollow tubules lined by columnar cells with apical cytoplasm. Tumor cells were strongly immunoreactive for EMA and cytokeratin but negative for inhibin; thus, confirming the diagnosis of SEC ovary. Recognition of this tumor is important as it is a well-differentiated, low-grade malignancy that displays good prognosis when confined to the ovary.
Keywords
Endometrioid tumor
ovary
sertoliform variant

INTRODUCTION
Sertoliform endometrioid carcinoma of the ovary (SEC) is an uncommon variant that bears histologic similarity to sertoli and sertoli-Leydig cell tumors (SLTs).[1] This morphologic similarity may serve as a potential diagnostic pitfall for the pathologist. Recognition of this tumor is important as it is a well-differentiated, low-grade malignancy that displays a good prognosis when confined to the ovary.[12]
CASE REPORT
A 55-year-old postmenopausal female patient presented with mass per abdomen since 2 years and pain for 2 days. There was no history of bleeding per vagina. No signs of virilization were noted clinically. Per-abdomen tender mass was felt in left hypogastric and iliac fossa. Ultrasonography showed multicystic lesion measuring 12 cm × 11 cm in the left ovary [Figure 1]. Intraoperatively, left ovarian cyst showed torsion with rupture of cyst wall. Total hysterectomy with bilateral salpingo-oophorectomy was done.

- Ultrasonography showing multicystic lesion measuring 12 cm × 11cm in the left ovary
On gross examination, ovary weighed 550 g, measured 13 cm × 11 cm × 7 cm, showed solid and cystic areas on cut section [Figure 2]. Microscopy showed round to solid tubules lined by pseudostratified columnar epithelium with elongated nuclei resembling sertoli tumor-like pattern along with conventional endometrioid tumor [Figures 3–5]. Utero-cervix and rest of adnexa were unremarkable. A histopathological diagnosis of SEC of left ovary was made.
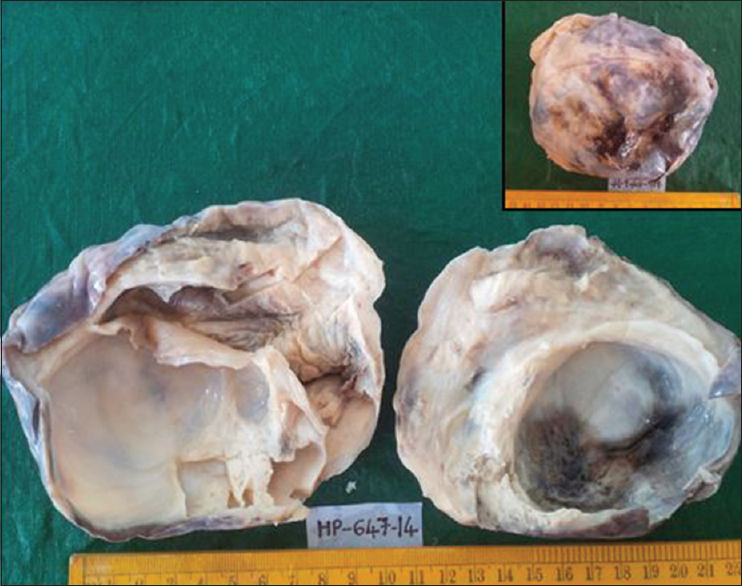
- Left ovarian tumor with cut surface showing cystic and gray-white solid areas. Inset: Outer surface showing blackish areas due to torsion
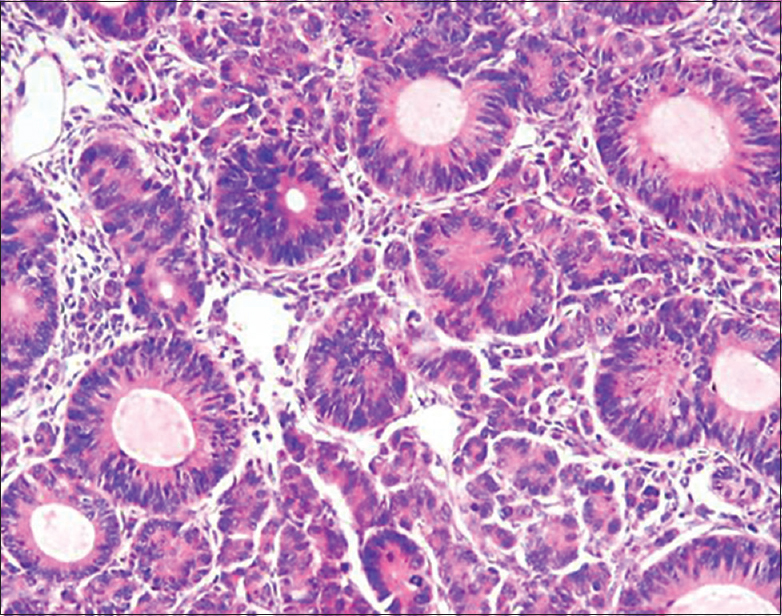
- Microphotograph showing sertoliform endometrioid carcinoma showing tubules and tightly packed nests of tumor cells separated by fibrous stroma. Individual tumor cells having vesicular nuclei, prominent nucleoli, and moderate cytoplasm (H and E, ×400)
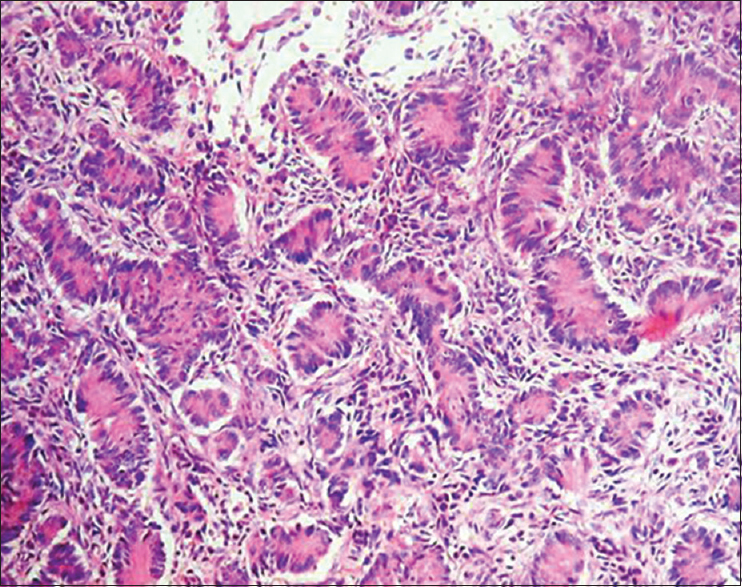
- Microphotograph showing foci of conventional endometrioid carcinoma (H and E, ×400)
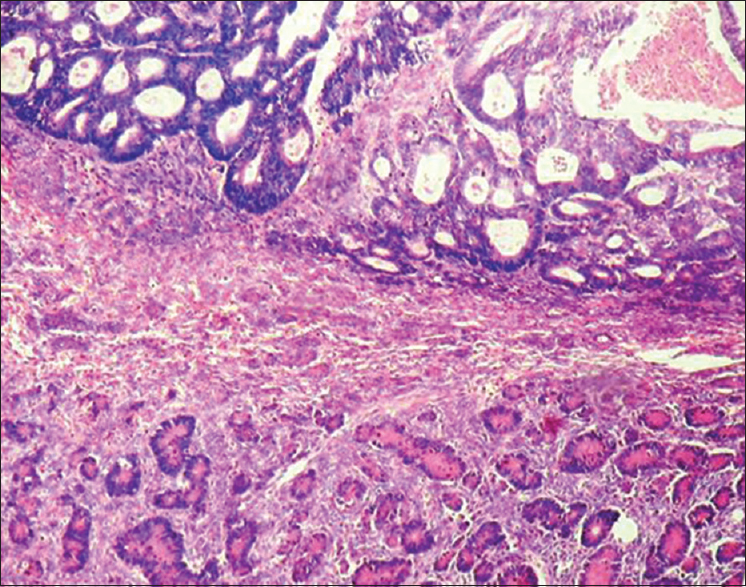
- Microphotograph showing foci of conventional endometrioid carcinoma and sertoli cell tumor-like pattern (H and E, ×200)
Immunohistochemistry (IHC) showed tumor cells strongly immunoreactive for epithelial membrane antigen (EMA), cytokeratin (CK) but negative for inhibin [Figures 6–8], thus confirming the diagnosis of SEC of left ovary.
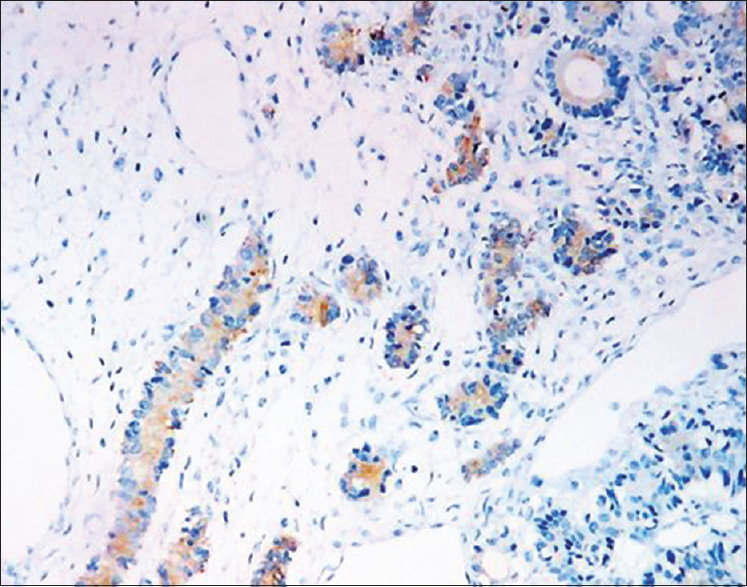
- Sertoliform endometrioid carcinoma showing cytokeratin positivity (immunohistochemistry, ×200)
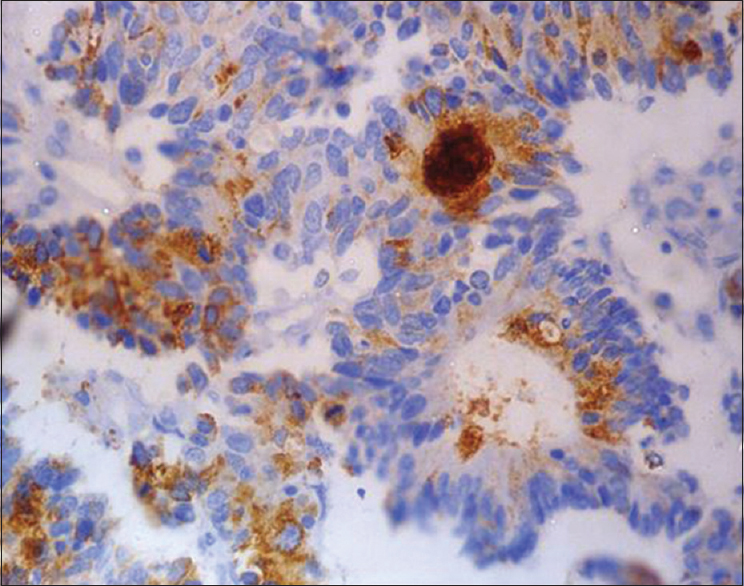
- Sertoliform endometrioid carcinoma showing epithelial membrane antigen positivity (immunohistochemistry, ×400)
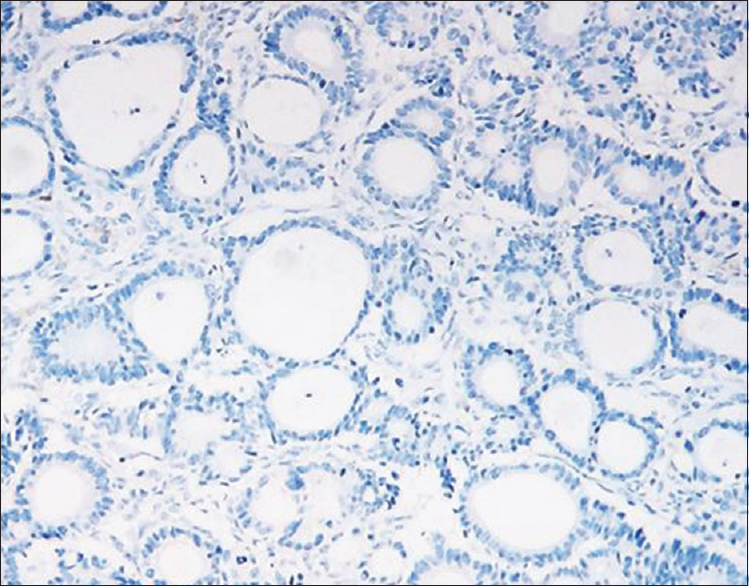
- Sertoliform endometrioid carcinoma showing inhibin negativity (immunohistochemistry, ×400)
DISCUSSION
Endometrioid carcinoma of ovary resembling sex cord-stromal tumor is a rare variant of endometrioid adenocarcinoma that focally looks like a sex cord-stromal tumor with sertoli, leydig, or granulosa cells. The histologic similarities of SEC and SLTs can be confusing even to experienced consultants. Ordi et al., in their study, reported that SEC typically demonstrates the following characteristics, while SLTs do not: (1) Presence of areas with usual pattern of endometrioid carcinoma, (2) presence of mucin at the apical borders of the tumor cells.[3]
Other factors that may favor SEC would include squamous or squamoid areas, well-developed cilia, the presence of endometriosis, or a concomitant adenocarcinoma of the endometrium.[4]
IHC is of great value in the differential diagnosis. Immunostains for alpha-inhibin is positive in most neoplastic sertoli cells but negative in the cells of endometrioid carcinoma, while positive EMA and CK immunostains favor SEC.[5]
Despite histologic similarity, there are important clinical differences between the SEC and SLT patient populations. Misir and Sur in their study report that in SLTs, the patient age tends to be younger, with an average age of 25 years and clinically, up to 50% of SLT patients may exhibit endocrine manifestations. In contrast, SEC occurs almost exclusively in postmenopausal women with an average age of 68 years. Virilizing symptoms, though uncommon in endometrioid carcinoma, may be encountered in the sertoliform variant, thus compounding the diagnostic difficulty.[6] In our case, the patient was in her postmenopause with no signs of virilization. She had SEC and presented with torsion which is extremely rare.
Recognition of SEC is important for grading of endometrioid adenocarcinoma. Usually, solid portion of endometrioid adenocarcinoma is considered as Grade 3 according to the International Federation of Obstetrics and Gynecologists grading system.[7] SEC should be considered as Grade 1 (well-differentiated), despite the presence of solid, sex cord-like proliferation as it carries good prognosis when confined to ovary.[13] According to these suggestions, our case is graded as well-differentiated (Grade 1) based on the histological features of foci of conventional endometrioid carcinoma. Patient is kept under close follow-up for any recurrence.
CONCLUSION
The case is presented for its rarity. In view of relatively good prognosis of SEC as compared to Endometrioid tumor, identifying this variant by an extensive sampling of the specimen is mandatory.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Sertoliform endometrioid carcinoma of the ovary: A potential diagnostic pitfall. Arch Pathol Lab Med. 2007;131:979-81.
- [Google Scholar]
- Ovarian sertoliform endometrioid carcinoma: A diagnostic dilemma. Indian J Pathol Microbiol. 2013;56:327-8.
- [Google Scholar]
- Sertoliform endometrioid carcinomas of the ovary: A clinicopathologic and immunohistochemical study of 13 cases. Mod Pathol. 1999;12:933-40.
- [Google Scholar]
- Ovarian endometrioid tumors mimicking sertoli and sertoli-leydig cell tumors: Sertoliform variant of endometrioid carcinoma. Cancer. 1982;50:1322-31.
- [Google Scholar]
- Ovarian carcinomas, including secondary tumors: Diagnostically challenging areas. Mod Pathol. 2005;18(Suppl 2):S99-111.
- [Google Scholar]
- Surface epithelial tumors of the ovary. In: Kurman R, ed. Blaustein's Pathology of the Female Genital Tract (5th ed). New York: Springer-Verlag Inc; 2002. p. :791-886.
- [Google Scholar]
- The utility of the revised International Federation of Gynecology and Obstetrics histologic grading of endometrial adenocarcinoma using a defined nuclear grading system. A Gynecologic Oncology Group study. Cancer. 1995;75:81-6.
- [Google Scholar]



