
Translate this page into:
Sister Mary Joseph’s nodule: A rare site for a common malignancy

*Corresponding author: Kafil Akhtar, Department of Pathology, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. drkafilakhtar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Patil S, Kratee K, Hassan MJ, Akhtar K. Sister Mary Joseph’s nodule: A rare site for a common malignancy. J Lab Physicians. 2025;17:142-5. doi: 10.25259/JLP_149_2024
Abstract
Sister Mary Joseph’s nodule is identified by detectable lumps that extend into the umbilicus due to the spread of cancer from the abdominal or pelvic regions. Commonly, these cancers originate from the gastrointestinal or genital areas, but other sources are rare. Our case involved a 27-year-old female who came with an umbilical swelling with bilateral adnexal growth. Laboratory, radiological, and histopathological examinations led to a diagnosis of adenocarcinoma ovary, with metastasis to the umbilicus. To our knowledge, this is a rare presentation of common abdominal malignancy, and therefore, this presentation should be kept in mind for an early diagnosis and better outcome.
Keywords
Adenocarcinoma
Ovary
Sister Mary Joseph’s nodule
Umbilical metastasis

INTRODUCTION
The term “Sister Mary Joseph’s nodule” refers to an umbilical nodule that serves as a cutaneous metastasis originating from a primary cancer. This designation honors a nurse recognized for identifying the link between this symptom and advanced stages of cancer.[1]
Typically, the malignancy associated with this nodule arises from adenocarcinomas in the gastrointestinal or genitourinary systems. However, sources from hematological origins, as well as pulmonary or breast cancers, are also documented.[2] Herein, we report a case of adenocarcinoma ovary with metastasis to the umbilicus.
CASE REPORT
A 27-year-old female patient presented to the Obstetrics and Gynecology Outpatient Department with complaints of abdominal distention for the past 2–3 months, along with an umbilical nodule. Physical examination showed a moderate to grossly distended abdomen and an inflamed and ulcerated brownish-black nodule around the umbilicus measuring 2 cm × 1.5 cm with satellite nodules measuring <1 cm [Figure 1]. She also complained of multiple episodes of loose stools and nausea with abdominal pain on and off (suggestive of widespread carcinomatosis).
Serum markers of carbohydrate antigen (CA) – 125 (323.0 U/mL) and beta-human chorionic gonadotropin (858 m/U/mL) were elevated. An abdominal contrast-enhanced magnetic resonance tomography showed a large solid cystic mass of size 11 × 16 × 16.5 cm in bilateral adnexa with multiple enhancing lymph nodes, the largest of size 5 × 5.5 cm along bilateral common iliac vessels and bilateral external iliac vessels [Figure 2]. The patient underwent ascitic fluid tap and cytology was suggestive of metastatic malignancy [Figure 3]. An umbilical skin biopsy was evaluated for pathological examination. The histopathology was suggestive of adenocarcinoma infiltrating the underlying dermis with occasional signet cells (Sister Mary Joseph’s Nodule) [Figure 4]. She administered 3 weekly 3 cycles of carboplatin, 220 mg/m2 and paclitaxel, 50 mg/m2-based chemotherapeutic regimen. She is doing well at 3 months of follow-up period.
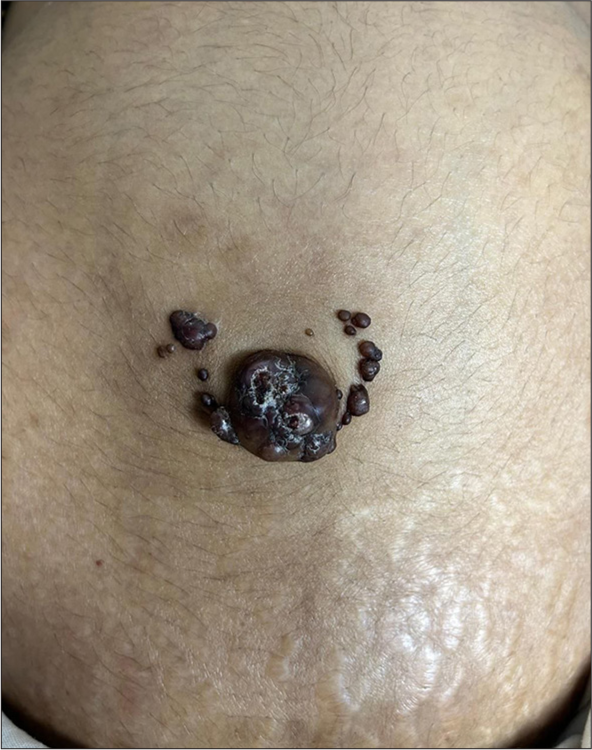
- Clinical image showed multiple brownish-black nodules with satellite nodules around the umbilicus.

- Contrast-enhanced magnetic resonance imaging of the abdominal cavity and pelvis showed an expansive tumorous formation covering the uterus with carcinomatosis of the peritoneum (transversal view).
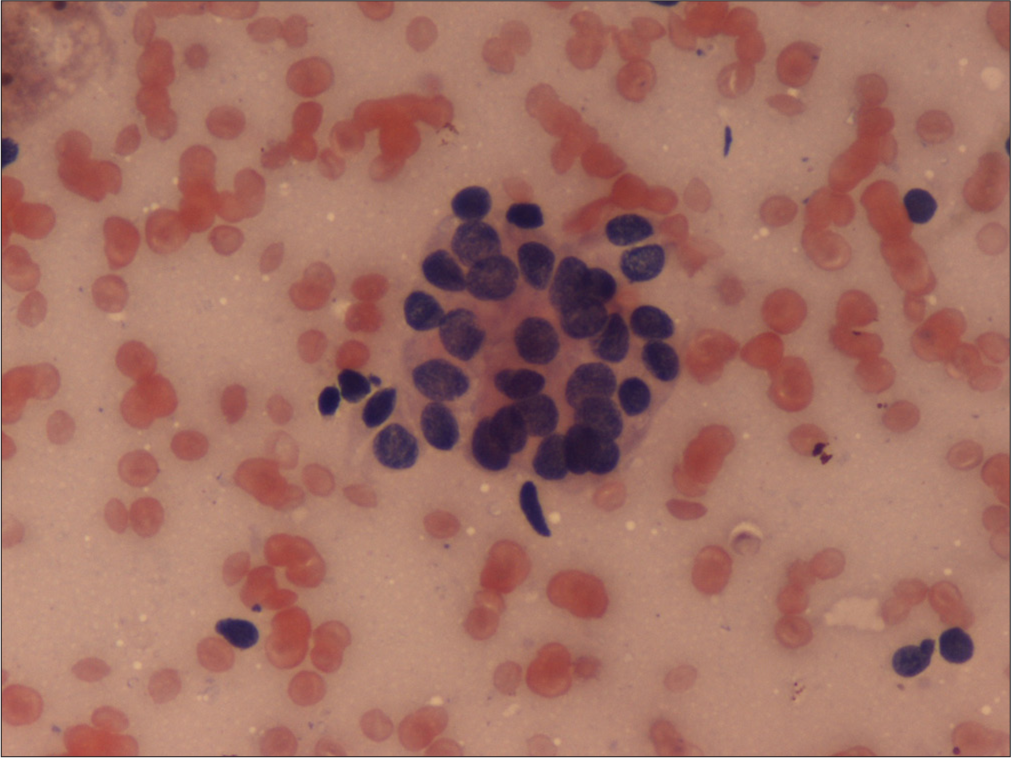
- Fine needle aspiration cytology was suggestive of metastatic malignancy. Hematoxylin and eosin ×40.
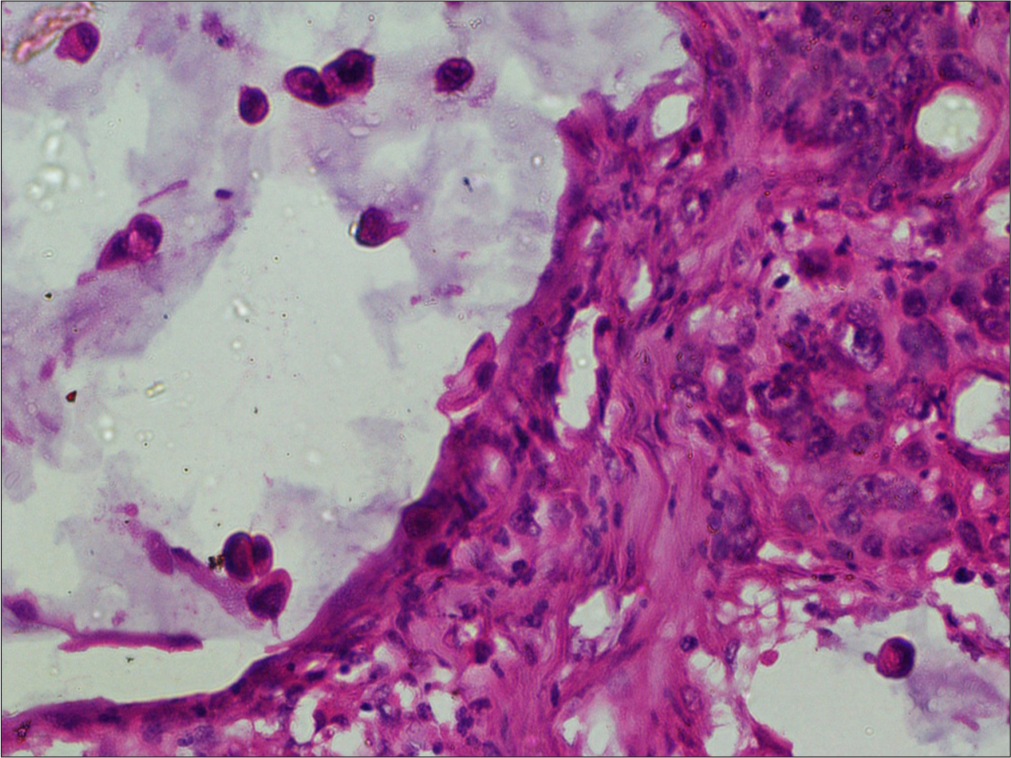
- The histopathology was suggestive of adenocarcinoma infiltrating the underlying dermis with occasional signet cells. Hematoxylin and eosin ×40.
DISCUSSION
Metastases to the umbilicus commonly referred to as Sister Joseph’s or Sister Mary Joseph’s nodule are rare but widely accepted as an ominous sign of poor prognosis, with survival averaging 2–11 months from diagnosis. [2,3]
There are three proposed mechanisms of metastasis of a neoplasm to the umbilical region – direct spread, vascular dissemination, and lymphatic propagation. [4-6] In our case, direct peritoneal spread was most likely the cause, which was confirmed by the fact of the widespread carcinomatosis of the patient.
Clinically, Sister Mary Joseph’s Nodule usually manifests as a firm, irregular nodule of about 1–1.5 cm in size but sometimes can reach 10 cm and cause pain, ulceration, and the production of various types of discharge. [7,8] The primary malignancy associated with Sister Mary Joseph’s nodule depends on the gender. In men, the first source is the stomach followed by the colon and pancreas and in women, it is the ovary followed by the endometrium, colon, and pancreas.[9-14]
Computed tomography or magnetic resonance imaging is performed to assess the spread of the tumor and its distribution. The differential diagnosis of Sister Mary Joseph’s Nodule includes primary umbilical carcinomas, benign tumors such as pyogenic granuloma, and conditions like abscesses or umbilical hernias [Table 1].[8] Microscopically, Sister Mary Joseph’s Nodule is most likely to be caused by tumors of the adenocarcinoma subtype, although squamous cell carcinomas and signet ring cell carcinomas can also cause umbilical metastases and the latter being particularly aggressive and commonly associated with gastric cancers.[11,12]
| Diagnosis | Primary Site | Clinical Features | Authors |
|---|---|---|---|
| Metastatic colon cancer | Colon | Ulcerated umbilical mass, weight loss, cachexia, liver metastases, Sister Mary Joseph’s nodule | Kamareddy, 2023[9] |
| Ovarian cancer | Ovary | Abdominal ascites with periumbilical pain. Rapid rise in CA-125, peritoneal carcinomatosis [18F] FDG PET/CT, Axial CT | Robinson et al., 2023[10] |
| Pancreatic adenocarcinoma | Pancreas | Small, erythematous, pus-discharging nodule Elevated CA19-9, contrast-enhanced CT | Dar et al., 2023[11] |
| Metastatic pancreatic adenocarcinoma | Pancreas | Abdominal pain, periumbilical nodules, liver metastases, progression during chemotherapy, Sister Mary Joseph’s nodules | Leyrat, 2021[12] |
| Carcinoma of cecum | Cecum | Abdominal pain, ascites, umbilical nodule, metastatic adenocarcinoma | Balakrishnan, 2015[13] |
| Metastatic pancreatic adenocarcinoma | Pancreas | Cachexia, elevated INR, subcutaneous nodule, weight loss, liver metastases, ascites, Sister Mary Joseph’s nodule | Menzies, 2015[14] |
CA: Carbohydrate antigen, PET: Positron emission tomography, CT: Computed tomography, [18F] FDG: 18F-Fluorodeoxyglucose, INR: International Normalized Ratio
Treatment strategies for Sister Mary Joseph’s Nodule should be tailored to each patient, considering the primary cancer, the extent of metastasis, and the resectability of the umbilical nodule.[13,14] Despite the poor prognosis associated with umbilical metastases, a combined treatment approach of surgery and chemotherapy has been shown to improve survival rates compared to single-modality treatments.[15,16] Overall, the survival rate for patients with treated umbilical metastases ranges from 5 to 11 months from diagnosis, with a very grave prognosis for primary gastric adenocarcinoma.[17-19]
CONCLUSIONS
Umbilical metastasis is rare and typically manifests in the later stages of the disease, highlighting the critical need for early detection. Thorough evaluation of any umbilical lesions is essential for the timely diagnosis of underlying cancers and to increase awareness among healthcare professionals to consider this condition in the differential diagnosis upon encountering an umbilical nodule.
Author contribution
SP: Wrote the manuscript; KK: Data collection and lab work; MJH: Data and image input; KA: Final draft and review.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The Sister Mary Joseph nodule. Br J Hosp Med (Lond). 2018;79:27-9.
- [CrossRef] [PubMed] [Google Scholar]
- Umbilical metastases: Current viewpoint. World J Surg Oncol. 2005;3:13-4.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph's nodule: A sign of internal malignancy. Ann Bras Dermatol. 2011;86:118-20.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph's nodule: Where umbilicus holds the truth! Cureus. 2021;13:13091-2.
- [CrossRef] [Google Scholar]
- Umbilical metastasis derived from early stage rectal cancer: A case report. World J Surg Oncol. 2014;12:82-3.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph's nodule as a metastasis of ovarian adenocarcinoma. Int J Dermatol. 2010;49:1045-6.
- [CrossRef] [PubMed] [Google Scholar]
- Umbilical metastasis or Sister Mary Joseph's nodule. Int J Dermatol. 1998;37:7-13.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph nodule: A brief review. Am J Gastroenterol. 2023;118:15-8.
- [CrossRef] [Google Scholar]
- Diffuse peritoneal carcinomatosis and Sister Mary Joseph nodule in ovarian carcinoma-exquisite demonstration of the peritoneal reflections on [18F]FDG PET/CT. Nuclear Med Rev. 2023;26:153-5.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph nodule-A case report with review of literature. J Res Med Sci. 2023;14:385-7.
- [Google Scholar]
- Sister Mary Joseph nodules: A case report about a rare location of skin metastasis. Case Rep Oncol. 2021;14:664-70.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph's nodule as the initial presentation of carcinoma caecum: Case report and literature review. J Gastrointest Oncol. 2015;6:102-5.
- [Google Scholar]
- Sister Mary Joseph's nodule as the sole presenting sign of gastric signet ring cell adenocarcinoma. Gastroenterol Clin Biol. 2010;34:565-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pathohistological classification systems in gastric cancer: Diagnostic relevance and prognostic value. World J Gastroenterol. 2014;20:5679-84.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph's nodule: A case of umbilical cutaneous metastasis with signet ring cell histology. Indian J Dermatol Venereol Leprol. 2009;75:503-5.
- [CrossRef] [PubMed] [Google Scholar]
- Sister Mary Joseph's nodule in endometrial cancer: A case report and review of the literature. J Cancer Res Ther. 2019;15:1408-10.
- [CrossRef] [PubMed] [Google Scholar]
- A long-term survival case of Sister Mary Joseph’s nodule caused by colon cancer and treated with a multidisciplinary approach. Nagoya J Med Sci. 2019;81:325-9.
- [Google Scholar]



