
Translate this page into:
Study of PD-L1 Expression with Association of Pathological Factors and Molecular Subtypes in Breast Carcinoma

Address for correspondence: Smita Chandra, MD, Department of Pathology, Himalayan Institute of Medical Sciences, Swami Ram Nagar, Doiwala, Dehradun, 248140, Uttarakhand, India (e-mail: smita_harish@yahoo.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background
Programmed death ligand 1 (PD-L1), expressed on cancer cells, shows varied results in the prognosis of breast cancer. This study was conducted to study the expression of PD-L1 in breast carcinoma and to correlate it with pathological, molecular classification and prognostic factors.
Materials and Methods
PD-L1 expression was correlated with tumor size, histopathological grade, necrosis, lymphovascular, perineurial invasion, lymph node metastasis, molecular classification, and survival in breast carcinoma cases.
Results
Fifty cases were included which showed statistically significant difference of PD-L1 with mean age, tumor size, histopathological grade, lymphovascular emboli, and lymph node metastasis (p < 0.05). Estrogen receptor was strongly positive in 46%, progesterone receptor in 42%, and PD-L1 in 6% of cases. No statistically significant difference between pathological tumor–node–metastasis (TNM) staging and PD-L1 expression (p = 0.354) was observed. Receptor operating characteristic curve analysis showed that at the cutoff of PD-L1 greater than 120, specificity was 56.1%, sensitivity 66.7%, negative predictive value 88.5%, and positive predictive value 25% for predicting living status.
Conclusion
PD-L1 is associated with poor prognostic factors including tumor size, histopathological grade, lymphovascular emboli, and lymph node metastasis in breast carcinoma. However, no significant association was observed between PD-L1 and pathological TNM stage or molecular subtypes of breast carcinoma. It is suggested that immunohistochemical reporting of PD-L1 should be standardized so that it is reproducible and reliable for the evaluation of breast carcinoma. Further, larger studies with extended follow-ups are recommended so that the exact role of PD-L1 as a prognostic marker in breast carcinoma could be ascertained.
Keywords
breast carcinoma
clinicopathological factors
PD-L1

Introduction
Breast carcinoma is the most common cancer worldwide (11.7%) with high mortality rate of 6.9%.[1] This condition is even worse in developing countries like India where cases present late to the hospitals with higher stage leading to increased mortality. Recently, immunological mechanisms are being studied to understand the pathogenesis of the different cancers. The cross talk between lymphocytes and tumor cells are even explored to determine the prognosis and targeted therapy against these carcinomas.[2-4] Programmed cell death 1 (PD-1) which is expressed on B and T lymphocytes, monocytes, and dendritic cells impedes immune response by giving an inhibitory signals to T cells and is also responsible for immune tolerance of self-antigens.[5,6] It binds to programmed death ligand 1 (PD-L1) which is not only present on lymphocytes and dendritic cells but also on nonlymphoid tissues.[7] PD-1 and PD-L1 interaction leads to decreased activation of T lymphocytes which although may be beneficial to prevent autoimmune reaction, but in tumor milieu, it may cause tumor cells to escape immune system and thus preventing their elimination.[8] PD-L1 has been therefore studied in various epithelial cancers including breast, lung, pancreas, etc. where its association with clinicopathological features and role in prognosis have also been explored.[9-11] However, varied results have been obtained with some studies showing high expression of PD-L1 correlates with poor prognosis, while others demonstrate that PD-L1 upregulation is associated with better survival in breast carcinoma.[12,13] The knowledge of PD-L1 in breast carcinoma may also be necessary as it may play promising role in immunotherapy.
Therefore, the present study was conducted to study the expression of PD-L1 in breast carcinoma cases and to correlate it with various pathological and prognostic factors. It was also intended to study the association of PD-L1 expression with molecular classification of breast carcinoma.
Materials and Methods
The study was conducted in pathology department of medical institution which included newly diagnosed cases of infiltrating ductal carcinoma of breast on histopathology over a period of 1 year from January to December 2019. Tru-Cut needle and core biopsies were excluded from the study. Relevant clinical details, radiological and laboratory investigations, were noted for every case. The gross and hematoxylin–eosin-stained paraffin sections were studied for tumor size, histopathological grade, in situ carcinoma, necrosis, calcification, lymphovascular emboli, perineurial invasion, and lymph node metastasis. The paraffin blocks were also stained for immunohistochemical markers including estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER 2) neu, Ki-67, and PD-L1. The ER, PR, and PD-L1 were evaluated according to H score system including both the staining intensity and percentage of stained tumor cells into H scores of 0 to 50 (negative), 51 to 100 (weakly positive), 101 to 200 (moderately positive), and 201 to 300 (strongly positive). HER 2 neu was scored 0, 1 (negative), 2 (equivocal), and 3 (positive) depending on intensity and percentage of stained cells. Ki-67 was reported less than 14 or 14% or higher cells.[14] Pathological tumor–node–metastasis (TNM) staging and molecular classification of breast carcinoma cases according to ER, PR, HER 2 neu, and Ki-67 status were done as recommended.[14,15] All the cases were followed up for at least 12 months, and their survival was noted.
All the data were compiled in Excel sheet and statistically analyzed using Statistical Package for Social Sciences version 23 (Chicago, United States). The results were expressed as number, percentages, mean ± standard deviation, and median. Association between categorical variables was done using Student's t-test and Pearson's correlation coefficient. The p-value less than 0.05 was considered significant. The diagnostic performance of PD-L1 in predicting living status of cases was assessed by performing receptor operating characteristic (ROC) curve analysis.
The study was approved by the Institutional Review Board with reference number SRHU/Reg/Int/2019-55 dated February 5, 2019.
Results
The study included 50 cases of infiltrating ductal carcinoma of breast with 48 cases diagnosed in females, while 2 cases in males. The mean age of cases was 53.8 ± 15.13 years, median of 56 years, and age range of 27 to 81 years. The maximum number of cases were in the age group of 31 to 40 and 61 to 70 years (26% each), and only one case had positive family history of breast carcinoma. Most of the cases presented with breast lump of less than 6 months duration (62% cases), axillary lymphadenopathy (78%), and skin excoriation (36%). Mammography was reported as Breast Imaging Reporting and Data System categories IV and V in 71.42% of cases. Fine needle aspiration cytology was done in 43 cases and out of which ductal carcinoma or atypical cells suggestive of carcinoma was diagnosed in 95.3% of cases. ►Table 1 shows the gross and histopathological findings in breast carcinoma cases. ►Table 2 shows the immunohistochemical expression of molecular markers in the cases. H score for ER was strongly positive in 46% of cases, PR in 42%, HER 2 neu negative score in 92% of cases, high Ki-67 proliferation index in 84% of cases, and 50% of cases were moderately positive for PD-L1 expression (►Fig. 1). The molecular classification of cases was luminal A (11 cases), luminal B (24 cases), Her 2 neu positive (4 cases), and triple negative (11 cases). Pathological TNM staging showed that maximum number of cases were of pT2N0Mx (30%) followed by pT2N1aMx stage (20%). Additionally, although skin excoriation was seen in 36% of cases grossly but microscopically ulceration was seen only in four cases, and therefore, only 8% of cases were included in T4 stage. On follow-up for 12 months, 82% of cases were alive, and 14% showed recurrent carcinoma. ►Table 3 shows the association of PD-L1 expression with histopathological and prognostic factors in the breast carcinoma cases. There was statistically significant difference in PD-L1 expression with mean age, tumor size, histopathological grade, lymphovascular emboli, and lymph node metastasis. It was also observed that there was no statistically significant difference between pathological TNM staging and PD-L1 expression (p = 0.354). ►Table 4 shows the association of PD-L1 expression with molecular subtypes of breast carcinoma cases. There was statistically significant association of PD-L1 with ER positivity, HER 2 neu negativity, and high Ki-67 proliferative index (< 14%). Luminal A and triple-negative carcinoma with positive PD-L1 expression constituted 22.5%, luminal B 45%, and HER 2 neu 10% of total PD-L1 positive cases. ROC curve analysis showed that at the cutoff of PD-L1 H score of over 120 for predicting living status of cases, specificity was 56.1%, sensitivity was 66.7%, negative predictive value of 88.5%, and positive predictive value of 25% with diagnostic odds ratio of 2.56 (►Fig. 2).

- (A, B) Grade 0 PD-L1 expression in breast carcinoma (IHC PD-L1, ×4 and ×40). (C, D) Grade 1 PD-L1 expression in breast carcinoma (IHC PD-L1, ×4 and ×40). (E, F) Grade 2 PD-L1 expression in breast carcinoma (IHC PD-L1, ×4 and ×40). (G, H) Grade 2 PD-L1 expression in breast carcinoma (IHC PD-L1, ×4 and ×40). IHC, immunohistochemistry; PD-L1, programmed death ligand 1.
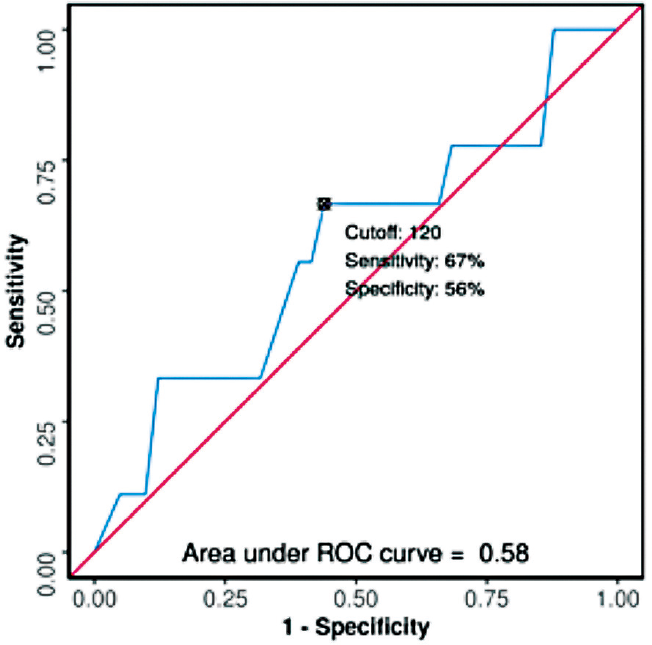
- Receptor operating characteristic (ROC) curve analysis showing diagnostic performance of programmed death ligand 1 score in predicting living status of cases.
| Pathological characteristics | Number of cases (%) |
|---|---|
| Laterality | |
| Right breast | 29 (58%) |
| Left breast | 20 (40%) |
| Bilateral | 1 (2%) |
| Tumor size | |
| < 2 cm | 2 (4%) |
| 2–5 cm | 32 (64%) |
| > 5 cm | 16 (32%) |
| Modified Richardson–Bloom score | |
| 3–5 | 0 |
| 6–7 | 37 (74%) |
| 8–9 | 13 (26%) |
| Histopathological grade | |
| Grade I | 0 |
| Grade II | 37 (74%) |
| Grade III | 13 (26%) |
| Intratumoral DCIS (> 25%) | 15 (30%) |
| Extratumoral DCIS (> 10%) | 3 (6%) |
| Calcification | 3 (6%) |
| Lymphovascular emboli | 41 (82%) |
| Perineural invasion | 9 (18%) |
| Uninvolved breast | |
| Fibrocystic breast disease | 45 (90%) |
| Chronic mastitis | 5 (10%) |
| Lymph node metastasis | 30 (60%) |
| Pathological TNM stage grouping | |
| Stage I | 1 (2%) |
| Stage IIA | 16 (32%) |
| Stage IIB | 11 (22%) |
| Stage IIIA | 10 (20%) |
| Stage IIIB | 5 (10%) |
| Stage IIIC | 3 (6%) |
| Stage IV | 4 (8%) |
Abbreviation: DCIS, ductal carcinoma in situ.
| Molecular marker | Interpretation | Number of cases (%) |
|---|---|---|
| ER H score | ||
| 0–50 (Grade 0) | Negative | 15 (30%) |
| 51–100 (Grade 1) | Weakly positive | 2 (4%) |
| 101–200 (Grade 2) | Moderately positive | 10 (20%) |
| 201–300 (Grade 3) | Strongly positive | 23 (46%) |
| PR H score | ||
| 0–50 (Grade 0) | Negative | 20 (40%) |
| 51–100 (Grade 1) | Weakly positive | 1 (2%) |
| 101–200 (Grade 2) | Moderately positive | 8 (16%) |
| 201–300 (Grade 3) | Strongly positive | 21 (42%) |
| HER 2 neu score | ||
| 0–1 | Negative | 46 (92%) |
| 2 | Equivocal | 1 (2%) |
| 3 | Positive | 3 (6%) |
| Ki-67 proliferation index | ||
| < 14% | Low proliferative index | 8 (16%) |
| > 14% | High proliferative index | 42 (84%) |
| PD-L1 H score | ||
| 0–50 (Grade 0) | Negative | 10 (20%) |
| 51–100 (Grade 1) | Weakly positive | 12 (24%) |
| 101–200 (Grade 2) | Moderately positive | 25 (50%) |
| 201–300 (Grade 3) | Strongly positive | 3 (6%) |
Abbreviations: ER, estrogen receptor; HER 2, human epidermal growth factor receptor 2; PD-L1, programmed death ligand 1; PR, progesterone receptor.
| Characteristics | Negative PD-L1 expression | Positive PD-L1 expression | p-Value |
|---|---|---|---|
| Mean age | |||
| 53.8 y | 9 | 41 | 0.04 |
| Tumor size | |||
| 2–5 cm | 8 | 24 | 0.01 |
| > 5 cm | 2 | 11 | |
| Histopathological grade | |||
| Grade I | 0 | 0 | 0.03 |
| Grade II | 8 | 29 | |
| Grade III | 2 | 11 | |
| Intratumoral DCIS | |||
| < 25% | 6 | 29 | 0.48 |
| > 25% | 4 | 11 | |
| Extratumoral DCIS | 0 | 3 | 0.39 |
| Microcalcification | 0 | 3 | 1 |
| Lymphovascular emboli | 10 | 31 | 0.05 |
| Perineurial invasion | 1 | 8 | 0.81 |
| Lymph node metastasis | 9 | 21 | 0.02 |
| Living status (after 12 mo) | |||
| Alive | 8 | 33 | 0.62 |
| Dead | 2 | 7 | |
| Recurrent status of tumor (until 12 mo) | |||
| Recurrent | 2 | 6 | 0.40 |
| Not recurrent | 0 | 2 | |
Abbreviations: DCIS, ductal carcinoma in situ; PD-L1, programmed death ligand 1.
| Molecular expression | Negative PD-L1 expression | Positive PD-L1 expression | p-Value |
|---|---|---|---|
| ER | |||
| Negative | 2 | 13 | 0.04 |
| Positive | 8 | 27 | |
| PR | |||
| Negative | 4 | 16 | 0.77 |
| Positive | 6 | 24 | |
| HER 2 neu | |||
| Negative | 8 | 38 | 0.05 |
| Equivocal | 0 | 1 | |
| Positive | 0 | 3 | |
| Ki-67 index | |||
| < 14% (low proliferative index) | 1 | 7 | 0.04 |
| > 14% (high proliferative index) | 9 | 33 | |
| Molecular classification | |||
| Luminal A | 2 | 9 | 0.34 |
| Luminal B | 6 | 18 | |
| HER 2 neu positive | 0 | 4 | |
| Triple negative | 2 | 9 | |
Abbreviations: ER, estrogen receptor; HER 2, human epidermal growth factor receptor 2; PD-L1, programmed death ligand 1; PR, progesterone receptor.
Discussion
PD-L1 or CD274, a ligand of PD-1 is upregulated on tumor cells by oncogenic and inflammatory signals in tumor microenvironment and thus may be predictive marker of PD-1/PD-L1 pathway inhibition.[16,17] PD-L1 has been studied in various carcinoma including lung carcinoma, melanoma, and head and neck carcinoma with its role in immunotherapy against these malignancies.[18,19] Although literature search shows studies related to the role of PD-L1 as prognostic biomarker in breast carcinoma, the results are divergent.[20] Few studies have observed that expression of PD-L1 is associated with poor prognosis in breast carcinoma, while others concluded that its upregulation is associated with better prognosis.[21,22] The present study observed that higher mean age showed statistical significant correlation with positive expression of PD-L1 which is in contrast to study done by Mori et al who observed significant association of negative PD-L1 with higher mean age (61.8 years).[23] This may be because Mori et al have studied PD-L1 in combination with tumor-infiltrating lymphocytes (TILs) in only triple-negative carcinoma, while we studied all the subtypes of breast carcinoma. In triple-negative carcinoma, the present study observed no statistically significant difference between PD-L1 expression and age which was similar to as observed by Botti et al.[21] Tumor size is considered to be an important prognostic factor in breast carcinoma, and it was observed in our study that larger tumor size was associated with increased expression of PD-L1. Muenst et al observed an interesting finding on flow cytometry of breast carcinoma cases that as the tumor size increases, PD-L1 production increases from TIL to cancer cells to evade antitumor immune response.[22] Another important observation of our study was statistically significant association of PD-L1expression with histopathological grade, lymphovascular emboli, and lymph node metastasis. This suggests that PD-L1 activation pathway may be responsible for spread and proliferation of tumor cells by escaping the tumor immunological mechanism. Although few studies have observed similar findings for histopathological grade, lymphovascular emboli and lymph node metastasis showed no significant association with PD-L1 expression in these studies.[24,25] Previously, studies have evaluated PD-L1 both on tumor cells and TIL with consistent findings, but the present study evaluated PD-L1 only on tumor cells.[21,24] It was also observed in the present study that PD-L1 expression showed statistical significant difference with ER positivity, HER 2 neu negativity and high Ki-67 proliferative index (< 14%). Stovgaard et al reviewed the expression of PD-L1 in subtypes of breast cancer and observed PD-L1 expression ranging from 2.3 to 37% for luminal A, 9 to 46% for luminal B, 0 to 33% for HER 2 neu positive, and 5 to 80% for triple-negative breast cancer.[8] Our study also observed similar findings for PD-L1 expression in different molecular subtypes with luminal B constituting maximum of PD-L1 positive cases (40%). The PD-L1 expression has been reported to be associated with better prognosis in triple-negative breast cancer patients in diabetics and with poor prognosis in cases with decreased TILs.[21,23] However, no significant association was observed between PD-L1 and different molecular subtypes of breast carcinoma in our study. This is because each subtype constituted lesser number of cases which may have led to statistically invalid results. Recently, Yazdanpanah et al have observed more PD-L1 expression in triple-negative cancer patients.[26]
The variation of PD-L1 expression in different studies may also be related to lack of uniform system of evaluating PD-L1. Guo et al observed differences in PD-L1 expression in association with clinicopathological factors when scored in tumor cells, tumor-infiltrating immune cells, or combination of them.[9] In addition, the different cutoffs for PD-L1 positive cells ranging from 1 to 50%, staining intensity and observing membranous stain, cytoplasmic or both may also play an important role in PD-L1 immunoexpression reporting. This may affect the assessment of PD-L1 with clinicopathological and prognosis of breast carcinoma. Therefore, it is suggested that PD-L1 reporting system with fixed cutoff, type of cells evaluated (tumor cells/immune cells or both), and staining intensity should be standardized for defining its prognostic role.
The present study had certain limitations which included lesser number of cases with shorter period of follow-up. This may be responsible for unequal distribution of cases in certain subgroups leading to skewed statistical analysis. In addition, tumor heterogeneity may also lead to improper assessment of PD-L1 in prognosis of breast cancer patients.
Conclusion
PD-L1 is associated with poor prognostic factors including tumor size, histopathological grade, lymphovascular emboli, and lymph node metastasis in breast carcinoma. However, no significant association was observed between PD-L1 and pathological TNM stage or molecular subtypes of breast carcinoma. It is suggested that immunohistochemical reporting of PD-L1 should be standardized so that it is reproducible and reliable for evaluation of breast carcinoma. In addition, further larger studies with extended follow-up are recommended so that exact role of PD-L1 as prognostic marker in breast carcinoma could be ascertained. This implication of PD-L1 may also play an important role in novel targeted immunotherapy against breast carcinoma.
Authors' Contribution
A.G. and S.C. conceptualized the study. A.G. helped in data curation and original drafting. Formal analysis was done by A.G., S.C., and N.C. and methodology by A.G., S.C., N.C.; and A.A., S.C., and N.C. supervised the study. S.C., N.C., and A.A. contributed to writing review and editing. All authors approved the final manuscript.
Conflict of Interest
None declared.
Funding
None.
References
- Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(03):209-249.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic impact of immune microenvironment in laryngeal and pharyngeal squamous cell carcinoma: Immune cell subtypes, immuno-suppressive pathways and clinicopathologic characteristics. Oncotarget. 2017;8(12):19310-19322.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction role of tumor infiltrating lymphocytes in triple negative breast cancer patients received the neoadjuvant chemotherapy: a meta analysis. Chemo Open Access. 2017;6:245.
- [Google Scholar]
- Evaluation of tumor infiltrating lymphocytes in breast carcinoma and their correlation with molecular subtypes, tumor grade and stage. Breast Dis. 2020;39(02):61-69.
- [CrossRef] [PubMed] [Google Scholar]
- Intrinsic and extrinsic control of peripheral T cell tolerance by costimulatory molecules of the CD28/B7 family. Immunol Rev. 2011;241(01):180-205.
- [CrossRef] [PubMed] [Google Scholar]
- PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol. 2008;26:677-704.
- [CrossRef] [PubMed] [Google Scholar]
- Immune inhibitory molecules LAG-3 and PD-1 synergistically regulate T-cell function to promote tumoral immune escape. Cancer Res. 2012;72(04):917-927.
- [CrossRef] [PubMed] [Google Scholar]
- PD-L1 expression in breast cancer: expression in subtypes and prognostic significance: a systematic review. Breast Cancer Res Treat. 2019;174(03):571-584.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of three scoring methods using the FDA-approved 22C3 immunohistochemistry assay to evaluate PD-L1 expression in breast cancer and their association with clinicopathologic factors. Breast Cancer Res. 2020;22(01):69.
- [CrossRef] [PubMed] [Google Scholar]
- Role of PD-L1 expression in non small cell lung cancer and their prognostic significance according to their clinicopathological factors and diagnostic markers. Int J Mol Sci. 2019;20(04):824.
- [CrossRef] [PubMed] [Google Scholar]
- PD-L1 expression in pancreatic cancer. J Natl Cancer Inst. 2017;109(06):djw304.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic value of PD-L1 in breast cancer: a meta analysis. Breast J. 2017;23(04):436-443.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget. 2015;6(07):5449-5464.
- [CrossRef] [PubMed] [Google Scholar]
- Immunohistochemical surrogates for molecular classification of breast carcinoma: a 2015 update. Arch Pathol Lab Med. 2016;140(08):806-814.
- [CrossRef] [PubMed] [Google Scholar]
- The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(02):93-99.
- [CrossRef] [PubMed] [Google Scholar]
- Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell. 2015;27(04):450-461.
- [CrossRef] [PubMed] [Google Scholar]
- Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature. 2014;515(7528):563-567.
- [CrossRef] [PubMed] [Google Scholar]
- Development of a programmed cell death ligand-1 immunohistochemical assay validated for analysis of non-small cell lung cancer and head and neck squamous cell carcinoma. Diagn Pathol. 2016;11(01):95.
- [CrossRef] [PubMed] [Google Scholar]
- Development of a diagnostic programmed cell death -ligand 1 immunohistochemistry assay for nivolumab therapy in melanoma. Appl Immunohistochem Mol Morphol. 2018;26(01):6-12.
- [CrossRef] [PubMed] [Google Scholar]
- Prognosis of PD-L1 in human breast cancer: protocol for a systematic review and meta-analysis. Syst Rev. 2020;9(01):66.
- [CrossRef] [PubMed] [Google Scholar]
- Programmed death ligand 1 (PD-L1) tumor expression is associated with a better prognosis and diabetic disease in triple negative breast cancer patients. Int J Mol Sci. 2017;18(02):459.
- [CrossRef] [PubMed] [Google Scholar]
- Expression of programmed death ligand 1 (PD-L1) is associated with poor prognosis in human breast cancer. Breast Cancer Res Treat. 2014;146(01):15-24.
- [CrossRef] [PubMed] [Google Scholar]
- The combination of PD-L1 expression and decreased tumor-infiltrating lymphocytes is associated with a poor prognosis in triple-negative breast cancer. Oncotarget. 2017;8(09):15584-15592.
- [CrossRef] [PubMed] [Google Scholar]
- PD-L1 expression and tumor infiltrating lymphocytes in breast cancer: clinicopathological analysis in women younger than 40 years old. In Vivo. 2020;34(02):639-647.
- [CrossRef] [PubMed] [Google Scholar]
- The B7-H1 (PD-L1) T lymphocyte-inhibitory molecule is expressed in breast cancer patients with infiltrating ductal carcinoma: correlation with important high-risk prognostic factors. Neoplasia. 2006;8(03):190-198.
- [CrossRef] [PubMed] [Google Scholar]
- PD-L1 expression in tumor lesions and soluble PD-L1 serum levels in patients with breast cancer: TNBC versus TPBC. Breast Dis. 2021;40(01):43-50.
- [CrossRef] [PubMed] [Google Scholar]



