
Translate this page into:
Trends of human immunodeficiency virus prevalence and mother-to-child transmission at a tertiary care center in North India
 , Parakriti Gupta1, Dipanshu Vasesi1, Poonam Goel2, Bharti Goel2, Alka Raheja1, Sunaina Suman1, Varsha Gupta1,
, Parakriti Gupta1, Dipanshu Vasesi1, Poonam Goel2, Bharti Goel2, Alka Raheja1, Sunaina Suman1, Varsha Gupta1,
*Corresponding author: Varsha Gupta, Professor and Head, Department of Microbiology, Government Medical College and Hospital, Chandigarh, India. varshagupta_99@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Singhal L, Gupta P, Vasesi D, Goel P, Goel B, Raheja A, et al. Trends of human immunodeficiency virus prevalence and mother-to-child transmission at a tertiary care center in North India. J Lab Physicians. doi: 10.25259/JLP_95_2024
Abstract
Objectives
Human immunodeficiency virus (HIV) is one of the most dreadful infections worldwide. Although the most common mode of transmission is unprotected sex in India, the threat of parent-to-child transmission (PTCT) serves as a major roadblock in curbing infection. The study was conducted to decipher trends of PTCT at tertiary care centers in North India.
Materials and Methods
This was a prospective study conducted over 8 years, wherein all pregnant women (19,996) attending antenatal clinics were included in the study. Testing was done free of cost, following a three-test protocol of the National Acquired Immunodeficiency Syndrome control organization. All newborns to HIV-positive females were tested and followed up to 18 months. Dry blood samples (DBS) collected at 1.5, 6, 12, and 18 months were tested using polymerase chain reaction (PCR). We also divulged the trend of HIV for all individuals attending integrated counseling and testing centers (ICTC).
Statistical analysis
Descriptive analysis was performed using Microsoft Excel and interpreted as percentages.
Results
A total of 36 (0.18%) reported HIV-positive and were counseled for implications on their health risk of sexual and vertical transmission. The yearly trend divulged decreasing HIV positivity, from 0.14% in 2014– 2015 to zero in 2021–2022, ranging from 0.11–0.22%. A similar trend was noted among ICTC, with 1.26% positivity (2020) and 2.23% in 2021, with overall positivity of 1.49%. All DBS samples reported negative for HIV deoxyribonucleic acid PCR.
Conclusions
The study underlines the role of monitoring, diagnostic, and counseling strategies in curbing transmission. Although the trend of HIV is declining, there is a constant need to screen all antenatal females to prevent vertical transmission.
Keywords
Parent-to-child transmission
Human immunodeficiency virus
Trend
Integrated counseling and testing centers
Prevention of parent-to-child transmission

INTRODUCTION
Human immunodeficiency virus (HIV) is one of the major causes of global morbidity and mortality, with ~38.4 million people living with HIV-acquired immunodeficiency syndrome (AIDS) and 650,000 deaths reported in 2021.[1] The main mode of transmission is unprotected sex in adults, followed by intravenous drug abuse, blood transfusion, and others. However, mother-to-child transmission (MTCT), also termed vertical transmission or parent-to-child transmission (PTCT), is the only mode of HIV acquisition in infants. Approximately 4% of all HIV infections are acquired through PTCT,[2,3] of which ~75% of the infections are acquired during labor, followed by antenatal transmission, that is, later stages of pregnancy in 25–30% of the cases and breastfeeding. Furthermore, the rate of MTCT is known to vary among breastfeeding and non-breastfeeding nations, with incidence being higher in the former.[4] National AIDS Control Organization (NACO) has anticipated ~22,000 pregnant females to be HIV-infected, and of these infected females, ~20,93,000 pregnant females were administered anti-retroviral therapy (ART) under Prevention of PTCT (PPTCT) of HIV/AIDS in 2020.[5] Due to the potential threat of PTCT and pediatric HIV, National AIDS and STD Control Program (NACP), the Government of India with NACO initiated the PPTCT program in 2002.[6] To facilitate accessibility to the destitute, multiple integrated counseling and testing centers (ICTCs) have been set up to achieve “Elimination of Mother to Child Transmission.” PPTCT aims to provide free testing and counseling services, along with the life-long provision of ART to HIV-positive females and anti-retroviral prophylaxis to infants.[6,7] The present study was conducted to decipher the trends of PTCT from our tertiary care center, with follow-up testing of all newborns up to 18 months.
MATERIALS AND METHODS
Inclusion criteria
All the pregnant women who attended the antenatal clinic (ANC) during the study period [8 years (2014–2022)] were included in the study. All the newborns to HIV-positive females were included for follow-up up to 18 months of age.
Testing procedure and interpretation
This was a prospective study conducted over 8 years (2014– 2022) at the PPTCT center of our tertiary care hospital. A total of 19,996 pregnant women attended ANC during the study period. Pre-test and post-test counseling and HIV testing of one and all were performed, according to the NACO guidelines, after obtaining their informed written consent. Testing was done free of cost in ICTCs for all using NACO-recommended enzyme-linked immunosorbent assay kits.[7] Patients who tested negative by one test were considered HIV-negative after screening. Testing is done using the three-test protocol for confirmation. If the test was found to be reactive, the patients were linked to ART centers and HIV care continuum services for further course of management and advised institutional delivery.
All the newborns to HIV-positive females were followed up to 18 months of age. Diagnosis in infants and children <18 months with perinatal and postnatal HIV exposure was established using nucleic acid amplification tests to detect viral nucleic acid. Antibody tests and antigen/antibody detection tests were not employed;[7,8] However, on requisition, antibody testing was performed in a few, in the advent of non-availability of nucleic acid amplification tests (2 in 2014–2015, 1 in 2015–2016, 4 in 2016–2017, 4 in 2017– 2018, 6 in 2018–2019, 7 in 2019–2020, 13 in 2020–2021, and 1 in 2021–2022). Dry blood samples (DBS) of infants were collected at 1.5 months, 6 months, 12 months, and 18 months of age and sent to the reference laboratory at All India Institute of Medical Sciences (AIIMS), New Delhi, for polymerase chain reaction (PCR).[9] Besides the HIV positivity among pregnant females and infants, we also divulged the trend of HIV positivity among all the individuals attending ICTC at our tertiary care center.
Statistical analysis
Descriptive analysis and graphical analysis were performed using Microsoft Excel and interpreted as percentages.
RESULTS
A total of 19,996 pregnant females attended ANC during the study period, all of whom were pre-counseled, and HIV testing was performed after obtaining informed written consent. Of these, 36 (0.18%) were reported HIV-positive at the PPTCT center of our institute. HIV-positive females were assisted by an ICTC counselor to cope with the result and to comprehend the implications of HIV positivity on their health and the risk of vertical transmission. These females were further linked to ART centers for confirmative testing using the three-test protocol of NACO. Children, spouses, or partners of HIV-positive females were also tested for HIV. Follow-up counseling was also provided to ensure safe behavior to prevent the transmission to others.
During the study period, 76 deliveries of HIV-positive females were conducted [60 (78.94%) were normal vaginal delivery, and 24 (31.57%) were cesarean sections], of which 25 (32.9%) were ANC-booked patients, while 51 (67.1%) patients were unbooked, whose HIV testing was done at the time of delivery. Trends over the years divulged a decrease in HIV positivity among pregnant females, with 0.14% in 2014– 2015 to zero in 2021–2022, ranging from 0.11% to 0.22% over all these years [Figure 1]. A similar trend was noted among all the individuals attending ICTC of our institute, with 1.26% positivity in 2020 and 2.23% in 2021. Of all the patients who tested positive, 62.37% were male, while 37.65 were female (non-pregnant). Overall, HIV positivity at our center was noted to be 1.49% from 2015 to 2022 [Figure 2].
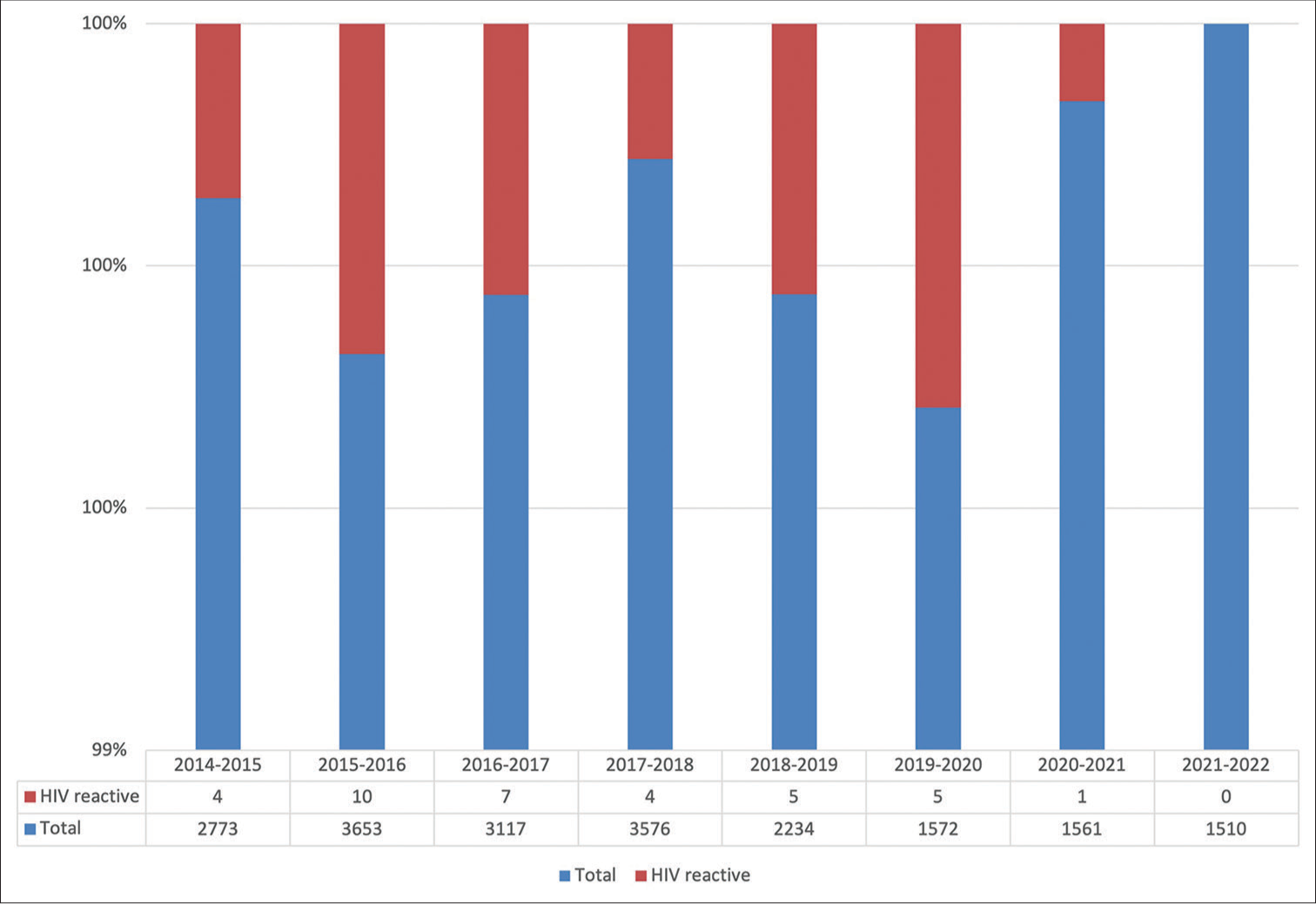
- Yearly trend of human immunodeficiency virus-positivity among pregnant females at our center.
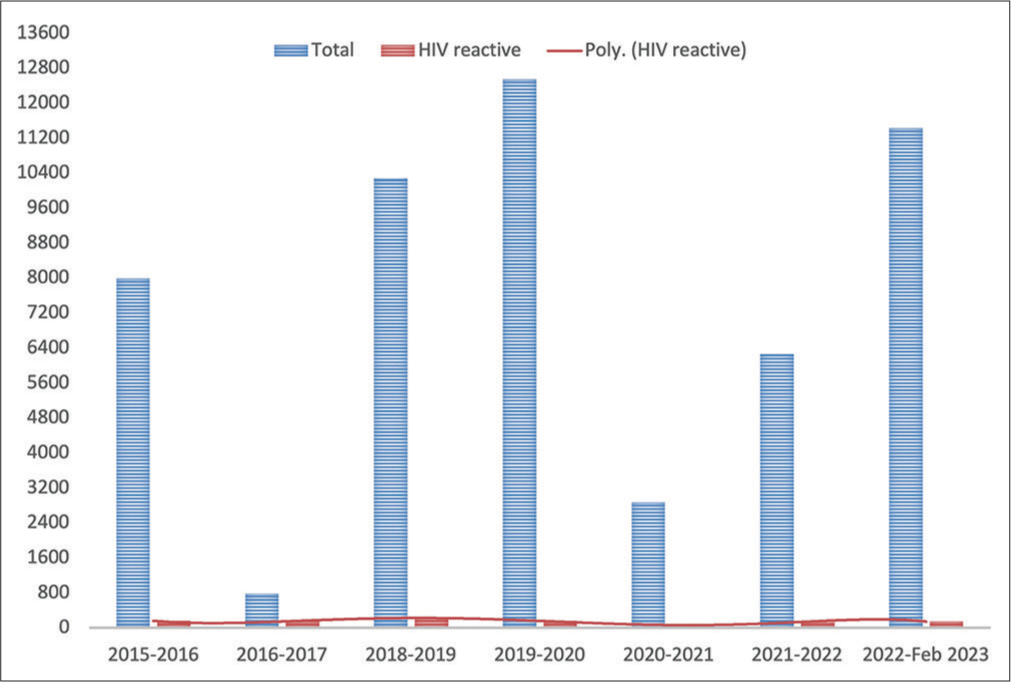
- Yearly trend of human immunodeficiency virus-positivity among all individuals presenting at the integrated counseling and testing center of our center. X-axis shows the years and Y-axis shows the number of cases.
Of all the newborns (HIV-positive females), three succumbed during labor itself, and the rest were healthy at the time of delivery. All newborns were administered nevirapine syrup, as per the NACO guidelines. Cotrimoxazole was also administered to all the infants after 6 weeks of birth to prevent Pneumocystis jiroveci pneumonia, toxoplasmosis, and various bacterial diseases. Mothers were advised to continue breastfeeding the infant till 6 months of age. Follow-up of all newborns was done at 1.5 months, 6 months, 12 months, and 18 months for repeat HIV testing, as per the NACO guidelines. At a 6-week follow-up, 93 DBS samples were collected, and all were reported negative for HIV deoxyribonucleic acid PCR test by AIIMS, New Delhi. After 18 months of follow-up, all newborns again reported HIV-negative.
DISCUSSION
The present study revealed successful prevention of PTCT in all of our patients during the study period. The same has been possible owing to the widespread awareness and vision of the NACP-V/National Strategic Plan for HIV/AIDS and sexually transmitted infections (2017–2024) to achieve zero new infections, zero AIDS-related deaths, and zero discrimination rate.[10] More than 21,000 ICTCs have been working to ensure the success of these goals and offer free HIV-related counseling and care to pregnant females. Reliable, confidential, and accurate testing services are provided to all pregnant females at these centers to ensure compliance and assist in coping with the situation. In the present study, both the groups, females who knew about their HIV status during ANC visits (32.9%) and who were tested at the time of labor (67.1%), were advised to take ART, initiate breastfeeding within one hour of delivery, continue exclusive breastfeeding, and adhere to breastfeeding for 6–12 months.[7,11] This is in contrast to the literature from other countries.[12-14] Despite the acceptable outcome in pregnant females who decide to breastfeed in industrialized countries, the experts advise against the same in those regions, raising the dilemma for the clinicians to advise the patients.[15-18]
A decreasing trend was noticed amongst pregnant females over the study period, with an overall seroprevalence of 0.18% (0.11– 0.22%) at our tertiary care center. A similar trend with 1.49% positivity (1.26–2.23%) was noted among all the individuals attending the ICTC of our center. This is in concordance with the Chandigarh State AIDS Control Society, with 0.19% prevalence among the adult population in Chandigarh. Data over the recent years issued by NACO have also revealed -a 42.7% change in new infections per year.[19] MTCT rate has noted a decline from 40.67 to 24.25% from 2010 to 2021, with PMTCT need of 20.61, the highest need in Maharashtra (2.67%), Bihar (2.45%), and U.P. (2.19%). The current PMTCT need for Chandigarh is 0.02,[19] which is encouraging compared to the figures reported in the past.[20,21] The decline reported in the present study is in congruence with the available literature.[22,23] A decline up to the level of 0.22% has also been reported.[24] A 10-year trend of seroprevalence revealing 0.44% has been reported from Maharashtra,[25] in contrast to the seroprevalence rate of 1.38% reported from Maharashtra in 2011.[26] However, the contrasting figures of 1.03% seroprevalence of HIV in antenatal females were reported from Punjab.[27]
Although a steady decline has been noted in the study, it is worthwhile to stringently monitor the seroprevalence at ICTCs and antenatal clinics. Joshi et al. have suggested the utility of second HIV testing at 36 weeks of gestation in women who initially tested negative for the infection and detected 0.043% new HIV infections, proving it to be of substantial advantage and cost-effective.[28] This double-testing strategy can be employed at centers with higher seroprevalence of HIV in the population to diagnose and appropriately monitor the progression of infection.
CONCLUSIONS
The study highlights the role of effective diagnostic and counseling strategies in delimiting the transmission and monitoring of infection under the four-pronged approach of PPTCT. PPTCT, with NACO V goals, has reached a creditable spot in the reduction of HIV with the provision of free ART and services to HIV-infected females and is heading steadily to reach the 95-95-95 goal and achieve 90% reductions by 2030. Although the trend is declining, there is a thriving need for constant screening of antenatal females to prevent transmission to the newborn. Diagnosis and counseling are imperative to ensure the mental health of pregnant females and monitor adherence to treatment regimens. Besides diagnosis, there is a constant requisite to continue stringent surveillance to identify and curb any shortcomings at the earliest, to safeguard the declining trend.
Author contribution
VG, LG: Conceptualization of the study; PG, DV: Material preparation, data collection and analysis; PGo, BG: Sample collection and management; AR: Sample testing; SS: Counselling; PG, DV: Writing the first draft of the manuscript; LG, VG: Approval of the manuscript. All authors read and approved the final manuscript.
Ethical approval
The study was approved by Institutional Ethical Committee vide approval number GMCH/IEC/691/2022/64, dated 14th May 2022.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids [Last accessed on 2024 Jan 21]
- Mother-to-child HIV transmission and its correlates in India: Systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020;20:509.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric HIV in India: Current scenario and the way forward. Indian J Public Health. 2017;61:124-30.
- [CrossRef] [PubMed] [Google Scholar]
- Prevention of mother-to-child HIV transmission in resource-poor countries: Translating research into policy and practice. JAMA. 2000;283:1175-82.
- [CrossRef] [PubMed] [Google Scholar]
- Technical report: India HIV estimates. Available from: https://www.naco.gov.in/documents/statistics [Last accessed on 2024 Jan 21]
- [Google Scholar]
- Available from: https://naco.gov.in/elimination-vertical-transmission-hiv-syphilis [Last accessed on 2024 Jan 21]
- Available from: https://naco.gov.in/sites/default/files/national_guidelines_for_hiv_care_and_treatment_2021.pdf [Last accessed on 2024 Jan 21]
- Diagnosis of human immunodeficiency virus infection. Clin Microbiol Rev. 2018;32:e00064-18.
- [CrossRef] [PubMed] [Google Scholar]
- Dried blood spot test for HIV exposed infants and children and their anti-retro viral treatment status in selected hospitals in Ethiopia. Ethiop J Health Sci. 2016;26:17-24.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://naco.gov.in/sites/default/files/Paving%20the%20Way%20for%20an%20AIDS%2015122017.pdf [Last accessed on 2024 Jan 21]
- Available from: https://www.cdc.gov/breastfeeding/breastfeeding-special-circumstances/maternal-or-infant-illnesses/hiv.html [Last accessed on 2024 Jan 21]
- Human immunodeficiency virus infection in Saudi Arabian children: Transmission, clinical manifestations and outcome. Ann Saudi Med. 2006;26:92-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of breastfeeding and formula feeding on transmission of HIV-1: A randomized clinical trial. JAMA. 2000;283:1167-74.
- [CrossRef] [PubMed] [Google Scholar]
- Mother-to-child transmission of HIV: Experience at a referral hospital in Saudi Arabia. Ann Saudi Med. 2010;30:15-7.
- [CrossRef] [PubMed] [Google Scholar]
- Infant feeding and transmission of human immunodeficiency virus in the United States. Pediatrics. 2013;131:391-6.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://clinicalinfo.hiv.gov/en/guidelines/perinatal/infant-feeding-individuals-hiv-united-states [Last accessed on 2024 Jan 21]
- Available from: https://hivinfo.nih.gov/node/2903 [Last accessed on 2024 Jan 21]
- Pediatric European Network for Treatment of AIDS (PENTA) guidelines for treatment of pediatric HIV-1 infection 2015: Optimizing health in preparation for adult life. HIV Med. 2018;19:e1-42.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://naco.gov.in/sites/default/files/india%20hiv%20estimates%202021%20_fact%20sheets__final_shared_24_08_2022.pdf [Last accessed on 2024 Jan 21]
- Seroprevalence of HIV in pregnant women in North India: A tertiary care hospital based study. BMC Infect Dis. 2007;7:133.
- [CrossRef] [PubMed] [Google Scholar]
- Seropositivity of hepatitis B, hepatitis C, syphilis, and HIV in antenatal women in India. J Infect Dev Ctries. 2013;7:832-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of HIV infection in pregnant women in Mumbai, India: Experience from 1993-2004 and 2008. J Family Med Prim Care. 2017;6:240-2.
- [CrossRef] [PubMed] [Google Scholar]
- Trends of HIV prevalence in rural South India. J Family Med Prim Care. 2019;8:669-72.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of HIV among rural pregnant women attending antenatal clinics at Pravara Rural Hospital, Loni, Maharashtra, India. Int J Health Allied Sci. 2012;1:13-5.
- [CrossRef] [Google Scholar]
- Ten years trend of HIV seroprevalence among Indian Pregnant women attending antenatal clinic at a tertiary hospital in Dhule, Maharashtra, India. IJRCOG. 2016;5:1514-9.
- [CrossRef] [Google Scholar]
- HIV seroprevalence among the pregnant population and utilisation of integrated counselling and training center facilities at a teaching hospital in Rural Maharashtra. Australas Med J. 2011;4:566-70.
- [CrossRef] [PubMed] [Google Scholar]
- Seroprevalence of human immunodeficiency virus among antenatal women in one of the institute of Northern India. J Clin Diagn Res. 2016;10:QC08-9.
- [CrossRef] [PubMed] [Google Scholar]
- Cost-effectiveness of a repeat HIV test in pregnancy in India. BMJ Open. 2015;5:e006718.
- [CrossRef] [PubMed] [Google Scholar]



