
Translate this page into:
Liver and mesenteric hydatid cyst in a child
*Corresponding author: Nitin James Peters, MS, Mch (Pediatric Surgery), Department of Paediatric Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh 160012, India. nitinjamespeters@yahoo.com; p.nitinjames@pgimer.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Vutukuru S, Peters NJ, Mewara A, Kaur S, Samujh R. Liver and mesenteric hydatid cyst in a child. J Lab Physicians. 2024;16:207-9. doi: 10.1055/s-0043-1774379
Abstract
Hydatid disease, though endemic in the sub-Himalayan region of the subcontinent, is relatively rare in the pediatric age group. The simultaneous existence of hydatid in two or more organs is very rare, seen only in 5 to 13% of patients. We report an 11-year-old patient, who presented with painless progressive abdomen distension over 6 months. Imaging studies revealed a large cystic lesion occupying majority of the abdomen. The patient was diagnosed to have a hydatid cyst of the liver and mesentery, with multiple daughter cysts intraoperatively. Excision of the cyst was done and the patient is doing well on postoperative follow-up of 1 year.
Keywords
abdominal cysts
hepatic hydatid
mesenteric hydatid cysts
multiple hydatids

INTRODUCTION
Hydatid disease is relatively uncommon in the pediatric age group.[1] The lung and liver are the usual organs involved.[2] Patients are usually asymptomatic until the cyst grows large enough to cause compression on the adjacent organs and cause symptoms. Pressure effects are initially vague and include nonspecific pain, cough, low-grade fever, and the sensation of abdominal fullness. Often, two or more organs can be involved. It has varied presentations and can mimic intra-abdominal cystic lesions or lymphangioma. We report a case of unusual presentation of hydatid, involving the liver and mesentery in a child.
CASE REPORT
An 11-year-old female child presented, with painless progressive abdomen distension for the past 6 months, associated with loss of appetite. There was no history of constipation, jaundice, hematemesis, cough, breathlessness, burning micturition, or increase in the frequency of micturition. There was a history of cattle rearing in their house. The family relied on a portable water source. On examination, the general condition was fair, with no pallor. Per abdominal examination revealed a 10m8 cm cystic mobile, nontender mass occupying the entire right hypochondrium, right lumbar, and epigastrium. Routine hematological investigations were normal with no eosinophilia and hydatid serology was nonreactive. Ultrasonography of the abdomen was suggestive of a multiloculated, cystic swelling extending from the epigastrium to the pelvis and contrast-enhanced computed tomography (CT) of the abdomen showed a huge hypodense, homogenous cystic lesion with multiple septations, without any calcifications, occupying the entire right side of the abdomen from the liver to the pelvis, pushing the small intestines to the left. The working diagnosis of mesenteric lymphangioma was entertained and, the child was taken up for exploratory midline laparotomy.
Intraoperatively, a large cyst occupying almost the whole of the abdomen, extending from the right hypochondrium to the hypogastrium, was noted. It was identified to be arising from the undersurface of segment 5 of the liver and densely adherent to the mesentery, displacing the entire small bowel to the left. The cyst had two separate “Cyst-pods” one arising from the liver and the other from the base of the mesentery. Multiple daughter cysts were seen inside the cyst (Figure 1A–C). The entire cyst was removed in toto without any spill, leaving a small cavity of size 3 × 5 cms in the liver parenchyma. Histopathology examination revealed multiple hooklets, confirming hydatid disease (Figure 2). Postoperatively, the child was stable and was orally allowed on postoperative day (POD)-2. The patient was discharged on POD-4 after drain removal and was started on tab albendazole (10 mg/kg/day) for 3 months. At 1-year follow-up, the patient is doing well and has no recurrence.
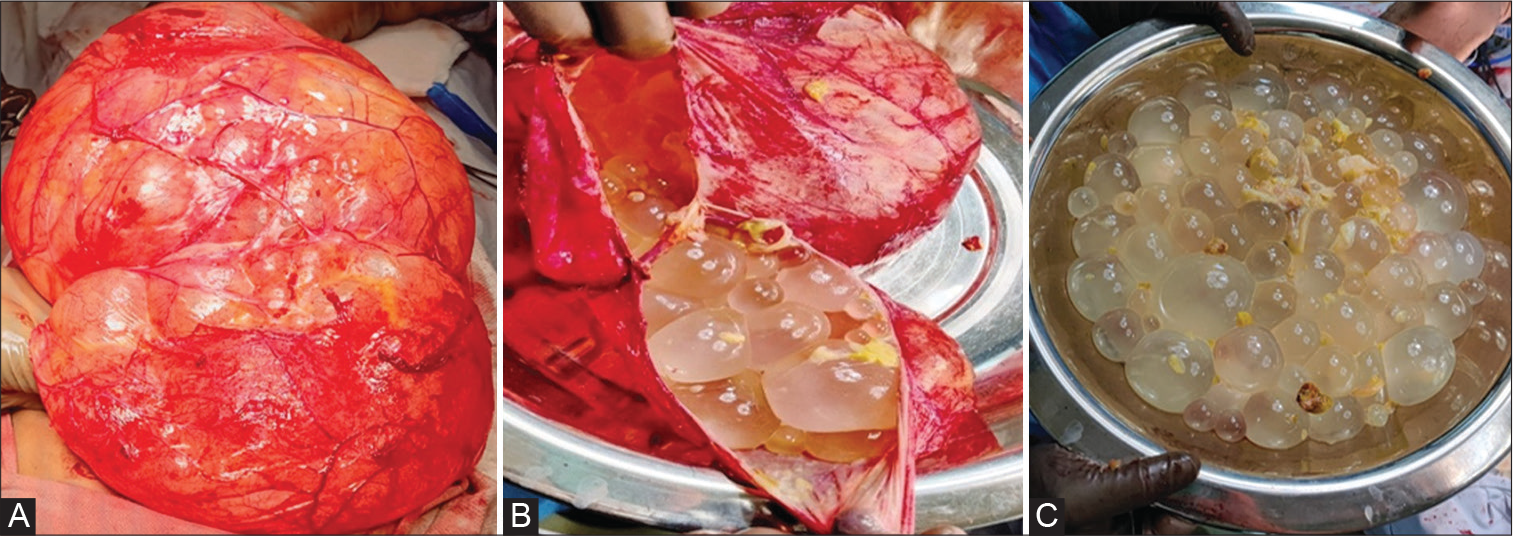
- (A) Intraoperative picture of a large thin-walled cyst, (B) multiple daughter cyst inside the cyst, (C) daughter cyst delivered out.

- Photomicrograph (Wet mount microscopy) showing several hooklets (yellow arrow) of Echinococcus granulosus.
DISCUSSION
Hydatid disease or hydatidosis, caused by Echinococcus granulosus, is endemic in the Indian subcontinent, especially in the sub-Himalayan regions.[3,4] Exposure to pets, lack of proper hand hygiene, scarcity of water, and farming are risk factors of hydatid disease.[5,6] Lung hydatids are more common than the liver in the pediatric age group, contrary to adults.[1] In nearly 8 to 10% of the patients, hydatid cysts can be present in unusual locations like peritoneum, mesentery, and omentum.[2,7,8] Intraperitoneal hydatid disease is seen in approximately 3.9 to 12.5% of patients.[9,10] The involvement of two organs is seen in 5 to 13% of the patients.[11] Patients with hydatid disease may remain asymptomatic for a long period of time until the cyst is large enough to cause symptoms.[12] Hydatid cysts usually present as well-defined thick-walled cystic lesions with daughter cysts. The index case had a flimsy cyst wall contrary to the usually reported intraoperative findings. Prompt treatment of these cysts is recommended as they are prone to complications like rupture, hemorrhage, infection, torsion, and dissemination of the disease.[13] Recurrence due to spillage has been reported in up to 13% of patients.[14] Hydatid cyst can be considered in the differential diagnosis of large intra-abdominal cysts like a mesenteric, omental, or duplication cyst. Mesenteric lymphangioma is also an important differential diagnosis to be considered.
A search of the PubMed and Embase databases using the following search terms: (“liver” OR “hepatic) AND (“mesenteric” OR “mesentery”) AND (“hydatid” OR “hydatidosis” OR “echinococcus”) yielded no such similar case in the pediatric age group. However, the simultaneous occurrence of hepatic and mesenteric hydatid was seen in a 39 year old young man as reported by Paramythiotis et al.[15] The presentation was similar to our index case and the CT imaging revealed three calcified lesions, one in the liver, one adjacent to an ileal loop, and one close to the urinary bladder. Excision of the lesions was done.
Another report by Deshmukh et al[16] revealed multiple hydatids in the liver, mesentery, peritoneum in a 61-year-old female who presented with abdomen distension. Laparotomy and excision of the cysts have been done. In literature, there have been many case reports and series on multiple hydatids of the lung, liver, spleen, peritoneal cavity, etc., but the presence of isolated liver and mesenteric hydatid is very rare. We hypothesize that involvement of the mesentery could be attributed to an event of a subclinical rupture from the liver cyst and intraperitoneal seeding of daughter cysts or escape into the systemic circulation.[17,18] Fortunately, the index case did not develop anaphylaxis and the cyst size gradually progressed causing the symptoms as described.
The goal of treatment in hydatid disease is to prevent rupture and spillage of the hydatid. Depending on Gharbi’s classification, the management of the cyst changes. Surgical treatment is required in Gharbi type 3 and 4 lesions, and open surgery is required in lesions more than 14cm in size.[16,19] However, percutaneous treatment is done in Gharbi type 1 and 2 and no treatment is required in Gharbi type 5. Appropriate scolicidal agents, like 10% povidone-iodine or 3% hypertonic saline, must be used during surgery to prevent anaphylaxis and distant seeding of the disease. Gentle and meticulous dissection is imperative with complete excision where ever possible. Postoperatively, the patients are treated with albendazole (dose: 10 mg/kg/day) for 3 months to prevent a recurrence.[16,19,20]
CONCLUSIONS
Involvement of liver and mesentery with hydatid disease is very rare. In the pediatric age group, trivial trauma while playing can lead to rupture of the cyst and cause the spread of the disease. Mesenteric hydatid cysts present with vague symptoms similar to mesenteric cysts. They should be kept as one of the differential diagnoses, especially in endemic regions. Appropriate management will prevent infection and rupture of the cyst, which can be life-threatening.
Conflict of Interest
None declared.
References
- Hydatid disease in children: a single centre study with analysis of treatment protocol. Int Surg J. 2020;7:6.
- [CrossRef] [Google Scholar]
- Unusual locations of the hydatid cyst: a review from Iran. Iran J Med Sci. 2013;38:2-14.
- [Google Scholar]
- Primary abdominal hydatid cyst presenting in emergency as appendicular mass: a case report. World J Emerg Surg. 2009;4:13.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated peritoneal, mesenteric, and omental hydatid cyst: a clinicopathologic narrative review. Iran J Med Sci. 2017;42:517-523.
- [Google Scholar]
- Abdominal cystic echinococcosis treated with albendazole. a pediatric cohort study. PLoS One. 2016;11:e0160472.
- [CrossRef] [PubMed] [Google Scholar]
- Hydatid disease in children: our experience. Formos J Surg. 2014;47:211-220.
- [CrossRef] [Google Scholar]
- Uncommon locations of hydatid disease: CT appearances. Eur Radiol. 1997;7:1303-1308.
- [CrossRef] [PubMed] [Google Scholar]
- Atypical localizations of hydatid disease: experience from a single institute. Niger J Surg. 2012;18:2-7.
- [Google Scholar]
- "Primary omental hydatid cyst": a rare entity. Case Rep Surg. 2012;2012:654282.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated omental hydatid cyst: clinical, radiologic, and pathologic findings. J Pediatr Surg. 2009;44:1041-1043.
- [CrossRef] [PubMed] [Google Scholar]
- Primary mesenteric hydatid cyst. BMJ Case Rep. 2012;2012:bcr0320125996.
- [CrossRef] [PubMed] [Google Scholar]
- Giant abdominal hydatid cyst masquerading as ovarian malignancy. Singapore Med J. 2007;48:e284-e286.
- [Google Scholar]
- Intraperitoneal rupture of hydatid cysts. Eur J Trauma Emerg Surg. 2017;43:387-391.
- [CrossRef] [PubMed] [Google Scholar]
- Acute intraperitoneal rupture of hydatid cysts: a surgical experience with 14 cases. World J Emerg Surg. 2013;8:28.
- [CrossRef] [PubMed] [Google Scholar]
- Simultaneous hepatic and mesenteric hydatid disease-a case report. Front Surg. 2017;4:64.
- [CrossRef] [PubMed] [Google Scholar]
- Hydatidosis: case report and literature review. Indian J Case Rep. 2020;6:185-187.
- [CrossRef] [Google Scholar]
- Peritoneal hydatid cyst: an unusual cause of abdominal pain in a haemodialysis patient. Nephrol Dial Transplant. 2006;21:1441-1442.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple primary omental hydatid: rare site for a common infestation. Trop Gastroenterol. 2011;32:134-136.
- [Google Scholar]
- Current approaches in the surgical treatment of liver hydatid disease: single center experience. BMC Surg. 2019;19:95.
- [CrossRef] [PubMed] [Google Scholar]
- Primary extrahepatic abdominal hydatidosis. Int J Surg. 2005;3:125-127.
- [CrossRef] [PubMed] [Google Scholar]



