
Translate this page into:
Acute Myeloid Leukemia with Concurrent Inversion 16 and Trisomy 9: A Case Report
Address for correspondence: Subhan Ali Rajasab, Department of Pathology (Cytogenetics), Kidwai Memorial Institute of Oncology, Bangalore 560029, Karnataka, India (e-mail: subhanalir@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Acute myeloid leukemia (AML) are a diverse group of hematological malignancies, each with a distinct clinical, morphological, immunophenotypic, and molecular profile. The World Health Organization (WHO) classifies AML into various subtypes based on recurrent genetic abnormalities, each of which has clinico-pathological and prognostic significance. Inversion(16)(p13q22) or t(16;16)(p13q22) is a balanced structural chromosomal abnormality associated with complete remission and a favorable response to treatment. Trisomy 9 is a numerical chromosomal abnormality with an intermediate risk and is often seen in association with other cytogenetic abnormalities. We describe a case of a 36-year-old female patient who was diagnosed as AML-M4 on peripheral smear and bone marrow evaluation. Cytogenetic studies revealed concurrent presence of inv(16) and trisomy 9. To the best of our knowledge, this is the first case in published literature with simultaneous presence of inv(16)(p13q22) and trisomy 9 in de novo AML.
Keywords
acute myeloid leukemia
inversion(16)
trisomy 9

Introduction
Pericentric inversion of chromosome 16 [inv(16)(p13q22)] and t(16;16)(p13q22) occur between the short arm of chromosome 16 at band 13 and the long arm of the same chromosome at band 22. Inv(16)(p13q22) or t(16;16)(p12q22) is a common recurrent cytogenetic abnormality occurring in de novo cases of acute myeloid leukemia (AML).[1] It is found in 5 to 8% of younger patients with AML.[2,3] It is often found to be associated with other chromosomal abnormalities such as unbalanced t(1;7), trisomy 8, trisomy 22, loss of Y chromosome.[4,5] Isolated trisomy 9 is a rare occurrence in hematologic malignancies. When present, trisomy 9 is considered to be an intermediate risk factor although literature to substantiate its role in disease progression is insufficient.[6,7] Concurrent presence of inversion 16 and trisomy 9 has not been reported in currently published literature, to the best of our knowledge. We present a case of de novo AML-M4 with concurrent inversion 16 and trisomy 9 in a young female.
Case Report
A 36-year-old female patient presented with complaints of fever, dry cough, and generalized weakness lasting 15 days. She had significant weight loss and loss of appetite. Past history and family history were not contributory. There was no history of exposure to toxic agents such as benzene. On examination, she was found to have pallor, mildly enlarged cervical lymph nodes, and mild hepatosplenomegaly. She underwent routine investigations. Hemogram showed hemoglobin of 30 g/L, total leucocyte count of 70 × 109/L, and a platelet count of 30 × 109/L. Peripheral smear revealed 40% blasts. Bone marrow aspirated from the anterior superior iliac spine was hypercellular with sheets of blasts having moderate cytoplasm, fine azurophilic granules, and occasional Auer rods. Nuclear chromatin was fine with two to three conspicuous nucleoli. Immunophenotyping by flow cytometry was performed and the blasts were found to express bright HLA-DR, CD34, CD33, CD13, MPO, CD117, CD64, and CD11c. Correlating cytomorphology of the blasts with their immunophenotypic profile, a diagnosis of acute myeloid leukemia–M4 was made. Serum biochemical parameters were found to be within normal limits. Chest radiograph was normal.
The patient was started on intense chemotherapy regimen comprising injection azacytidine 100 mg slow intravenous infusion in 100 mL of normal saline over 1 hour along with supportive care. At the time of writing this report, the patient had completed two cycles of azacytidine-based chemotherapy and was alive with disease, in partial remission.
Cytogenetic Studies
Chromosome analysis was performed on the bone marrow aspirate before initiation of therapy. The sample was collected in a heparinized tube and cultured for 24 hours and 48 hours without mitogen in RPMI-1640 medium containing 15% qualified heat inactivated fetal bovine serum (GIBCO BRL, USA). The slides were scanned and metaphases were captured using the Olympus BX63 automated microscope. 50 G banded metaphases were analyzed that showed clonal 47,XX, + 9,inv(16)(p13q22) karyotype (►Fig. 1). Trisomy 9 and inversion 16 were confirmed using fluorescent in situ hybridization probes (►Figs. 2 and 3).
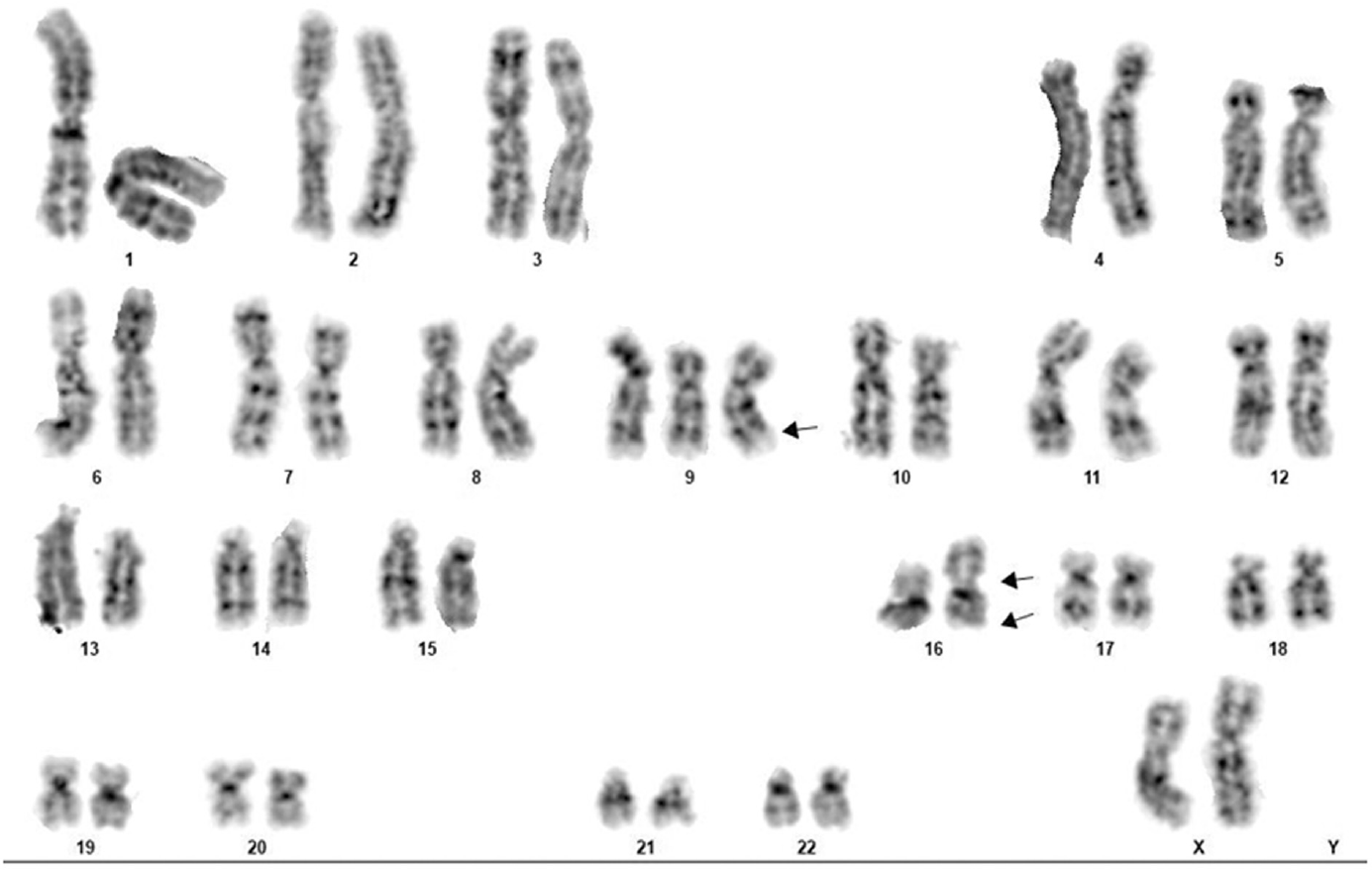
- Conventional karyotype with GTG banding showing 47,XX, + 9,inv(16)(p13q22). Single arrow shows trisomy 9, double arrows indicate inv(16).

- FISH using dual color and dual fusion probe for ABL1-BCR showed three red signals confirming trisomy 9. (A, B) Metaphase FISH, (C) Interphase FISH.
![FISH performed on interphase nuclei using CBFß [16q22] break apart probe from Metasystems Gmbh, Germany, showing two fusion signals in a normal cell and one fusion, one red, and one green signal in an neoplastic cell indicating inv(16).](/content/164/2023/15/1/img/JLP-15-142-g003.png)
- FISH performed on interphase nuclei using CBFß [16q22] break apart probe from Metasystems Gmbh, Germany, showing two fusion signals in a normal cell and one fusion, one red, and one green signal in an neoplastic cell indicating inv(16).
Discussion
Acute myeloid leukemia (AML) are classified based on their recurrent cytogenetic abnormalities, some of which have a good prognosis while others are associated with decreased survival. Trisomy of multiple chromosomes are known to occur in cases of AML. More common is trisomy 8 and is a good prognostic factor. Trisomy 9 is a rare occurrence and its presence is considered as an intermediate risk factor.[7]
Inversion 16 is one of the three recurrent cytogenetic abnormalities associated with high rates of complete remission and clinically favorable prognosis. It is often seen in cases of AML-M4 with eosinophilia, characterized by the presence of atypical eosinophils in bone marrow smear and rarely with M2 and M5 subtypes.[1] Most patients with inv(16) harbor additional cytogenetic abnormalities such as trisomy 22, trisomy 8, or partial deletion of 7q.[3] Inv(16) is detected in approximately 8% of adults diagnosed with AML. It leads to the fusion of the core-binding factor subunit (CBFB, PEBP2B) gene on chromosomal band 16q22 with the smooth muscle myosin heavy chain (MYH11) gene on 16p13.[4]Cbfb/MYH11 allele causes arrest of myeloid differentiation, predisposing to leukemia; however, additional genetic alterations are required for the development of a leukemic phenotype.[5]
Trisomy 9 is a numerical chromosomal abnormality chiefly associated with myeloproliferative and myelodysplastic disorders. Most cases have been found to have idiopathic thrombocytosis. Patients with a history of exposure to toxic agents such as benzene are said to be predisposed to develop trisomy 9. It has rarely been reported as the primary abnormality in AML. The rarity with which trisomy 9 occurs, either alone or in association with other cytogenetic abnormalities, suggest that it may not be a primary event in the pathogenesis of leukemia, but a secondary anomaly associated with clonal evolution of the disease.[8] The presence of inv16 and Trisomy 9 has been reported in earlier studies (►Table 1).
| Abnormality | Diagnosis | No. of cases | Reference |
|---|---|---|---|
| 46, XY, inv(16)(p13.1q22)[1]/47, XY, idem, + 22 [4]/46, XY, idem, t(11;17;22)(q13;q11.2;q13) [9]/46XY [6]. | AML with CLL | 1 | 3 |
| 47, XX, del(7)(q22), inv(16)(p13q22), +22 | AML | 1 | 4 |
| inv(16)(p13.1q22) or t(16;16)(p13.1;q22) | AML | 176 | 5 |
| Trisomy 9 | (Various) | 10 | 6 |
| 47, XX, +9(90%) and 46, XX (10%). | AML | 1 | 7 |
| 47, XX, + 9. | Secondary AML | 1 | 8 |
| 46, XX, inv(16) (p13.1q22) | AML (Therapy related) | 1 | 9 |
| 47, XX,+9, t(9;11)(p21.3;q23.3)[17]/46, XX[3]. | AML | 1 | 10 |
Cases with inv(16)/t(16;16) carry a favorable clinical outcome.[9] High white blood cell (WBC) count, advanced age, and lower platelet count negatively impact the overall survival and disease-free survival. Molecular markers such as the presence of cKit mutations, FLT3 ITD, complex karyotype, inv(3) or t(3;3), t(6;9), MLL rearrangements, del(5q) and del(7q) also have an adverse effect on the outcome of the disease. Isolated trisomy 9 is considered a low-to-intermediate risk factor, but in concurrence with other cytogenetic abnormalities, it may result in the rapid progression of disease with consequent poor prognosis.[6,7,10] Delaunay et al showed that the presence of other additional chromosome structure or number abnormalities or persistence of normal metaphases had no significant impact on CR rate.[11,12,13] Its role in prognostic stratification of AML is not well established due to the rarity of its occurrence. More studies need to be done to establish its role in leukemogenesis.
Conclusion
Cytogenetic analysis at the time of diagnosis is important for risk stratification of AML and is considered one of the most important prognostic indicators used to predict the response to therapy and overall disease progression. It is also an essential criterion for assessing residual disease post-induction and consolidation therapy. FISH can be performed in non-dividing cells and cases with low mitotic index, to detect and confirm cytogenetic abnormalities such as trisomies. AML with inv(16) generally has a favorable outcome. Isolated trisomy 9 is considered a low-to-intermediate risk factor. Its role in prognostic stratification of AML is not well established due to the rarity of its occurrence. Inversion 16 with concurrent trisomy of chromosome 9 prognosis yet to be established with more studies. The final outcome of combination of cytogenetic risk stratification of both good and intermediate risk factors yet to be substantiate with large case studies.
Conflict of Interest
None declared.
References
- Cytogenetic abnormalities in adult non-promyelocytic acute myeloid leukemia: a concise review. Crit Rev Oncol Hematol. 2011;80(03):331-346.
- [CrossRef] [PubMed] [Google Scholar]
- WHO classification of tumours of haematopoietic and lymphoid tissues. WHO classification of tumours. 2017;22008:439.
- [Google Scholar]
- Concurrent acute myeloid leukemia with inv(16)(p13.1q22) and chronic lymphocytic leukemia: molecular evidence of two separate diseases. Am J Hematol. 2006;81(12):963-968.
- [CrossRef] [PubMed] [Google Scholar]
- De novo inversion (16) acute myeloid leukemia in association with trisomy 22, deletion 7q and FLT3 (ITD) associated with complete remission. Archives of Medicine. 2015;7(05):9.
- [Google Scholar]
- Secondary genetic lesions in acute myeloid leukemia with inv(16) or t(16;16): a study of the German-Austrian AML study group (AMLSG) Blood. 2013;121(01):170-177.
- [CrossRef] [PubMed] [Google Scholar]
- Trisomy 9 in a patient with secondary acute myelogenous leukemia detected by fluorescent in situ hybridization. Pathobiology. 1999;67(02):111-114.
- [CrossRef] [PubMed] [Google Scholar]
- Trisomy 9 in a patient with acute myelogenous leukaemia FAB type M2: a rare occurrence. Indian J Hematol Blood Transfus. 2010;26(03):103-105.
- [CrossRef] [PubMed] [Google Scholar]
- Trisomy 9 in hematologic disorders: possible association with primary thrombocytosis. Cancer Genet Cytogenet. 1987;27(01):73-78.
- [CrossRef] [PubMed] [Google Scholar]
- A case of therapy-related acute myeloid leukemia associated with inv(16), with subsequent development of t(9;22) Leukemia. 2006;20(04):746-748.
- [CrossRef] [PubMed] [Google Scholar]
- An extra chromosome 9 derived from either a normal chromosome 9 or a derivative chromosome 9 in a patient with acute myeloid leukemia positive for t(9;11)(p21.3;q23.3): a case report. Oncol Lett. 2019;18(06):6725-6731.
- [CrossRef] [PubMed] [Google Scholar]
- French Acute Myeloid Leukemia Intergroup, Groupe Ouest-Est des Leucémies Aiguës Myéoblastiques, Leucémies Aiguës Myéoblastiques de l'Enfant, Acute Leukemia French Association, Bordeaux-Grenoble-Marseille-Toulouse cooperative groups. Prognosis of inv(16)/t(16;16) acute myeloid leukemia (AML): a survey of 110 cases from the French AML Intergroup. Blood. 2003;102(02):462-469.
- [CrossRef] [PubMed] [Google Scholar]
- Acute Leukemia French Association, Groupe Ouest-Est des leucémies et autres maladies du sang (GOELAMS), Core Binding Factor Acute Myeloid Leukemia (CBF AML) intergroup. Acute myeloid leukemia with translocation (8;21) or inversion (16) in elderly patients treated with conventional chemotherapy: a collaborative study of the French CBF-AML intergroup. J Clin Oncol. 2009;27(28):4747-4753.
- [Google Scholar]
- Prognostic significance of WBC, age, and cytogenetics in patients with core binding factor AML: a comparative study from the French AML intergroup. Blood. 2002;100:748a.
- [Google Scholar]



