
Translate this page into:
Chikungunya Fever Among Patients with Acute Febrile Illness Attending a Tertiary Care Hospital in Mumbai
Address for correspondence: Dr. Lata Baswanna Galate, E-mail: lata.b.galate@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Chikungunya fever (CHIK) is an arboviral disease. Dengue fever (DENG) and CHIK are indistinguishable clinically and need to be differentiated by laboratory investigations.
Purpose:
This study aimed at estimating the seroprevalence of CHIK mono-infection and CHIK and DENG dual infection in suspected patients. We also analyzed the age, sex distribution, joint involvement, and relation of joint movement restriction with visual analog scale (VAS).
Materials and Methods:
Two hundred patients clinically suspected with DENG and CHIK were enrolled from a Tertiary Care Hospital in Mumbai from April 2012 to October 2013. The detailed history and examination findings were recorded. Serum samples were subjected to DENG and CHIK immunoglobulin G (IgM) enzyme-linked immunosorbent assay (ELISA).
Results:
The seroprevalence of CHIK was 12.5%. Mono-infection of CHIK was 3%, and CHIK and DENG dual infection was 9.5%. Most affected age group in CHIK cases was 46–60 years wherein female preponderance was seen. All 6 patients with CHIK mono-infection had fever and joint involvement; knee and elbow were the most commonly affected joints. All CHIK patients had VAS score of 6–10 with restricted joint movement. Of the patients with dual infection, the majorities were from 31 to 45 years with male preponderance; all had fever and joint pain mainly affecting knee and elbow. Of patients who had VAS score 6–10 in patients with dual infection, only 5.26% had restricted joint movement.
Conclusion:
IgM ELISA for Chikungunya infection should be included in the routine laboratory tests for acute febrile illness.
Keywords
Chikungunya
dengue
dual infection
seroprevalence

INTRODUCTION
Chikungunya fever (CHIK) is a mosquito-borne illness caused by the Chikungunya virus (CHIKV).[1] The infection has an acute onset with variable clinical features including the clinical triad of “fever, rash, and arthralgia.”[23] CHIKV, an arbovirus belonging to the genus alphavirus (Togaviridae family), has a single-stranded RNA genome, a 60–70 nm diameter capsid, and a phospholipid envelope.[4]
Since 1953, CHIKV has caused numerous well-documented outbreaks and epidemics in both Africa and South East Asia, involving hundreds of thousands of people,[5] and often separated by periods of more than 10 years. Between 2001 and 2011, a number of countries have reported Chikungunya outbreaks.[5] In India, CHIKV has re-emerged in the states of Andhra Pradesh, Karnataka, Maharashtra, Madhya Pradesh, and Tamil Nadu since December, 2005 after a quiescence of about three decades.[6]
The clinical illness of CHIK needs to be differentiated from dengue fever (DENG) and its variants. A rash occurs in both the diseases but is more common in DENG in which decreased platelet count leads to signs of severe hemorrhage.[78] The probable diagnosis of CHIK can be made on the basis of the clinical triad of fever, rash, and arthralgia. Confirmatory diagnosis of CHIK can be made only by laboratory tests. The virus produces neutralizing and hemagglutination inhibiting (HI) antibodies which can be used to make the serological diagnosis. The HI test is a simple diagnostic test, but it identifies the arboviral group rather than the specific virus. Illness is confirmed by detection of the antigen or antibody to the specific virus in the blood sample of the patient. Reverse transcriptase-polymerase chain reaction (RT-PCR) is confirmatory for the identification of CHIKV. Immunoglobulin G (IgM) capture enzyme-linked immunosorbent assay (ELISA) is the most sensitive serological assay and is necessary to distinguish the disease from dengue.[910] There is paucity of available data from Western India; hence, the present study was undertaken to understand the burden of Chikungunya infection through serodiagnosis among patients presenting with acute febrile illness in a Tertiary Care Hospital in Mumbai.
MATERIALS AND METHODS
The prospective study was conducted in the Department of Microbiology of a Tertiary Care Hospital after Institutional ethical clearance, from April 2012 to October 2013. Patients above 12 years of age with acute febrile illness and joint pain with clinical suspicion of Chikungunya/DENG were included. All patients were screened for malaria, leptospirosis, and typhoid fever using standard laboratory tests and only those patients negative for the above were included in the study.
Two-hundred patients with the above criteria were included in the study. Detailed history of each patient was taken. Age, sex, residential address, number of days of fever, the type of joint involvement, presence of swelling and morning stiffness, visual analog scale (VAS) score, and any restriction of joint movement were recorded. Hematological investigations were recorded. Five ml blood sample was collected after taking consent. Serum was separated and tested for Chikungunya IgM antibodies and dengue IgM antibodies by ELISA.
As per the WHO, a confirmed case of CHIK is a patient fulfilling any one of the laboratory criteria. Hence, the presence of virus-specific IgM antibodies in single serum sample collected in the acute phase is diagnostic of CHIK.[11]
ELISA kit for Chikungunya IgM ELISA was obtained from the National Institute of Virology, Pune. Dengue IgM ELISA was performed using Pan-bio ELISA kit.
RESULTS
Of the 200 patients tested, 6 patients were Chikungunya IgM antibody positive, 151/200 patients were positive for dengue IgM antibodies, and 19/200 patients were positive for both Chikungunya and dengue IgM antibodies.
Hence, 3% patients were diagnosed as CHIK mono-infection, 75.5% patients were diagnosed as DENG mono-infection, 9.5% patients were CHIK and DENG dual infection, and 24% patients had neither infection.
All the patients with CHIK were found in the age group of 13–60 years. No case was identified in the geriatric age group. The most common age group was 46–60 years. Fifty percent (3/6) of the patients with CHIK mono-infection were in this age group. In CHIK and DENG dual infection, 12 (63.15%) patients were in the age group of 31–45 years. In CHIK mono-infection, females were more affected than males, however in dual infection, male preponderance was seen [Table 1].

All the 200 patients suspected of CHIK included in the study presented with fever and joint pain. In CHIK mono-infection, other symptoms were joint swelling (83.33%) followed by headache (66%) and myalgia (66%). Fifty percent (3/6) complained of morning stiffness of joints. In dual infection, myalgia (52.63%), headache (42.10%) followed by rash (36.84%), and joint swelling (26.31%) were other symptoms. Only one patient had morning stiffness. Significantly, more number of CHIK mono-infected patients had joint swelling as compared to CHIK and DENG dual-infected patients, P = 0.0447 [Table 2].

The knee followed by the elbow joint was the most commonly involved joints in mono as well as dual-infected patients.
A VAS is a psychometric response scale which can be used in questionnaires. It is a measurement instrument for subjective characteristics or attitudes that cannot be directly measured.[12]
Visual analog score of ≥6–10 was observed in all patients (100%) of CHIK mono-infection. Only 15.78% of patients with dual infection had VAS score <5 [Table 3].

All the 6 patients with CHIK mono-infection had VAS score of 6–10 with restricted joint movement as compared to only 1 patient with dual infection P ≤ 0.0001 [Table 4].

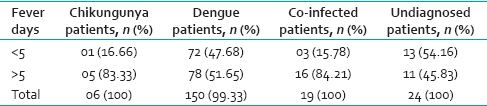
Fever of more than 5 days was seen in 83.33% mono-infection patients and 84.21% dual infection patients.
In DENG, 52.32% patients presented with fever of more than 5 days and 47.68% presented with <5 days of fever [Table 5].
Hematological analysis showed 65% of patients with CHIK mono-infection had normal hemoglobin levels. In patients with dual infection, 14/19 had normal hemoglobin levels and 5/19 had mild anemia. Normal WBC count was seen in 66.66% mono-infection and 89.47% dual-infection patients.
Platelet counts were normal in 4/6 (66.66%) of CHIK mono-infection and 15/19 (78.94%) of CHIK and DENG dual-infection patients. Only 2 of 6 patients with mono-infection and 4/19 patients of dual-infection had low platelet count. In dengue mono-infection patients, 58.27% had low platelet count. Thus, significantly higher number of dengue mono-infection patients had low platelet count as compared to CHIK and DENG dual-infected group, P = 0.0040
DISCUSSION
Since the first isolation of CHIKV in Calcutta in 1963, there have been multiple epidemics in different parts of the country until 1973. Its long absence since 1973 led to the belief that the virus has disappeared from Indian subcontinent and South East Asia.[13] After about three decades of quiescence, Chikungunya epidemic resurfaced in many states of India since December 2005. As outbreaks were also reported from Western India, we undertook a study to understand the disease burden in the citizens of Mumbai.
Over a period of one and half years (2012–2013), 25/200 cases of CHIK were diagnosed, thereby the seroprevalence being 12.5 percent. A study by Kalawat et al. from Tirupati in 2011 have reported the incidence of 18.05% of CHIK.[14]
Dual infection
Dengue and Chikungunya are arboviral infections transmitted by Aedes aegypti mosquito. In areas where both the virus co-circulates, they can be transmitted together. Many factors influence the spread of both viruses which include vector distribution, human travel, urbanization, and climatic changes. As both the infections mimic each other in their clinical presentation, screening for both the viruses would enable us to understand the dual brunt thereby anticipating different outcomes.
In our study, 9.5% patients had dual infection as compared to 2.7% reported by Kalawat et al. from Tirupathi in 2011[14] and 1.15% as reported by Mohanty et al. from Southern Orissa 2011–12.[15]
Age
Suryawanshi et al. have reported 60% cases in the age group of 20–30 years from Nagpur in 2006.[16] Chandra et al. in 2008 from Mangalore have seen patients affected maximally in the age group of 47–56 years (22.8%).[17]
In our study, all cases of CHIK were in the age group of 13–60 years. In patients with dual infection, 84.21% were in the age group of 13–45 years and 15.78% were in the age group of 46–60 years.
Fever and joint pain
In our study, significantly more number of patients with CHIK had joint swelling as compared to the co-infected group.
Fever and joint pain were observed in all cases followed by headache (96%), myalgia (73%), and joint swelling (42.5%) in CHIK as reported by Mohanty et al. from Southern Orissa in 2011–2012.[15]
CHIK is usually abrupt and sudden in onset with high-grade fever for 4–5 days. Symptoms are generally self-limiting.[18] Chikungunya IgM antibodies usually become detectable by 5 days of fever.
In our study, 5 out of 6 patients with mono-infection of CHIK had fever of more than 5 days duration and only 1 patient had fever of 4 days duration. In patients with mono dengue infection and undiagnosed group, 47.68% and 54.16%, respectively, had fever of <5 days duration. It is possible that if these patients were retested after 7 days follow-up, we would have detected and diagnosed few more cases.
A multicentric study by Ray et al. in India had reported that RT-PCR is more sensitive till first 4 days of fever after which IgM ELISA is diagnostic.[19]
Joint swelling
The Chikungunya viral polyarthropathy frequently involves the small joints of the hand, wrist, and ankles.[18]
Our study findings with respect to joint swelling in CHIK infection corroborated with co-infected patients. This highlights a change in presentation of joint involvement. Chandra et al. from Mangalore in 2008 have reported the involvement of ankle (72.2%) followed by knee (60%) and wrist (45%) in patients with CHIK.[17]
Polyarthritis
In our study, all 6 patients with mono-infection with Chikungunya had restricted joint mobility. Only one patient of the co-infected group had restricted movements. A significant association was observed between restrictive joint movement and CHIK as compared to coinfected patients.
No comparative studies are available from India. Chandra et al. have only reported partial disability in 16.8% of cases of CHIK from Mangalore in 2008.[17]
Hematological findings
Our study highlights minimal thrombocytopenia among coinfected patients.
Murhekar et al. have also reported normal platelet counts in patients with CHIK infection from South India.[20]
CONCLUSION
-
This is the first report from Western India of Chikungunya and dengue dual infection
-
This study highlights the clinical and hematological correlation between clinical manifestations of Chikungunya mono-infection and Chikungunya and dengue dual infection
-
All acute febrile illness patients with joint pain should be screened in the laboratory for both Chikungunya and dengue IgM antibodies
-
There is an urgent need for good quality rapid Chikungunya antibody test enabling small private laboratories to diagnose Chikungunya infection.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Human arboviral infections. In: Jawetz, Melnick and Adelberg's Medical Microbiology (23rd ed). Singapore: McGraw Hill; 2004. p. :514-24.
- [Google Scholar]
- Genome microevolution of chikungunya viruses causing the Indian Ocean outbreak. PLoS Med. 2006;3:e263.
- [Google Scholar]
- Differential infectivities of o’nyong-nyong and chikungunya virus isolates in Anopheles gambiae and Aedes aegypti mosquitoes. Am J Trop Med Hyg. 2005;72:616-21.
- [Google Scholar]
- The alphaviruses: Gene expression, replication, and evolution. Microbiol Rev. 1994;58:491-562.
- [Google Scholar]
- Alphaviruses. In: Fields BN, Knipe DM, Howley PM, eds. Fields Virology Vol 1. (3rd ed). Philadelphia: Lippincott-Raven Publishers; 1996. p. :858-98.
- [Google Scholar]
- Chikungunya in India: Global Alert and Response. 2006. [Cited for Epidemiology of Chikungunya] Available from: http://www.who.int/csr/don/2006_10_17/en/
- [Google Scholar]
- Chikungunya disease in infants and children in Vellore: A report of clinical and haematological features of virologically proved cases. Indian J Med Res. 1965;53:764-76.
- [Google Scholar]
- Concurrent isolation from patient of two arboviruses, chikungunya and dengue type 2. Science. 1967;157:1307-8.
- [Google Scholar]
- Arboviruses: Alphaviruses, flaviviruses and bunyaviruses. In: Greenwood D, Slack RC, Peutherer JF, eds. Medical Microbiology (16th ed). London: Churchill Livingstone; 2002. p. :484-501.
- [Google Scholar]
- Vectors of chikungunya virus in Senegal: Current data and transmission cycles. Am J Trop Med Hyg. 1999;60:281-6.
- [Google Scholar]
- Definition of Chikungunya Fever. Available from: http://www.searo.who.int/entity/emerging_diseases/topics/Def_Chikungunya_Fever.pdf
- [Google Scholar]
- Visual Analogue Scale. Available from: https://en.wikipedia.org/wiki/Visual_analogue_scale
- [Google Scholar]
- Clinical Profile of Chikungunya Fever. Available from: http://www.api.india.org/pdf/pg_med_2008/Chapter-42.pdf
- [Google Scholar]
- Prevalence of dengue and chickungunya fever and their co-infection. Indian J Pathol Microbiol. 2011;54:844-6.
- [Google Scholar]
- Seroprevalence of chikungunya in Southern Odisha. J Family Med Prim Care. 2013;2:33-6.
- [Google Scholar]
- Clinical profile of chikungunya fever in patients in a tertiary care centre in Maharashtra, India. Indian J Med Res. 2009;129:438-41.
- [Google Scholar]
- Epidemiologal study on chikungunya outbreak in Mangalore district, Karnataka. Int J Pharma Bio Sci. 2011;2:343-7.
- [Google Scholar]
- Epidemiology, clinical manifestations, and diagnosis of chikungunya fever: Lessons learned from the re-emerging epidemic. Indian J Dermatol. 2010;55:54-63.
- [Google Scholar]
- Chikungunya infection in India: Results of a prospective hospital based multi-centric study. PLoS One. 2012;7:e30025.
- [Google Scholar]
- Treatment practices and laboratory investigations during chikungunya outbreaks in South India. Indian J Med Res. 2011;133:546-7.
- [Google Scholar]



