
Translate this page into:
Clinical manifestations of nocardiosis: Study of risk factors and outcomes in a tertiary care hospital
Address for correspondence: Dr. Teena Wadhwa, Department of Microbiology, Medanta-The Medicity, Sector-38, Gurgaon - 122 001, Haryana, India. E-mail: drteenaarora@hotmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
PURPOSE:
The aim of this study is to evaluate the predisposing risk factors, clinical presentations, laboratory parameters, and treatments taken and outcomes in patients of nocardiosis in the span of 5 years in a tertiary care hospital.
MATERIALS AND METHODS:
The patients whose specimens showed Nocardia like organism in Gram-staining, Kinyoun staining and characteristic colonies in culture were included in the retrospective analysis study. Retrospective analysis of associated risk factors, clinical presentations, and radiological findings was performed.
RESULTS:
Of the thirteen patients, 11 (76.9%) had immunosuppressive pathologies including solid organ transplantation, autoimmune disease, use of steroids, and immunosuppressive drugs as important risk factors. Four types of clinical manifestations were observed, pulmonary (46.1%), cutaneous (23.07%), cerebral (15.3%), and bacteremia (15.3%). The most common presentation was pulmonary with steroid therapy as a significant risk factor. Consolidation and pleural effusion were the common radiological findings in these cases. In eight of the nine patients anti-nocrdial drugs were given. Cotrimoxazole as monotherapy was given in four cases (44.44%), cotrimoxazole in combination with meropenem in two cases (22.22%); minocycline and linezolid were given in one case each. The overall mortality was 36.36% and was seen in patients with pulmonary nocardiosis.
CONCLUSIONS:
The study indicates that Nocardial infections are re-emerging on account of an increase in numbers of immunocompromised patients due to increased organ transplants, autoimmune diseases, malignancies, and use of immunosuppressive drugs and steroids. The diagnosis is often missed/not suspected and delayed because of the clinical resemblance to many other infections. Nocardial infection should be suspected and assessed particularly in immunocompromised patients not responding to treatment/improving clinically.
Keywords
Immunosuppressant drugs
nocardiosis
solid organ transplant
steroids

Introduction
Nocardia is relatively an uncommon known pathogen that causes infections mostly in compromised patients.[1] The majority of infections occur in patients with weakened cell-mediated immunity. Nocardia infections are commonly seen in individuals who undergo bone marrow or solid organ transplantation, patients on immunosuppressive therapy, those with human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome, patients on long-term steroid therapy and those with malignancies.[2]
Nocardiosis usually presents as one of three clinical manifestations pulmonary, central nervous system (CNS), and subcutaneous tissue. Pulmonary nocardiosis is the most common manifestation and is mainly acquired through inhalation of the organism from dust or soil. Other sites of Nocardial dissemination and infection include skin, subcutaneous tissues, and the CNS.[3] The route of spread of organism in disseminated nocardiosis is hematogenous and the organism can spread to involve the brain, eye, bone, joint, heart, kidney, skin, or other organs and tissues.[4] Nocardiosis can virtually disseminate to any organ, most commonly involved is the CNS, and despite giving the appropriate therapy, progression of disease, and relapse usually occur.[5] Co-infection with Aspergillus, Cytomegalovirus (CVM), or Mycobacterium has been reported in nocardiosis patients.[678]
Nocardial infections are less commonly suspected and often misdiagnosed as actinomycosis, Mycobacterium, Cryptococcus, or toxoplasma infections or as malignancies, thus causing a delay in diagnosis and institution of inappropriate therapy which may influence the patient outcome. However, due to increase in the number of immunocompromised patients over past several years, the organism is re-emerging as an important opportunistic pathogen.[9]
This study is aimed to review the clinical and microbiological characteristics; treatment given and outcomes of thirteen cases of Nocardial infection diagnosed in our laboratory in a tertiary care hospital over 5 years. The study also aims to create awareness about infections caused by this forgotten organism.
Materials and Methods
Retrospective analysis of the laboratory confirmed cases of Nocardia on the basis of staining and culture from January 2010 to 2015 was undertaken. The medical records of all the patients were screened for various parameters which included the patient's demographic details, history of transplantation or any other immunosuppressive condition, and use of immunosuppressant drugs or steroids, underlying associated comorbidities (such as diabetes, hypertension (HT), chronic liver disease, chronic kidney disease, and alcoholism), clinical and radiological characteristics, treatments taken and outcomes.
In our laboratory, routinely blood samples and body fluids from sterile sites are received in blood culture bottles and are loaded in Bac-T Alert three-dimensional (3D) system, other samples, including broncho-alveolar lavage (BAL), pus, and sputum are inoculated on blood agar, chocolate agar, and MacConkey agar, incubated at 37°C and examined for growth.
When the bottles loaded in Bac-T Alert 3D system flash positive, an aliquot is taken and centrifuged, smear made from the deposit is processed for Gram-staining. Those cultures that showed Gram-positive branching filaments in Gram-staining were further subjected to modified Kenyon staining using weak acid (1%–2% sulfuric acid) as decolourizer to see the presence of acid-fast branching filaments suggestive of Nocardia. Subcultures on blood agar and MacConkey agar plates were made from all culture bottles showing microorganisms in Gram-staining, incubated at 37°C overnight and examined for growth. The cultures suggestive of Nocardia in Gram's and modified Kinyoun staining were sub-cultured on blood agar, sabaurod dextrose agar (SDA), and Lowensten Jenson (LJ) media and incubated aerobically at 37°C for up to 3 weeks (SDA and LJ). Nocardia growth on blood agar showed dry, chalky white colonies with a characteristic earthy odor. Colonies observed on SDA/LJ media were increased, irregular and folded varying from white to orange. Modified Kinyoun staining was performed from the growth to see acid fastness of the organisms. Microscopy in cases of Nocardia like growth revealed acid-fast branching filaments fragmenting into bacillary and coccoid forms.
Nocardia speciation and antibiotic susceptibility could not be performed as the facility for these is currently not available in our department but will be opted for in the near future.
On the basis of the retrospective analysis, the cases showing Nocardia could be classified into the following groups:
-
Pulmonary nocardiosis: Respiratory samples were positive for Nocardia and lung was the primary site of involvement
-
Cerebral nocardiosis: Nocardia was isolated from cerebrospinal fluid (CSF) and pus from brain abscess
-
Primary cutaneous and soft tissue nocardiosis: Nocardia was isolated from pus from wound or an abscess
-
Nocardia bacteremia: Nocardia was isolated from blood culture samples, either from the central venous line or peripheral line.
Results
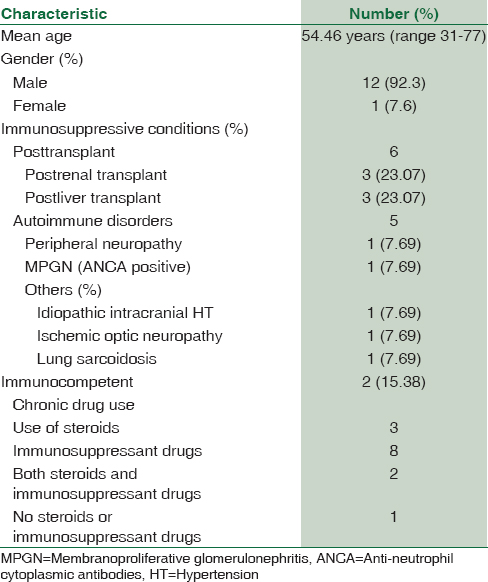
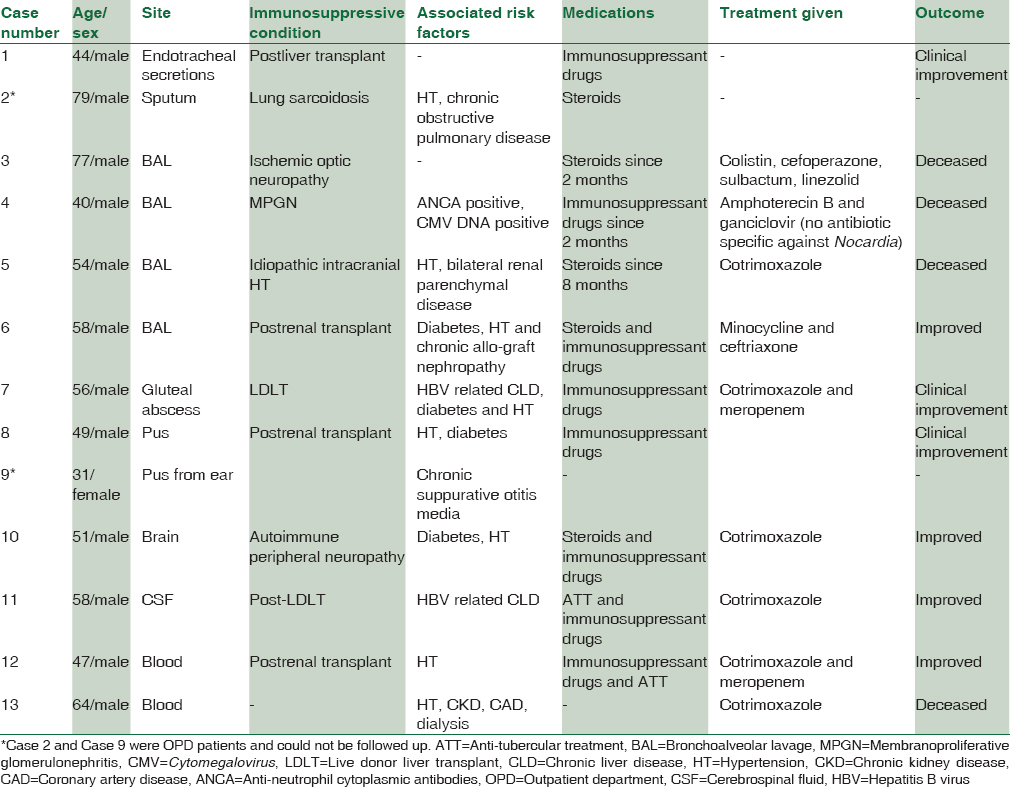
During the period from 2010 to 2015, 13 cases of Nocardial infections were diagnosed, which were positive either by staining or grew in culture. Of them, 12 patients were male and one was female with a median age of 54.46 years. Of the 13 patients, eight patients had clinical condition related to immunosuppression of which six were posttransplant on immunosuppressant drugs [Tables 1 and 2].
Pulmonary nocardiosis
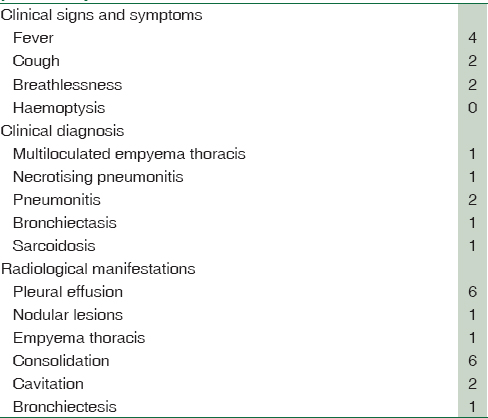
Six patients had pulmonary nocardiosis with the lung being the most common site of involvement and all were either on immunosuppressant drugs or steroids or both [Table 3]. The most common clinical presentation in pulmonary nocardiosis was fever followed by a cough and breathlessness. Pleural effusion and lung consolidation were the common radiological findings.
Case 1
Nocardia was isolated from endotracheal secretions in one patient. High-resolution computed tomography (HRCT) chest was suggestive of consolidation with areas of breakdown and cavity formation involving left upper lobe with multiple parenchymal infiltrates in bilateral lung fields suggestive of infective etiology indicative of tubercular pathology.
Case 2
The patient was presented as an out-patient and could not be followed up.
Nocardia was isolated from BAL in four patients, the details of these patients are described as under:
Case 3
The patient was admitted with respiratory distress. Computed tomography (CT) chest showed segmental and patchy consolidation in bilateral lobes with necrosis suggestive of infective etiology. BAL sample was sent for routine Gram-stain and culture, Gram-staining was suggestive of Nocardia like organism. The patient was managed as a case of Nocardial pneumonia after the laboratory diagnosis of Nocardial infection was made. However, he died due to severe respiratory distress with septic shock.
Case 4
Patient admitted with complaints of fever, cough, and dyspnea. HRCT chest was suggestive of bilateral upper and middle zone consolidation with bilateral pleural effusion. Nocardia was detected in Gram-stain initially. There was also the growth of Aspergillus species in BAL, and the patient was also positive for CVM DNA, thus was being treated as a case of bacterial, fungal, and viral pneumonia but developed severe sepsis and septic shock and succumbed to death.
Case 5
Patient admitted with fever and respiratory distress. Chest X-ray was suggestive of consolidation with pleural effusion. Nocardia like organism was seen in routine Gram-stain and isolated in aerobic culture. Antibiotic therapy specific for Nocardia was started, but the patient died as a result of multiorgan failure and septic shock.
Case 6
The patient was admitted with the complaint of intermittent fever. HRCT chest was suggestive of collapse, consolidation and bronchiectasis left lower lobe with pleural effusion. There was clinical suspicion of pneumonia due to Pneumocystis jirovecii or Nocardia. BALCT sample was negative for Pneumocystis jirovecii in immunofluorescent assay. Nocardia like organism was seen in modified Kinyoun staining and grew in culture. The patient improved clinically after Nocardia directed therapy was initiated.
Primary cutaneous and soft tissue nocardiosis
Two of the three patients with cutaneous nocardiosis were posttransplant patients on immunosuppressant drugs, and the common clinical presentation was fever.
Case 7
Patient admitted with complaint of fever and swelling of the hips. Magnetic resonance imaging (MRI) pelvis showed two large multiloculated gluteal abscess on left side. Pus obtained from drain catheters was sent for culture that grew Nocardia.
Case 8
Patient admitted with high-grade fever and pustular furuncles with gangrenous toes. Nocardia was isolated from pus.
Both these patients [Case 7 and 8] were posttransplant patients.
Case 9
The patient was presented as an out-patient and could not be followed up.
Cerebral nocardiosis
There were two patients of cerebral nocardiosis [Case 10 and 11 in Table 2] and both were on immunosuppressant and anti-tubercular drugs and had presented with complaints of drowsiness and altered sensorium.
Case 10
The patient was a known case of autoimmune peripheral neuropathy and was on anti-tubercular drugs for suspected tubercular lung pathology. He developed seizures for which MRI brain was performed that revealed well-defined circumscribed lobulated cystic lesions in right temporal and occipital lobes showing restricted diffusion with peripheral ring enhancement with thin intralesional septations. The findings were suggestive of brain abscess that could be tubercular. For further evaluation, MR spectroscopy brain was done which was suggestive of Tubercular etiology, so he was continued with anti-tubercular drugs. However, on subsequent follow-up, there was no reduction in the size of brain abscess. Burr hole and drainage of pus was done from the abscess that showed Nocardia like organism in Gram-stain and grew in culture for which cotrimoxazole was added.
MRI brain done on subsequent follow-up showed complete interval resolution of the rim enhancing abscess with a significant reduction in perilesional edema.
Case 11
The patient was post liver transplant with right-sided empyema and meningitis being treated as tubercular was admitted with complaint of drowsiness and altered sensorium. MRI brain showed ventriculitis with entrapped temporal horn of right lateral ventricle. Aspiration of CSF with an intra-ventricular reservoir placement was done in right temporal horn and CSF sample was sent for culture from which Nocardia was isolated.
Nocardia bacteremia
Two patients [Case no 12 and 13 in Table 2] had Nocardia bacteremia; both presented with dyspnea and lymphopenia as the abnormal laboratory parameter.
Case 12
The patient was postrenal transplant patient on immunosuppressant drugs and steroids. CT chest showed multiloculated left empyema thoracis. Video-assisted thoracoscopic surgery was done that revealed dense adhesions of the lung to chest wall and diaphragm, with lower lobe destruction and necrosis and pleural cavity full of multiple pockets of thick pus, thus framing a clinical diagnosis of ruptured lung abscess or necrotizing pneumonia. Pus drained from pleural cavity was sent for histopathology which was suggestive of Nocardia like organism. Nocardia was also grown from two peripheral blood samples of this patient sent on the same day.
MRI brain was done in view of the patient developing generalized tonic-clonic seizures that showed multiple granulomatous lesions involving both cerebral hemispheres which could be tubercular or Nocardial. Anti-tubercular drugs were also added because of persistent fever and high adenosine deaminase levels. The patient became afebrile and was discharged on anti-tubercular treatment) and anti-Nocardial drugs.
Case 13
The patient was admitted with complaint of dyspnea for the past 1 year and diagnosed with lower respiratory tract infection. Ultrasound chest showed bilateral pleural effusion with underlying lung collapse. Bronchoscopy showed left lung field full of blood, BAL was sent for culture that grew Klebsiella pneumoniae for which he was started on broad spectrum antibiotics. Nocardia was isolated from central venous catheter blood sample, antibiotic therapy directed for Nocardia was started, but he died due to septic shock.
Treatment and outcomes
The antibiotic treatment given in four patients was not documented and so could not be ascertained. Nocardia specific treatment was given in eight out of nine patients after the laboratory diagnosis was made. The drugs given were cotrimoxazole in four cases, combination of cotrimoxazole and meropenem in two cases, minocycline in one case, and linezolid in one case.
Outcomes with different treatment regimen were 100% with combination of cotrimoxazole and meropenem, 75% with cotrimoxazole alone and 100% with minocycline and linezolid alone, each.
There were two mortalities in spite of directed anti-Nocardia treatment, one case was on cotrimoxazole, and the other case was on linezolid.
The overall mortality due to Nocardial infection was 36.36% and was mainly in patients with pulmonary Nocardiosis (three out of the four patients who died) and one patient was a case of Nocardial bacteremia.
Discussion
The study showed male preponderance, 12 out of 13 cases being male. A similar finding has been reported by other workers.[101112] Male preponderance may be the effect of male hormones as mentioned by Kontoyiannis et al.[13] There was no significant correlation with age as Nocardia was isolated from posttransplant patients, patients on immunosuppressant drugs, and those having some auto-immune pathology irrespective of age. This emphasizes the fact that Nocardia has re-emerged as a pathogen in populations of immunocompromised patients such as posttransplants patients and other immunosuppressive conditions. Nocardia is re-emerging as important pathogen because of the tremendous increase in a number of such patients. Whenever Nocardia is seen/grown in the laboratory it should not be considered a contaminant. Careful evaluation of the patient should be undertaken and appropriate antibiotic therapy for Nocardia should be instituted with regular follow-up of the patient.
Eleven out of thirteen Nocardia infections were immunocompromised patients, six were postsolid organ transplant cases mainly liver, and renal transplants and five were cases of auto-immune disorders. The most common risk factors for acquiring the Nocardial infection in this study were found to be solid organ transplantation and auto-immune diseases with underlying comorbidities diabetes and HT. Moreover, as per Yang et al.[10] autoimmune disease was the most common risk factor followed by lung pathologies and organ transplantation with underlying co-morbidities such as diabetes and HIV infection.[1012] Matulionyte et al. reported[12] solid organ malignancy to be the most common predisposing factor followed by solid organ transplantation. The difference in predisposing risk factors is easily explained by the fact that a large number of solid organ transplants happen at our institution and HIV infection is not a priority of the hospital.
The results obtained in the present study emphasize the fact that all symptomatic cases of solid organ transplant, those on immunosuppressive therapy for autoimmune diseases and those with HIV infection should be screened for Nocardial infection also.
In the current study, Gram-stain came out to be the sensitive diagnostic test as most of our positive cases were detected in Gram-stain showing the characteristic morphology. This was confirmed on modified Kinyoun staining and growth in the culture media. This finding is similar to that reported by Chedid et al.[14] This indicates that Gram-stain is the efficient staining method to screen for Nocardia. This will be of help for the clinicians even in those cases where the index of suspicion for Nocardia is low as most of our cases were an incidental finding while screening the Gram-stained smear.
The most common organ affected was lung in our study (six patients out of thirteen patients), the same has been reported earlier.[10121415] Pulmonary disease is the predominant manifestation of Nocardial infection because of the primary route of exposure which is inhalation. Pulmonary nocardiosis is usually suppurative in nature, but granulomatous or mixed types are also reported.[16] The significant association of Pulmonary nocardiosis was seen with the use of steroids, four of the six pulmonary cases were on steroids and two on immunosuppressant drugs. The patients presented mainly with symptoms of fever, cough, and breathlessness.[14] The most common radiological finding was pleural effusion followed by consolidation, CT scan of the chest was the diagnostic modality used in our patients of pulmonary nocardiosis as was in the study by Rosman et al.[15] In the study by Wang et al.,[17] Rosman et al.,[15] consolidation was the most common radiological finding followed by cavitation.
Clinical suspicion of Nocardia is less and it is underdiagnosed because of its relatively low incidence and symptoms mimicking tuberculosis, Pneumocystis jirovecii infection, invasive fungal disease or malignancy.[12] The most common initial diagnosis in two patients in our study was tuberculosis because of the clinical similarity between the two as was also reported by Matulionyte et al.[12] Due to similar clinical and radiological presentation, these patients are often started with anti-tuberculous drugs, particularly in country like India where tuberculosis is more common. A classic radiographic picture of tuberculosis that is unresponsive to medication should increase the suspicion of Nocardia infection.[18] CVM was a concomitant viral infection in one patient of pulmonary nocardiosis (Case 4) and could be associated with poor prognosis of the patient as has also been reported by Torres et al.[19]
Cutaneous nocardiosis usually develops after traumatic injury to the skin that involves contamination with soil and unlike other forms of nocardiosis, it mostly develops in immunocompetent hosts. After skin inoculation, a superficial abscess or localized cellulitis may develop.[16] However, in this study, two of the three patients who developed cutaneous and soft tissue infections were posttransplant patients on immunosuppressant drugs as has also been reported by Karumanchi et al.[20] where all three patients in their study had some underlying immunosuppressive condition. Thus, in the current scenario with increase in a number of patients with immunosuppressive pathologies, those presenting with cutaneous lesions along with any associated immunosuppressive condition should also be screened for Nocardia.
Cerebral nocardiosis is uncommon, accounting for only 2% of all cerebral abscesses. Hematogenous dissemination from either the primary pulmonary or cutaneous infection can result in disease in virtually any part of the body, but the brain and soft tissues are most commonly affected. Unlike primary pulmonary and cutaneous infections, which may be self-limiting, lesions of disseminated nocardiosis progress, unless treated.[21] CNS involvement most frequently presents as brain abscesses, although meningitis, diffuse cerebral infiltration, and spinal cord infections have also been described.[16] Two of our patients in this series had CNS involvement, and both were on immunosuppressant drugs, were initially started on antituberculous drugs on clinical ground because of the suspicion of tubercular pathology and nonspecific radiological findings similar to tuberculosis but after the isolation of Nocardia, Cotrimoxazole was added in the antibiotic regimen and response was seen both clinically and radiologically.
Bacteremia due to Nocardia is relatively rare even in immuno-compromised patients despite the fact that Nocardia has propensity for dissemination.[22] We had two cases of bacteremia, one patient was postrenal transplant on immunosuppressant drugs and steroids. Nocardia was isolated from lung abscess as well as both peripheral blood samples suggestive of the lung as the primary target organ with dissemination to blood. The patient had IgG antibodies positive for CVM and Epstein–Barr virus. Al Akhrass et al.[22] also reported CVM infection to be the most common concomitant infection in patients with central venous catheter-associated bacteremia.
Although the primary focus of infection was not identified in the other patient of Nocardia bacteremia; however, it could be lungs as the patient had presented with respiratory symptoms for last 1 year. The patient did not have any underlying immunosuppressive condition; Nocardia in central line could be due to colonization because of the ability of Nocardia to adhere to the biofilm formed on central lines as shown by Al Akhrass et al.[22] Factors that could have contributed to the worsening condition of this patient could be the involvement of lungs and lower respiratory tract infection with K. pneumoniae and septic shock eventually resulting in the death of the patient.
Nine out of 13 cases were given Nocardia specific treatment was started, 66.66% of the patients were given Cotrimoxazole either as monotherapy (44.44%) or in combination with meropenem (22.22%). This is similar to that reported by Chedid et al.[14] and Yang et al.[10] wherein also Cotrimoxazole was used as the major drug for treatment of Nocardial infections. The overall mortality in our case series was 36.36%. Other studies have reported similar finding mortality rate of 42.8% (11) and 41%.[14] Of the two patients who died one had multi-organ dysfunction syndrome with septic shock and was on Cotrimoxazole treatment, the other had a pulmonary infection with acute respiratory distress syndrome, septic shock and was on Linezolid treatment. The predisposing factor in both patients was the use of steroids. The delay initiation of anti-nocardial treatment might have resulted in mortality as the patients were being treated for other infective etiologies.
The limitation of this study was that the Nocardia species identification and antibiotic susceptibility could not be done. Nocardia can be identified to species level using biochemical tests, including hydrolysis of adenine, casein, tyrosine, xanthine, and hypoxanthine. However, as mentioned by Barbara et al.,[23] using these biochemical tests as sole criteria for identification of the species does not provide an accurate identification because of the generally nonreactive nature of most species in these tests and increasing number of described species. Detection of the species by molecular methods can result in rapid and precise identification. Recently, 16S ribosomal ribonucleic acid (rRNA) sequencing is being used more frequently for the identification of the species as was done by Wauters et al.,[24] wherein they studied the species distribution of Nocardia in a large number of clinical samples using 16S rRNA sequencing. Other recent techniques include Pyrosequencing and Ribotyping, these all methods have been published in 2006,[24] they are sensitive and rapid but need more evaluation.
Cotrimoxazole still being used as the common drug. This observation was in our study also where it was used in six patients (either as sole drug or in combination) of the eight patients who were administered specific anti-Nocardial therapy. Clinical improvement was observed in four of these patients. Although we could not do the identification and sensitivity, this did not significantly influence the clinical outcome and prognosis of the patients.
Conclusions
Mostly in critical care and immunocompromised host, index of suspicion for Nocardial infection is extremely low. Although Nocardial infection is known to cause localized and disseminated infections in immunocompromised hosts, it can also cause infections in immunocompetent host with the adverse outcome as seen in the present study (case of bacteremia). Usually, the clinical and laboratory physicians also do not routinely screen for Nocardial infection.
Nocardial infection should be suspected, and screening for the same should be performed in symptomatic cases not responding to usual relevant therapies. Modified Kinyoun staining should be done in all cases suspected of Nocardia like organism in Gram-stain.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Nocardial infections in the United States, 1972-1974. J Infect Dis. 1976;134:286-9.
- [Google Scholar]
- Primary brain abscess caused by Nocardia otitidiscaviarum. Intern Med. 2014;53:2007-12.
- [Google Scholar]
- The medically important aerobic actinomycetes: Epidemiology and microbiology. Clin Microbiol Rev. 1994;7:357-417.
- [Google Scholar]
- Nocardia spp infections among hematological patients: Results of a retrospective multicenter study. Int J Infect Dis. 2013;17:e610-4.
- [Google Scholar]
- Systemic nocardiosis following allogeneic bone marrow transplantation. Transpl Infect Dis. 2003;5:16-20.
- [Google Scholar]
- Pulmonary nocardiosis in a patient with a bone marrow transplant. Bone Marrow Transplantation Team. Bone Marrow Transplant. 1995;15:479-81.
- [Google Scholar]
- Successful treatment of concomitant pulmonary nocardiosis and aspergillosis in an immunocompromised renal patient. Eur J Clin Microbiol Infect Dis. 1993;12:110-2.
- [Google Scholar]
- Pulmonary nocardiosis due to Nocardia otitidiscaviarum in an immunocompetent host- a rare case report. Asian Pac J Trop Med. 2011;4:414-6.
- [Google Scholar]
- Clinical findings of 40 patients with nocardiosis: A retrospective analysis in a tertiary hospital. Exp Ther Med. 2014;8:25-30.
- [Google Scholar]
- Clinical experiences of pulmonary and bloodstream nocardiosis in two tertiary care hospitals in Northern Taiwan, 2000-2004. J Microbiol Immunol Infect. 2008;41:130-6.
- [Google Scholar]
- Secular trends of Nocardia infection over 15 years in a tertiary care hospital. J Clin Pathol. 2004;57:807-12.
- [Google Scholar]
- Nocardia bacteremia. Report of 4 cases and review of the literature. Medicine (Baltimore). 1998;77:255-67.
- [Google Scholar]
- Nocardial infections: Report of 22 cases. Rev Inst Med Trop Sao Paulo. 2007;49:239-46.
- [Google Scholar]
- Nocardiosis: A 15-year experience in a tertiary medical center in Israel. Eur J Intern Med. 2013;24:552-7.
- [Google Scholar]
- Nocardia Species. In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases (8th ed). Philadelphia: Elsevier Churchill Livingston; 2015. p. :2853-2863.
- [Google Scholar]
- Clinical characteristics, microbiology, and outcomes for patients with lung and disseminated nocardiosis in a tertiary hospital. J Formos Med Assoc. 2015;114:742-9.
- [Google Scholar]
- Pulmonary nocardiosis mimicking pulmonary tuberculosis. Indian J Tuberc. 2001;48:211.
- [Google Scholar]
- Nocardiosis in central Kerala: A case series. Int J Med Public Health. 2015;5:384-6.
- [Google Scholar]
- Nocardial brain abscess in an immunocompetent individual. Neurol India. 2011;59:779-82.
- [Google Scholar]
- Central venous catheter – Associated Nocardia bacteraemia in cancer patients. Emerg Infect Dis. 2011;17:1651-8.
- [Google Scholar]
- Clinical and Laboratory Features of the Nocardia spp. Based on Current Molecular Taxonomy. Clin. Microbiol. Rev. 2006;19:259-82.
- [Google Scholar]
- Distribution of Nocardia species in clinical samples and their routine rapid identification in the laboratory. J Clin Microbiol. 2005;43:2624-8.
- [Google Scholar]



