
Translate this page into:
Comparison of Three Blood Culture Techniques in the Diagnosis of Human Brucellosis
Address for correspondence: Dr. Smita Mangalgi, E-mail: smitamangalgi@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Isolation of Brucella is the gold standard in the laboratory diagnosis of brucellosis. As Brucella is intracellular and the number of circulating bacteria is usually low, removal/dilution of antibacterial substances, concentration of bacteria and optimal culture conditions may enhance the rate of isolation.
Aims and Objectives:
The objective of the following study was to compare the lysis concentration (LC), clot culture and conventional Castaneda blood culture techniques for the isolation rate and recovery time in the diagnosis of human brucellosis.
Materials and Methods:
Blood cultures by LC, clot culture and conventional method were performed in 169 patients who had antibody titers ≥160 international units by the serum agglutination test.
Results:
Overall blood culture positivity was found to be 24.8%, 43.1% and 34.9% by conventional, LC and clot culture techniques in that order. The mean recovery time by LC and clot culture techniques was significantly less than conventional method, resulting in an overall difference of nearly 6 and 4 days respectively.
Conclusions:
For the isolation of Brucella from blood, LC and clot culture techniques are better than the conventional technique.
Keywords
Blood culture
brucella
clot culture
conventional
lysis concentration

INTRODUCTION
Brucellosis is endemic in low socio-economic countries like India and the prevalent species causing human infections are Brucella melitensis and Brucella abortus.[1] Contact with the infected animals, consumption of raw milk and ignorance regarding the disease, are the major risk factors.[12] Since clinical manifestations of this disease are protean in nature, laboratory help is a must in the diagnosis. In the laboratory, brucellosis is diagnosed either by isolation of the causative agent and/or by serological tests. Although an array of serological tests is available, Rose Bengal Plate Test (RBPT) and serum agglutination test (SAT) are the most widely used. The sensitivity of RBPT is considerably high, but its specificity is much lower when used to test individuals residing in an endemic area.[3] In the same way, SAT, used to confirm RBPT results, also has limitations of lack of sensitivity as well as specificity.[4567] Apart from this, serological testing does not provide direct evidence for the presence of the pathogen, hence, isolation of Brucella spp. from the clinical specimen is considered to be the gold standard.[289]
Many of the methods have been developed for culturing Brucella spp. from blood specimen, including the conventional Ruiz-Castaneda (Castaneda) method, automated systems, lysis concentration (LC) and clot culture.[1011121314] In general, blood culture for Brucella is performed by conventional Castaneda method where the blood specimen is directly inoculated in the liquid phase of the Castaneda medium. Although the results by this method are satisfactory in acute untreated cases, the incubation time required is very long. The isolation rate is markedly reduced in treated cases or sub-acute/chronic brucellosis patients.[13] The earlier reports have shown an increase in isolation rate and decrease in recovery time by adapting LC technique.[1213] However, both conventional and LC methods require one more blood sample for culture once the serological test is found positive. As it is difficult to obtain one more blood specimen in ignorant patients, clot culture could be a better option. Isolation of Salmonella by clot culture has been tried by many workers.[151617] Reports on clot culture for Brucella are scarce and controversial.[1518] Hence in this study, an attempt has been made to compare LC, clot culture and conventional culture techniques for the isolation of Brucella from blood specimen in an endemic area.
MATERIALS AND METHODS
Blood culture by all the three techniques was performed in 169 out of 191 patients showing SAT titer of ≥160 international units (IU) after obtaining written consent. Depending on the duration of the disease, patients were divided into three groups as: acute (<8 weeks), sub-acute (8-52 weeks) and chronic (>52 weeks) brucellosis.[1518] Patients were considered to have relapse/re-infection if symptoms reappeared within a year after the completion of antibrucellar treatment.
Five ml of blood was collected aseptically from patients with the clinical symptoms resembling brucellosis (fever, malaise, joint pain, low backache, headache, and weight loss) in a sterile, plastic screw capped bottle with 6-7 glass beads of 2 mm diameter. The sample was allowed to clot. The specimen was centrifuged at 2000 rpm for 15 min; the serum was separated aseptically and used for serology. The clot was preserved in the refrigerator for clot culture if needed.
Blood sample for conventional and LC culture technique was collected from patients who had significant SAT titers (≥160 IU). About 10 ml of blood was collected in adults and 5 ml in case of children. The specimen was equally distributed and processed for conventional blood culture and LC technique.
Conventional culture technique
The blood specimen was inoculated aseptically into the broth phase of Castaneda's biphasic medium consisting of brain heart infusion agar and broth with Brucella selective supplement (Hi-Media).
LC technique
Procedure described by Etemadi et al., was employed with a minor modification.[12] 5 ml of blood was added to 40 ml of sterile distilled water with 1.5 ml of 4% sodium citrate in adults and 2.5 ml was added to 20 ml of sterile distilled water with 0.75 ml of 4% sodium citrate in children, in a sterile screw caped centrifuge tube. The contents were gently mixed and the tubes were centrifuged at 7,000 rpm for 30 min. The supernatant was discarded and the sediment was inoculated in the Castaneda's medium, instead of culture plate.
Clot culture technique
The blood clot preserved in the sterile screw capped plastic tube with glass beads after removal of serum was used for this method. The clot was disrupted by shaking the tubes on a shaker for 15 min. The disrupted clot was then inoculated in Castaneda's medium.
Incubation
The media were incubated at 37°C with 10% CO2 for a maximum of 30 days.
Recording of results
The bottles were observed daily for growth. Sub-culturing was done by allowing the blood broth mixture to flow over the solid phase. The day of appearance of the first colony was recorded for comparison of growth rates.
Identification and confirmation of the isolates
The isolates were identified based on colony morphology, gram stain, modified “ZN” staining, CO2 requirement, biochemical tests like oxidase and urease, H2S production for 4 days and growth in the presence of basic fuchsin (1:50,000 and 1:100,000) and thionin (1:25,000, 1:50,000 and 1:100,000). Provisional confirmation and bio-typing of the isolate was done by performing slide agglutination test using B. abortus and B. melitensis monospecific antisera (Murex Biotech). The isolates were confirmed at IVRI Izatnagar/DRDE Gwalior.
The study was approved by the Institutional Ethical Committee.
Statistical analysis
Statistical analysis of the data was performed by GraphPad InStat software designed by GraphPad Software, Inc. USA. Chi-square test with Yate's correction was used for comparison.
RESULTS
Blood culture by all the three techniques was performed in 169 out of 191 patients. Overall blood culture positivity was found to be 24.8%, 43.1% and 34.9% by conventional, LC and clot culture techniques respectively. The isolation rates in patients with acute, sub-acute, chronic brucellosis and relapse/reinfection by various culture techniques are given in Table 1.
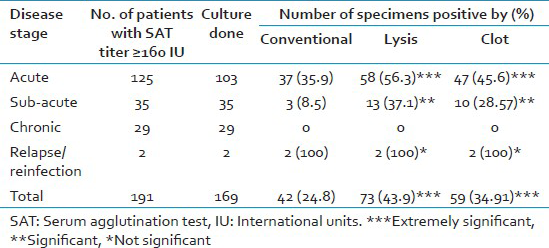
When compared with the conventional technique LC and clot culture techniques yielded growth in significantly more number of cases (P < 0.0001). Isolation rate was high in acute stage compared with sub-acute stage. Brucella could not be isolated in chronic patients by any of the methods.
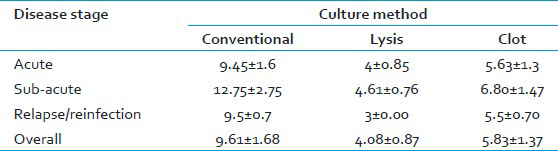
The mean recovery time for conventional technique was 9.61 days (standard deviations [SD] ±1.68), whereas with LC and clot culture techniques it was 4.08 (SD ± 0.87; P < 0.0001) and 5.83 (SD ± 1.37; P < 0.0001) respectively. In the acute stage, recovery time was relatively less by all the three methods [Table 2]. Earliest growth by the conventional technique was seen on the 6th day where as it was on the 3rd day with both LC and clot culture techniques. LC technique showed earlier growth in 96% blood cultures, before the first positive culture by conventional method was noted, whereas clot culture yielded earlier growth in 42.55% of cultures. Maximum incubation time required for culture to be positive by LC, clot culture and conventional technique was 6, 9 and 16 days respectively. After 16th day, no culture was found positive, though the cultures were incubated for 1 month. Despite maximum aseptic precautions taken during collection and processing of the sample, contamination rate was high for clot culture (5.32%) followed by LC (2.95%), may be due to more number of manipulations required for the procedure. None of the conventional cultures showed contamination.
DISCUSSION
In the present study, blood culture positivity was found to be 24.8%, 43.1% and 34.9% and the recovery time was 10, 4 and 6 days by conventional, LC and clot culture techniques respectively. Our findings suggest that LC and clot culture methods are more sensitive and require less time than conventional culture thereby helping in early detection of infection. Among the LC and clot culture techniques, LC was better due to increased isolation rates and decreased recovery time. Similar findings have been reported by Etemadi et al., Mantur and Mangalgi and Espinosa et al.,[121314]
The mean recovery time by LC in this study was 4.08 days, which is in agreement with Espinosa et al.,[14] but slightly more as compared to the results of 2 and 2.7 days by Etemadi et al., and Mantur and Mangalgi.[1213]
In a study done by Escamilla et al., clot culture technique was found to be less sensitive and more labor-intensive when compared with the conventional method.[15] Conversely in our study, clot culture technique was more sensitive and also the recovery time was less when compared with the conventional method. Similar findings have been reported by Mantur et al.,[18] Another advantage of this technique is that need for one more blood sample is alleviated.
In a study by Espinosa et al., isolation rate was higher in sub-acute cases than in patients with acute brucellosis by LC technique.[14] Whereas far higher isolation rates in both acute and chronic stages have been reported by Mantur and Mangalgi.[13] In our study, culture positivity rate was high in patients with acute followed by sub-acute brucellosis and none of the chronic cases grew Brucella.
As the patients in our study were not relieved of their symptoms over a long time, they switched on to many doctors before being diagnosed as brucellosis cases at our hospital, which could be an attribute for our lower isolation rates. History of minimum 3-4 courses of antibiotics was elicited in 116 (68.63%) patients.
In general, blood cultures are attempted to confirm the presumptive serological diagnosis. In India, especially in rural areas, due to the misperception that blood once lost is lost forever and blood loss enhances the disease; it is difficult to obtain one more blood specimen for culture in seropositive individuals. In such situations and also in field conditions (camps), wherein obtaining a second sample for culture is difficult, clot culture could be the optimal alternative. Both lysis and clot culture require manipulations, which enhance the chances of laboratory infection and contamination, thereby necessitating strict biosafety and aseptic measures.
CONCLUSIONS
We propose that for the isolation of Brucella from blood specimen, LC method is better than conventional Castaneda's method as the isolation rate is high and the recovery time is less. Clot culture is a better option when a second blood sample cannot be obtained for culture. As lysis and clot culture techniques are sensitive, simple and inexpensive and yield earlier results, they can be adapted in the technically and economically backward areas where automated systems are far from reach. However, to prevent laboratory acquired infection, these methods are to be carried out in Class II biosafety cabinet with BSL-3 precautions.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Laboratory diagnosis of brucellosis in a rural endemic area in Northeastern Spain. Int Microbiol. 2004;7:53-8.
- [Google Scholar]
- Evaluation of seven tests for diagnosis of human brucellosis in an area where the disease is endemic. Clin Vaccine Immunol. 2008;15:1031-3.
- [Google Scholar]
- Seroprevalence of human brucellosis in rural endemic areas in eastern Turkey. Trop Doct. 2008;38:42-3.
- [Google Scholar]
- Seroprevalence study of human brucellosis by conventional tests and indigenous indirect enzyme-linked immunosorbent assay. ScientificWorldJournal 2012 2012 104239
- [Google Scholar]
- Comparison of a dipstick assay for detection of Brucella-specific immunoglobulin M antibodies with other tests for serodiagnosis of human brucellosis. Clin Diagn Lab Immunol. 2003;10:612-5.
- [Google Scholar]
- Diagnosis of brucellosis by using blood cultures. J Clin Microbiol. 1997;35:2417-8.
- [Google Scholar]
- Evaluation of conventional castaneda and lysis centrifugation blood culture techniques for diagnosis of human brucellosis. J Clin Microbiol. 2004;42:4327-8.
- [Google Scholar]
- Comparison of culture techniques at different stages of brucellosis. Am J Trop Med Hyg. 2009;80:625-7.
- [Google Scholar]
- Evaluation of blood clot cultures for isolation of Salmonella typhi, Salmonella paratyphi-A, and Brucella melitensis. J Clin Microbiol. 1986;24:388-90.
- [Google Scholar]
- The study of salmonellosis with reference to salmonella typhi in enteric fever patients. Journal of Clinical and Diagnostic Research. 2011;5:467-9.
- [Google Scholar]
- Comparison of whole blood culture and blood clot culture for the diagnosis of enteric fever. JKIMSU. 2013;2:145-6.
- [Google Scholar]
- Diagnostic yield of blood clot culture in the accurate diagnosis of enteric fever and human brucellosis. Clin Lab. 2007;53:57-61.
- [Google Scholar]



