
Translate this page into:
Cryoglobulinemia as an Initial Manifestation of Underlying Hematological Malignancy: A Rare Occurrence in India
Address for correspondence: Dr. Narender Kumar, E-mail: kumar.narender@pgimer.edu.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cryoglobulinemias rarely been reported from India even though associated conditions such as hepatitis C infection, rheumatoid arthritis and plasma cell dyscrasias, etc., are common occurrences. In many regions of the country, temperatures in winter can be conducive to the precipitation of cryoglobulins, yet epidemiology of the disease suggests that it is a common condition in the west. We encountered a 68-year-old-male patient who presented with a history of headache off and on along with hepatosplenomegaly. The rare occurrence of cryoglobulinemia in our setting can delay the diagnosis, as happened in our case, since the index of suspicion of clinicians and laboratory personnel is low. We are reporting this case because of the rarity and protean clinical manifestations of cryoglobulinemia.
Keywords
Cryoglobulin
cryoglobulinemia
lymphoplasmacytic lymphoma
rouleaux formation

INTRODUCTION
Cryoglobulins are special serum immunoglobulin's that usually precipitate at a temperature between 0°C and 4°C and dissolve when re-warmed to 37°C. This in vitro phenomenon can be observed in a wide spectrum of infectious diseases, autoimmune disorders and with hematological malignancies.[12] The classification of cryoglobulinemia was proposed by Brouet et al.[3] They classified cryoglobulins in to three types. Type I and II are monoclonal while type III is polyclonal. Both type I and type II are associated with lymphoproliferative disorders.[3] During the winters in the North India temperature usually falls in between 0°C and 10°C. Such cold weather is likely to produce cold-induced symptoms in patients with cryoglobulinemia.[4] As very low temperature is unusual in Indian subcontinent, cases of cryoglobulinemia are usually remains symptomless and hence undetected.[5] We encountered an interesting case of cryoglobulinemia in a 68-year-old-male who presented with cryoglobulinemic manifestations for the last 18 months.
CASE REPORT
A 68-year-old male patient who was chronic alcoholic presented with complain of headache on and off for the last 18 months before presenting to us in September 2011. There was no history of jaundice or ascites. On examination, there was hepatomegaly (3 cm below costal margin) and splenomegaly (2 cm below costal margin) however no palpable lymph nodes are noted. In the past history, his peripheral blood was sampled multiple times in private laboratories. However, he was not able to get any report since his sample clotted soon after sampling.
The patient was sent for routine blood investigations. Although, phlebotomist had taken the venous blood sample but it clots itself even in the presence of anticoagulants. He tried a few times but the whole process was in vain. Subsequently, he informs the case to the consultant in Hematology. Following this, patient was called on the next day and sampling was done by maintaining the whole set up temperature at 37°C and above. This time the sample did not clot.
Serological investigations for hepatitis B virus, hepatitis C virus, and human immunodeficiency virus infection were performed to exclude any viral infection and no associated infective etiology was found. Serum sample for detection of antibodies (rheumatoid factor, antinuclear antibodies, smooth muscle antibody, anti-mitochondrial antibody) for any underlying autoimmune disorder was sent for however all the tests came negative.
The hemogram showed bicytopenia with hemoglobin of 3.9/dl and total leucocyte count of 2.9 × 109/L. The platelet count is within normal range (216 × 109/L). Peripheral blood film showed extensive rouleaux formation [Figure 1a].
Bone marrow aspirate was performed. The marrow was cellular and clotted; however showed the presence of homogenous pale pink background due to the presence of cryoglobulins [Figure 1b]. Erythropoiesis and megakaryopoiesis were normal. Differential nucleated cell count showed extensive increase in lymphocytes (73%) along with plasma cells (8%) [Figure 1c]. Bone marrow biopsy showed the presence of interstitial and nodular aggregates of lymphoid cell. The sinusoids were dilated and are filled with pale eosinophillic material (cryoglobulins) [Figure 1d]. Bone marrow fibrosis was increased (grade 3)[6]. Immunophenotying was performed on bone marrow sample and that showed expression of CD19, CD79b along with heterogeneous expression of CD23 [Figure 2]. Serum protein electrophoresis showed the presence of sharp M band in the gamma region, hence proving monoclonality of disease. Immunofixation for specific immunoglobulin was advised but unfortunately patient cannot afford further testing. On the basis of peripheral blood, bone marrow and flowcytometry findings a diagnosis of Lymphoplasmacytic Lymphoma was made. The patient was started on prednisolone 1 mg/kg/day and was asked to report weekly. The patient is now in follow-up and show improvement in their symptoms and easy sampling of blood.
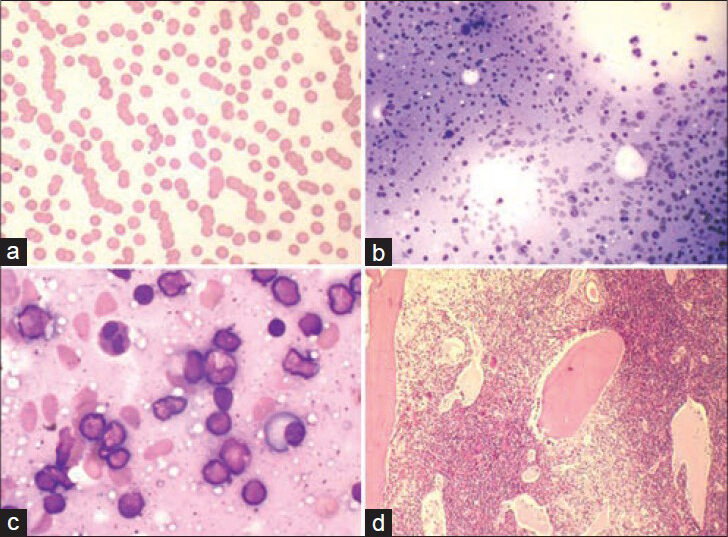
- Peripheral blood shows rouleaux formation (MGG-Giemsa, ×400) (a). Bone marrow aspirate shows presence of pink homogenous material due to cryoglobulins (MGG-Giemsa, ×200) (b). High power view demonstrates increase in numbers of lymphocytes and plasma cells (MGG-Giemsa, ×1000) (c). Dilated sinusoids filled with pale eosinophillic material are seen on trephine biopsy section (H and E, ×100) (d)
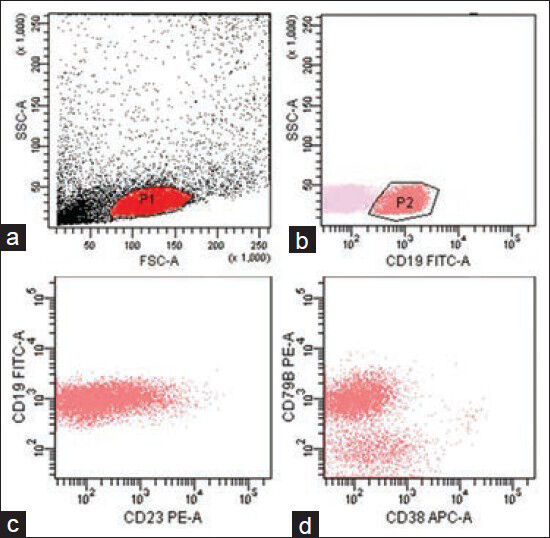
- Panel of scatter plots showing the multicolor immunophenotyping of bone marrow aspirate sample by flow cytometry. The gating of cells in each tube has been done on side scatter-A (SSC-A) versus forward scatter-A (FSC-A) (a). The cell is lymphoid region P1 were subsequently gated in SSC-A versus CD19 plot with the gated P2 population showing surface CD19 expression (b). The gated cells show heterogeneous expression of CD23 along with homogeneous expression of CD79b (c and d)
DISCUSSION
Cryoglobulins are proteins that can precipitate at low temperatures (<4°C) and dissolve when re-warmed to 37°C. The final product of this precipitate is known as “cryocrit” The cryoglobulin can be defined on the basis of its composition: Polyclonal or monoclonal immunoglobulins; or the presence of rheumatoid activity (RA). Three types of cryoglobulinemia have been identified namely: Type I includes monoclonal cryoglobulins (IgM, IgG and IgA) without any RA; type II includes a monoclonal component (usually IgM with RA) and a polyclonal component (usually IgM/IgG); type III have several polyclonal components and a component with RA (usually IgG/IgM). Type II and type III are classically referred to as mixed cryoglobulinemia.[3]
In general, cryoglobulinemia regardless of their type are associated with skin manifestations, but may also cause rheumatologic symptoms that involve the kidneys, the peripheral nerves or central nervous system, the lungs, the myocardium and the gastrointestinal tract.[7] Interesting the present case does not have any characteristic symptom. The only central nervous system manifestation is in the form of headache.
Type I cryoglobulinemia is associated with low grade lymphoproliferative disorders such as multiple myeloma, Waldenstrom macroglobulinemia, chronic lymphatic leukemia and account for 10-15% of all cases of cryoglobulinemia. Type II cryoglobulinemia is associated not only with lymphoproliferative diseases but also with autoimmune disorders and infective etiologies especially hepatitis. Type III cryoglobulinemia is frequently seen in patients with autoimmune or infectious diseases.[8] This case is also having lymphoplasmacytic lymphoma and hence can be categorized in to type I cryoglobulinemia.
In tropical and subtropical countries like India where the winter is either nonexistent or very brief, most of the patient with cryoglobulinemia did not show any symptoms and remain undetected. In this case, difficulty in processing of sample raises the suspicion of disease which was confirmed by bone marrow examination and by exclusion of other autoimmune etiology along with infective pathology. The diagnosis of Lymphoplasmacytic Lymphoma on bone marrow aspiration solves the underlying pathogenesis of the cryoglobulinemia.
CONCLUSION
We presented a case of cryoglobulinemia which is very rare in Indian subcontinent and was suspected due to the problem in sampling and processing of the blood.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Hepatitis C virus, cryoglobulinaemia, and vasculitis: Immune complex relations. Lancet Infect Dis. 2005;5:227-36.
- [Google Scholar]
- Biologic and clinical significance of cryoglobulins. A report of 86 cases. Am J Med. 1974;57:775-88.
- [Google Scholar]
- Some observations on cryoproteinemia (from India) Aspect Allergy Appl Imrnunol. 1981;13:36-40.
- [Google Scholar]
- Clinical and immunological profile of cryoglobulinaemia in North India. Asian Pac J Allergy Immunol. 1984;2:227-31.
- [Google Scholar]
- Quantitation of bone marrow reticulin - A normal range. Am J Clin Pathol. 1971;56:24-31.
- [Google Scholar]
- Characteristics and outcome of 49 patients with symptomatic cryoglobulinaemia. Rheumatology (Oxford). 2002;41:290-300.
- [Google Scholar]



