
Translate this page into:
Hepatic Tuberculosis Mimicking Metastasis in a Case of Carcinoma Sigmoid Colon
Address for correspondence: Dr. Sabina Khan, E-mail: drsabina1@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Tuberculosis (TB) presenting as isolated liver mass without clinical evidence of TB is difficult to diagnose preoperatively and is usually mimicked by primary or metastatic carcinoma of the liver. Hepatic TB associated with carcinoma colon is a rare association which has very rarely been reported in the literature. This case illustrates the diagnostic difficulties of hepatic TB and the need to consider it in the differential diagnosis of hepatic nodular lesions in carcinoma colon patients. Here, we report a case of 48-year-old female who presented in the casualty with features of acute intestinal obstruction. Preoperatively a mass was seen at the hepatic flexure along with three lesions in the liver presumed to be metastatic in origin. However, histopathology of the mass revealed adenocarcinoma colon and the liver lesion proved to be hepatic TB. We wish to highlight that on encountering a hepatic lesion in a carcinoma colon patient the possibility of hepatic TB should also be kept in mind apart from the obvious possibility of metastasis especially in an endemic country like India.
Keywords
Carcinoma colon
hepatic lesion
hepatic tuberculosis

INTRODUCTION
Tuberculosis (TB) is a global health problem fairly common in India. Usually, lung involvement is seen. However, 6–38% patients of active pulmonary TB may have abdominal TB.[1] Abdominal TB, a common clinical entity in Indian sub-continent can infect the gastrointestinal tract, peritoneum, mesentery, lymph nodes, liver, spleen and pancreas. Hepatic TB is usually associated with miliary TB or active pulmonary TB. However, isolated liver TB in the absence of miliary TB is very rare restricted to case reports and case series in English literature.[2] Hepatic TB associated with carcinoma colon is much rarer. The diagnosis is often delayed due to lack of specific symptoms and laboratory findings.
Here we report a case of synchronous hepatic TB and adenocarcinoma of the colon which is a very rare finding with only a few reports in the literature and none from the Indian subcontinent. This case illustrates the diagnostic difficulties of hepatic TB and the need to consider it in the differential diagnosis of hepatic nodular lesions in carcinoma colon patients. Increased awareness of this rare association can prevent needless laparotomy as these patients respond well to anti-tubercular treatment.
CASE REPORT
A 50-year-old female presented to the emergency department with pain in the abdomen since 5 days, vomiting and constipation since 3 days. There was no history of fresh bleeding per rectum or malena. She had a history of abdominal hysterectomy 2 years back for multiple uterine fibroids. She had no other co-morbidities, and her family history was not significant.
On examination she was conscious, oriented with a regular low volume pulse of 98/min, blood pressure 98/66 mmHg, respiratory rate 22/min, and temperature of 98.8 F. Abdominal examination revealed mild distension with visible peristalsis. A lower midline irregular scar was seen; no lump was palpable. All the hernial orifices were intact. The patient had generalized tenderness, and the bowel sounds were exaggerated. Rectum was empty on per rectal examination, and there was no evidence of any growth. Clinical impression of acute intestinal obstruction was made, and the patient was subjected to blood and radiological investigations. Her blood investigations were - hemoglobin: 9.1 g/dl, total leucocyte count: 7000 cells/mm3, serum bilirubin 0.9 mg%, serum glutamic-oxaloacetic transaminase: 55 IU, serum glutamic pyruvic transaminase: 48 IU, blood urea: 29 mg%, serum creatinine: 1.4 mg%, potassium: 3.2 meq/l, sodium: 139 meq/l, random blood sugar: 98 mg%
Patient was subjected to X-ray abdomen and chest. X-ray abdomen showed multiple air fluid levels while chest X-ray was normal. Computerized tomography scan was not done as it was not available in emergency. Ultrasound Abdomen revealed distended bowel loops. Based on history, clinical examination and X-ray findings, an impression of acute intestinal obstruction secondary to postoperative adhesions was made.
Exploratory laparotomy was planned after adequate resuscitation. Exploration revealed distended small bowel and caecum with a circumferential growth at the hepatic flexure of size around 5 cm × 5 cm. Large bowel distal to the lesion was collapsed. The mesenteric lymph nodes were enlarged, and there were three liver lesions, two on the right lobe and one on the left ranging in size from 2 cm to 5 cm. There was no evidence of any free fluid or peritoneal deposits. An extended right-sided hemicolectomy with ileocolic, end-to-end anastomosis was done. Biopsy from the liver lesion of the largest size was taken. Mass closure of the abdomen was done with a single drain in the pelvis. Patient recovered well though she developed superficial surgical wound infection which was treated with irrigation and antibiotics as per the culture and sensitivity.
Post-operative contrast enhanced computerized tomography of the abdomen showed multiple hypodense lesions in both lobes of the liver suggestive of metastases [Figure 1a and b]. Histopathological examination of the resected bowel revealed well-differentiated mucin secreting adenocarcinoma invading the muscular layer [Figure 2c and d]. Twelve lymph nodes isolated were uninvolved by the tumor (Stage pT2N0). Biopsy from the liver nodules showed multiple confluent epithelioid granulomas with caseation necrosis suggestive of TB [Figure 2a and b]. No metastatic deposit was seen.
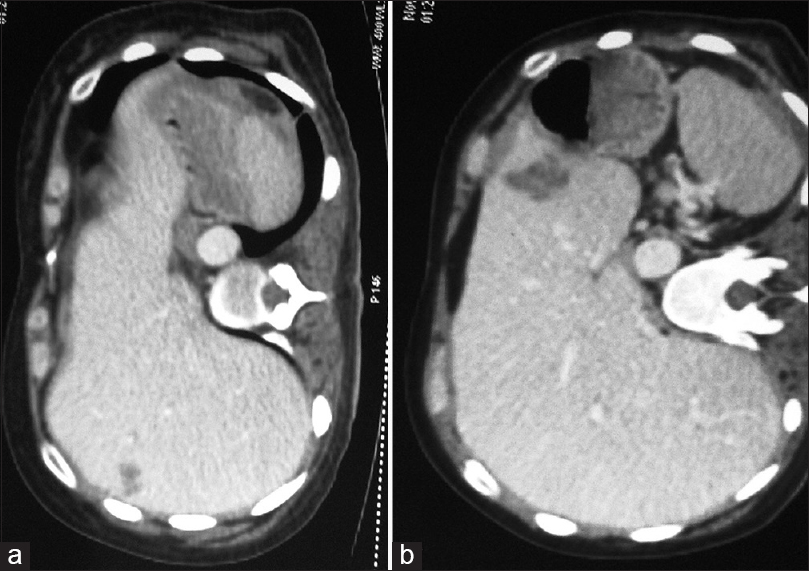
- Hypodense lesion in segment 7 of the liver suggestive of metastasis (a). Hypodense lesion in segment 3 of the liver suggestive of metastasis (b)
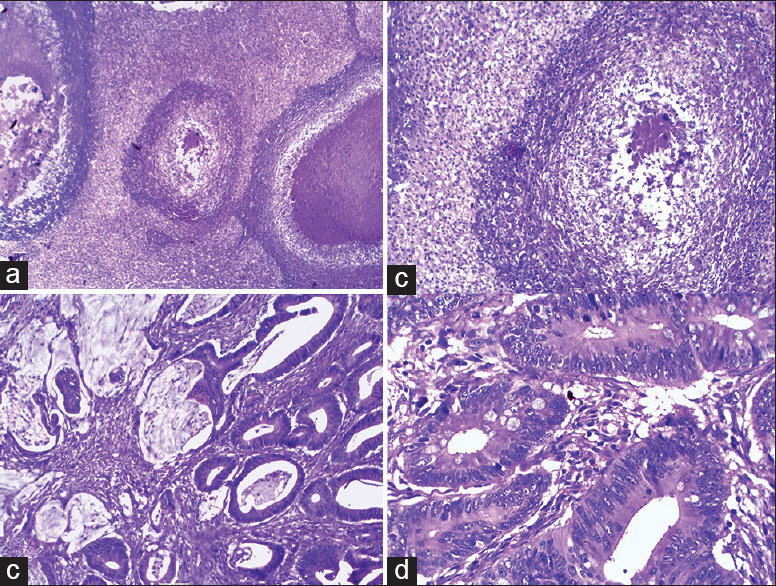
- Microphotograph showing numerous confluent epithelioid granulomas effacing the normal liver architecture (H and E, ×100) (a). High power view of caseating granuloma with adjacent normal hepatocytes (H and E, ×400) (b). adenocarcinomatous glands with extracellular mucin infiltrating the muscle layer (H and E, ×100) (c). High power view showing glands lined by malignant cells having enlarged hyperchromatic nuclei, coarse chromatin and eosinophilic cytoplasm (H and E, ×400)
Based on the histopathology findings, patient was put on anti-tubercular treatment. Chemotherapy was not started as it was a T2 tumor and patient was put on regular follow-up. Ultrasound abdomen done after 2 months showed absence of any lesions in the liver. Carcinoembryonic antigen done after 3 months of surgery was 1.2 ng/ml. Thus, the patient responded well to anti-tubercular treatment and is still continuing with the treatment.
DISCUSSION
Liver involvement in TB is seen both in pulmonary and extra-pulmonary TB. Three forms of hepatic TB are seen.[3] Most common is the diffuse hepatic involvement seen with pulmonary or miliary TB. The second form is diffuse hepatic infiltration without pulmonary involvement. Third and much rarer form is focal hepatic TB in the form of local tuberculoma or abscess.[4] Our case was also an example of the third form that is, focal hepatic TB with three nodular lesions seen in liver.
Incidence of isolated hepatic TB is estimated to be 0.3%.[5] It is rare due to low tension of hepatic oxygen which is unfavorable for the mycobacterial growth.[6] The clinical presentation of local hepatic TB do not have any pathognomonic picture. Abdominal pain, fever and weight loss are most commonly found.[7] Hepatomegaly is the most common finding present in 96% of the cases although it was not present in our case.[8] Liver function tests are nonspecific except for elevated alkaline phosphatase levels. It is not possible to diagnose hepatic TB on imaging as other focal lesions in the liver such as metastasis, and hepatocellular carcinoma can have a similar appearance.[9] Noninvasive diagnosis is, therefore, difficult, and up to 90% cases require laparotomy for definitive diagnosis as seen in our case too. The best method of diagnosis remains pathological examination of liver biopsy which will show characteristic caseating granulomas.[47] In a study by Landen et al. major hepatectomy was done in a colon cancer patient diagnosed with focal liver lesions presuming it to be colonic liver metastasis. However pathology revealed a benign tuberculous pseudotumor.[10] Our patient also showed numerous confluent epithelioid granulomas with caseation necrosis thus clinching the diagnosis of hepatic TB. AFB could not be demonstrated as was the case with other studies also.[1112]
Coexistence of abdominal TB and colon carcinoma though rare has been described.[13] The causal relationship between the two is still not clear. The possible mechanisms include reactivation of the dormant bacilli due to immunosuppression caused by cancer and derangement of host's intestinal mucosal barrier by underlying malignancy. However, coexistence of colon carcinoma with isolated hepatic TB is very rare and, therefore, no cause-effect relationship could be defined.
CONCLUSION
Isolated hepatic TB although uncommon should be included in the differential diagnosis of liver mass especially in areas endemic for TB. It can be confused with primary or metastatic carcinoma especially if associated with other malignancies. Coexistence of carcinoma colon and hepatic TB, although rare should be kept in mind especially in countries where TB is rampant.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Pancreatic tuberculosis with splenic tuberculosis mimicking advanced pancreatic cancer with splenic metastasizes: A case report. Cases J. 2008;1:84.
- [Google Scholar]
- Hepatic tuberculosis in absence of disseminated abdominal tuberculosis. Ann Hepatol. 2006;5:41-3.
- [Google Scholar]
- The nodular form of local hepatic tuberculosis. A review. J Clin Gastroenterol. 1990;12:166-73.
- [Google Scholar]
- Isolated hepatic tuberculosis: Report of five cases and review of the literature. J Hepatobiliary Pancreat Surg. 1999;6:195-8.
- [Google Scholar]
- Hepatic tuberculosis: Comparison of miliary and local form. Infection. 1995;23:5-8.
- [Google Scholar]
- The nodular form of hepatic tuberculosis: A review with five additional new cases. J Clin Pathol. 2003;56:835-9.
- [Google Scholar]
- Isolated giant tuberculomata of the liver detected by computed tomography. Gastrointest Radiol. 1989;14:305-7.
- [Google Scholar]
- Tuberculosis diagnosed after major hepatectomy for suspected malignancy. Acta Chir Belg. 2010;110:221-4.
- [Google Scholar]
- Hepatic granulomas: Profile and follow-up of 10 cases responding to antituberculous therapy. J Assoc Physicians India. 1987;35:207-9.
- [Google Scholar]
- Carcinoma colon associated with tuberculosis: An unusual presentation. Int J Colorectal Dis. 2007;22:843-4.
- [Google Scholar]



