
Translate this page into:
Internal Carotid Artery Fibromuscular Dysplasia in a Child: Incidental Postmortem Finding after Head Injury
Address for correspondence: Dr. Arulselvi Subramanian, E-mail: arulselvi.jpnatc@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Fibromuscular dysplasia (FMD) is a rare, segmental, nonatheromatous, and noninflammatory arterial disease of unknown etiology. It predominantly involves renal artery (60–75%) followed by extracranial part of the internal carotid artery and vertebral arteries (25–30%). The disease typically affects middle-aged women and involves intermediate-sized arteries throughout the body. There are rare case reports of extracranial FMD compounding a trauma case. A patient was brought to trauma center emergency with a history of fall from height. There were one previous episode of seizure and two episodes of vomiting. His Glasgow Coma Scale on admission was E1V1M4. Noncontrast computed tomography of the head showed fracture on the right zygomatic, temporal, and parietal bone, with underlying thin subdural hemorrhage. The patient underwent left frontotemporoparietal decompressive craniectomy and lax duraplasty with bone flap in bone bank. On the 1st postoperative day, he succumbed to his injuries despite timely surgery and necessary interventions. It was only postmortem when FMD was diagnosed in carotid artery by histopathological examination. On microscopy, intimal changes were seen in the form of expansion of subendothelial loose matrix with mesenchymal cells, thickening and hyalinization of the internal elastic lamina, areas of duplication and disruption of internal elastic lamina. Medial wall changes included thickening of the wall, focal loss of the smooth muscle, and replacement with fibrosis (dysplastic change). This case emphasizes the importance of considering this disease in the differential diagnosis of children and young adults with stroke (which subsequently lead to his fall).
Keywords
Carotid artery
fibromuscular dysplasia
trauma

INTRODUCTION
Fibromuscular dysplasia (FMD) is a rare, segmental, nonatheromatous, and noninflammatory arterial disease of unknown etiology. The disease typically affects middle-aged women and involves intermediate-sized arteries throughout the body. FMD not only is found predominantly within the renovascular (75%) and cerebrovascular (24%) systems but also has been reported in the mesenteric, iliac, and subclavian arteries. Although the disease can affect all three arterial wall layers, the media are involved in 90–95% of the cases. There are rare case reports of extracranial FMD compounding a trauma case. The present case describes a 5-year-old boy who fell from height and died due to widespread left cerebral ischemia. He succumbed to his injuries despite timely surgery and necessary interventions. It was only postmortem when FMD was diagnosed in carotid artery. This case emphasizes the importance of considering this disease in the differential diagnosis of children and young adults with stroke (which subsequently lead to his fall).
CASE REPORT
We report a case of carotid FMD in a 5-year-old child. The patient was brought to trauma center emergency with a history of fall from height. There were one episode of seizure and two episodes of vomiting. There was no history of any ENT bleed. On arrival, patient's Glasgow Coma Scale (GCS) was E1V1M4. Pulse and respiratory rate were within normal limits. Pupils were dilated and fixed. Extensor posturing was present. Noncontrast computed tomography (NCCT) of the head showed fracture on the right zygomatic, temporal, and parietal bone with underlying thin subdural hemorrhage. Cervical spine was however unremarkable. The patient was started on supportive treatment. His routine hematological and biochemical investigations were done. The patient underwent left frontotemporoparietal decompressive craniectomy and lax duraplasty with bone flap in bone bank. Postoperatively, the patient was shifted to the neuro-Intensive Care Unit on ventilatory support. However, unfortunately, patient developed ischemic changes in the left hemisphere. NCCT of the head showed diffuse infarct in the middle cerebral artery/anterior cerebral artery/posterior cerebral artery territory with upward herniation of the brain through craniotomy site, and diffuse edema was seen. His GCS fell to E1V1M1 with no spontaneous respiration and was declared dead on the 2nd postoperative day. Postmortem was done and the left internal carotid artery (ICA) was sent for pathological analysis after suspicious changes. Grossly, the left ICA was 9 cm in length and was covered externally with fibro-fatty tissue. On opening the artery along the length, the intimal wall was smooth. On microscopy, focal areas of intimal changes were seen in the form of expansion of subendothelial loose matrix with mesenchymal cells, thickening and hyalinization of the internal elastic lamina, areas of duplication and disruption of internal elastic lamina. Medial wall changes included thickening of the wall, focal loss of the smooth muscle, and replacement with fibrosis (dysplastic change) [Figures 1–4]. Angiographic findings were not available, but based on the relevant clinical history and supporting histopathological changes, we proposed the diagnosis of FMD with predominant intimal and medial dysplasia.
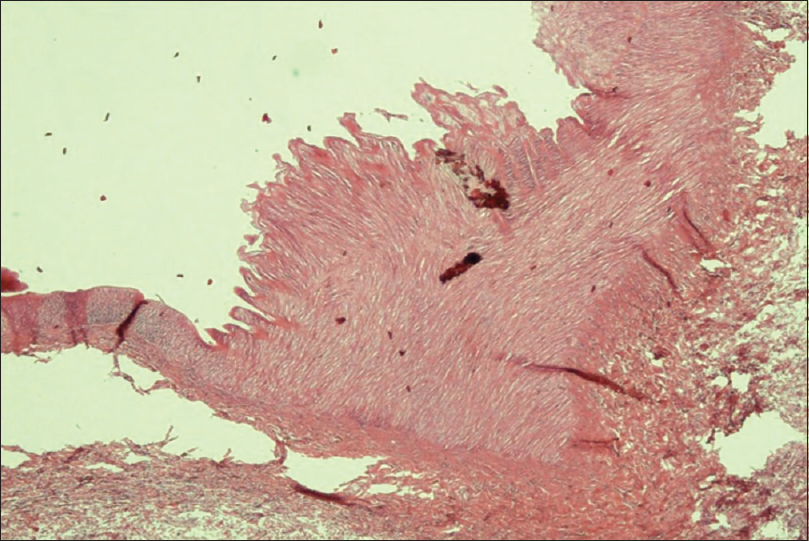
- Internal carotid artery wall showing alternate thinning (arrow) and thickening of the tunica media. Medial walls with fibrosis (dysplastic changes) (H and E, ×40)
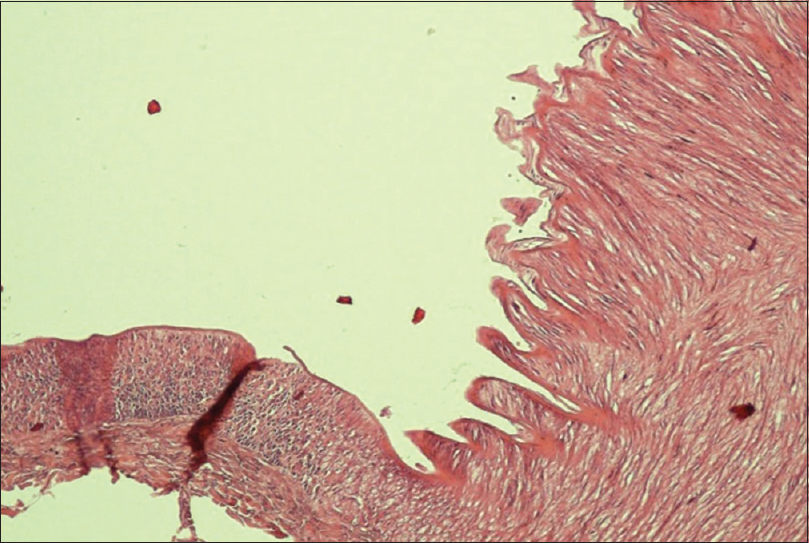
- Focal fence-like protrusions in the lumen of the artery (H and E, ×100)
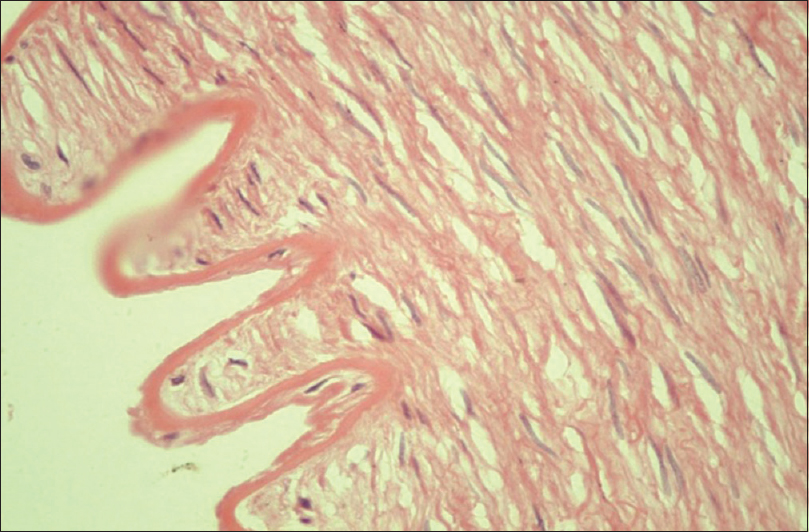
- Splitting of the internal elastic lamina (H and E, ×400)
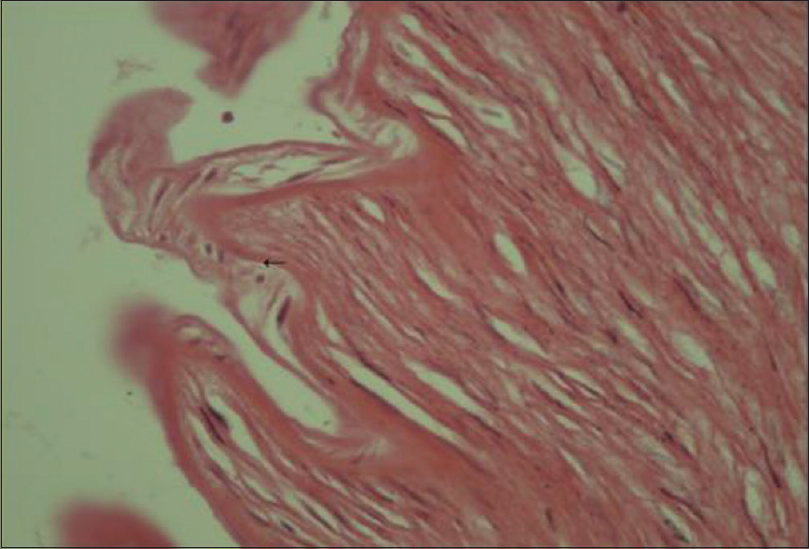
- Expansion of subendothelial loose matrix with mesenchymal cells, thickening and hyalinization of internal elastic lamina. H and E, ×400
DISCUSSION
FMD is a rare, nonatheromatous, and noninflammatory angiopathy of unknown etiology. FMD mainly affects the renal artery (60–75% of all cases) which usually manifests as renovascular hypertension, followed by the extracranial segments of the internal carotid and vertebral arteries (25–30% of all cases).[1] Cervical artery FMD, mainly affecting the ICA, is usually asymptomatic. It is discovered incidentally by Doppler ultrasound in patients worked up for dizziness, headache, or an asymptomatic cervical bruit. FMD lesions when complicated by brain ischemia, embolus, and thrombosis in cases with dissection or associated aneurysms rupture lead to neurological symptoms in the form of Horner's syndrome, transient ischemic attack, ischemic stroke, or subarachnoid hemorrhage.[2]
Familial occurrences of this disease have been reported in a few cases, and a Swedish study found an abundance of anomalies of the urinary tract, hypertension, or suspected otosclerosis in the families of patients with FMD. One-third of the patients studied had a family history among first-degree relatives (parents, siblings, or children) of stroke, hypertension, migraine, or impaired hearing. Other factors may play a role like microtrauma to the affected vessels, ischemia secondary to vasa vasorum occlusion, and ischemia and irritation causing cell mutation, and subsequent dysplastic lesions in the vessels. Further proposed etiologies which have not been substantiated include hormonal, metabolic, and immunological factors. The etiology remains unclear, but the multifactorial hypothesis including a congenital component seems reasonable. FMD is progressive in some cases so may start as a minor congenital lesion which predisposes the patient to a later abnormal fibroproliferative response to mechanical or circulatory stimuli.[3]
The first histologically proven case of carotid FMD was reported by Connett and Lansche in 1965. Histologically, the lesion is heterogeneous with various degrees of collagen hyperplasia, internal elastic lamina rupture, and disorganization of media layer. As pathological specimen is rarely received, the diagnosis is often made angiographically.[4]
FMD has been classified histologically into three types based on the primary site of involvement of arterial wall by McCormack et al. in 1967: Type 1 (85%): Medial fibroplasia, Type 2 (10%): Intimal fibroplasia with long tubular stenosis on angiography, and Type 3 (5%): Subadventitial fibroplasia of the arterial wall with asymmetric outpouching along one side of the ICA. The “string-of-beads” sign as seen on angiography is by far the most common and is pathognomonic for Type 1 FMD. Its pattern is explained by areas of luminal stenosis alternated with small fusiform or saccular aneurysms. The diameter of the “beads” is wider than the normal diameter of the artery at the level of involvement.[5] Correlations between different pathologically proven FMD subtypes and angiography have been established. For example, string-of-beads has been associated with medial fibroplasia/dysplasia and perimedial fibroplasia while tubular or focal stenosis has been correlated with medial hyperplasia, intimal fibroplasia, or adventitial hyperplasia.
Intimal fibroplasia characterized most pathologically proven cases of FMD with childhood stroke. Pathologically-proven FMD associated with childhood stroke is a unique syndrome, different from adult FMD, and lacking string-of-beads angiography. Accurately, labeling pediatric stroke patients as “FMD” based purely on intracranial angiographic features are not possible given current knowledge. Until better biomarkers of FMD are identified, pathological confirmation remains the only means by which FMD can be confirmed.
Stroke in children and young adults is uncommon. At least one-third of childhood strokes have no clear etiology. The most frequently noted etiology for childhood stroke is cardiac malformation, followed by sickle cell disease, coagulopathies, metabolic derangements, and infectious processes. FMD should additionally be considered in this differential.[6] In our case, all investigations were negative.
In literature, only one medicolegal case report was published, in which FMD of the basilar artery was identified in a victim of road traffic accident and the pathological finding was correlated with cause of the accident.[1] In our case also, we correlated the circumstances under which the patient fall from the height, i.e., loss of consciousness, with the histopathologically proved FMD. In the current case, we did not found any gross or microscopic secondary lesions which usually lead to manifestation in the disease.
CONCLUSION
Even in the traumatic cases where the cause of death is severe injuries, one should consider the circumstantial events and always rule out the vascular pathologies as FMD in this case.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We thank Prashant Ramteke, Roopam Deka (SR's Lab Medicine), Jasbir Singh (SR, Forensic medicine), Lian, Meenakshi, and Renu (Lab Technicians) for help and assistance in processing and diagnosis.
REFERENCES
- Fibromuscular dysplasia of the basilar artery: An unusual case with medico-legal implications. Forensic Sci Int. 2007;173:188-92.
- [Google Scholar]
- Childhood ischemic stroke caused by fibromuscular dysplasia of the intracranial artery – Case report. Neurol Med Chir (Tokyo). 1997;37:542-5.
- [Google Scholar]
- Fibromuscular hyperplasia of the internal carotid artery: Report of a case. Ann Surg. 1965;162:59-62.
- [Google Scholar]
- Isolated intracranial fibromuscular dysplasia presents as stroke in a 19-year-old female. Arq Neuropsiquiatr. 2005;63:318-20.
- [Google Scholar]



