
Translate this page into:
Invasive mixed fungal disease after covid-19: A series of seven cases
*Corresponding author: Vaishali A. Walke, MD, Professor, Department of Pathology Lab Medicine, Medical College Building, First Floor, All India Institute of Medical Sciences, Saket Nagar, Bhopal, Madhya Pradesh, 462020, India vaishali.patho@aiimsbhopal.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Walke VA, Jayashankar E, Karuna T, Chourasia JK, Panwar H, Kapoor N, et al. Invasive mixed fungal disease after covid-19: A series of seven cases. J Lab Physicians. 2024;16:228-35. doi: 10.1055/s-0043-1770699
Abstract
Coronavirus disease 2019 (COVID-19) is a recent global pandemic that is caused by the novel severe acute respiratory syndrome coronavirus 2. The patients of covid-19 are susceptible to a diverse range of secondary infections, fungal being the most common. The increased risk is proposed to be due to the generous use of steroids for the treatment of COVID-19 infection and the presence of comorbidities, such as diabetes mellitus, hypertension, preexisting lung diseases, and/or old age. Invasive mixed fungal disease is potentially life-threatening to the patients of COVID-19. In the present series of seven cases, the authors intend to discuss the clinicopathological profile and gamut of histopathological findings in invasive mixed fungal infection comprising of mucor and Aspergillus in treated patients of COVID-19. Six patients had a clinical diagnosis of sinonasal–orbital invasive fungal disease, while there was a case of lung infection. The acquaintance and knowledge about histomorphology of invasive fungi and the multidisciplinary diagnostic approach not only will aid in early and accurate diagnosis but can guide the clinician for necessary surgical intervention and initiation of appropriate antifungal medications in patients of COVID-19.
Keywords
mixed fungal infection
Aspergillosis
Mucormycosis
COVID-19

INTRODUCTION
Coronavirus disease 2019 (COVID-19) is considered to be the most dreaded infection encountered recently by the world.[1] The transmission is potentially through the respiratory route with the lungs being the primary focus, resulting in severe acute respiratory distress syndromes. Additionally, immunosuppression due to varied reasons makes these patients more susceptible to a diverse range of secondary infections, fungal infections being the most common that are associatedwith increased morbidity.[2,3] Moreover, corticosteroids administered to modulate inflammation-mediated lung injury also increase the risk, particularly for systemic fungal coinfections such as Candidiasis, Aspergillosis, and Mucormycosis.[4,5] Mucormycosis, a subtype of Zygomycosis, presents with high morbidity and is commonly noticed in treated patients of COVID-19 and was responsible for approximately 28,200 new cases, and the symptoms included, blurred vision, redness of the eye, nasal blockage or discharge, and local pain to blackish discoloration of nose and palate.[6,7] The dual nature of invasive fungal infections in these patients is uncommon with only a few case series and reports documented in the literature.[8–10] In this study, authors intend to discuss the clinicopathological profile of dual fungal disease comprising of Mucormycosis and Aspergillosis in known and treated patients of COVID-19.
CASE SERIES
A total of 57 clinically suspected patients of COVID-19-associated invasive fungal disease were reported during a period of 3 months from April 2021 to June 2021 to the histopathology lab for tissue diagnosis. Out of these 45 cases revealed histopathological evidence of Mucormycosis alone, while 7 showed the presence of dual fungal disease and the remaining 12 were negative for fungal elements on histology. Six patients presented with signs and symptoms of sinonasal– orbital cellulitis, while one had respiratory symptoms that are included in the current study. The imaging findings in all these seven cases favored the possibility of invasive fungal disease. The surgical procedures performed were endoscopic exenteration in six and lobectomy in one patient. Upon receipt in the surgical pathology laboratory, the specimens were processed as per the protocol and representative sections were stained with hematoxylin and eosin (H&E) and special stains such as Gomori methenamine silver (GMS) and periodic acid Schiff (PAS). The detailed clinical information pertaining to the individual cases were described below:
Case 1
A 49-year-old male patient was clinically diagnosed as post-COVID-19 rhino-orbital Mucormycosis. For COVID-19, he received Dexamethasone with a tapering dose in addition to antibiotics and supportive care for a period of 1 week and had a hospital stay for 7 days. He was a known case of diabetes mellitus (DM), and the patient was taking oral antidiabetic medications for the last 10 years. After a period of 2 weeks of post-COVID-19 illness, the patient developed signs and symptoms of rhino-orbital sinusitis and was admitted for further management. Considering Mucormycosis as etiology, the patient was put on injectable amphotericin B and endoscopic exenteration was planned. The fresh tissue was sent for mycology evaluation, while for histopathology, the specimen was received in 10% formalin. The potassium hydroxide (KOH) preparation revealed an admixture of both broad, aseptate hyphae and narrow septate hyphae. The probable diagnosis of mixed fungal infection was made and the remaining specimen was processed for culture examination. With the diagnosis of mixed fungal infection, Mucor and Aspergillus, the patient was put on another antifungal drug voriconazole.
Case 2
A 66-year-old male known diabetic patient was admitted with signs and symptoms of rhino-orbital sinusitis in the form of headache and orbital pain. He received treatment for COVID-19 in the form of intravenous steroids and oxygen supplementation during 2 weeks of hospital stay. Endoscopic exenteration was performed and KOH preparation on the fresh tissue sample yielded broad, aseptate, hyphae suggesting Mucor along with hyaline, septate hyphae favoring hyalohyphomycosis. On initial presentation, the infection was already involving the orbit; subsequently, the disease spread to the brain and the patient developed signs of meningitis during the course of the disease. The patient, later on, succumbed to his infection in spite of combined surgical and medical line of management.
Case 3
A 45-year-old male patient was referred to the hospital with headache and facial pain associated with swelling. He was diagnosed with post-COVID-19 rhinosinusitis possibly of Mucor origin. The past history revealed his 1 week hospitalization for COVID-19 and received steroids as a part of treatment. The history of comorbid factors such as DM could not be elicited. The nasal crusting sample sent for direct microscopy revealed broad, aseptate fungal hyphae with right-angle branching suggested the possibility of Mucor. The patient was started with the antifungal medication tablet posaconazole. The endoscopic exenteration performed and the specimen was sent for both mycological and histological examination. The culture in this case could isolate only Rhizopus arrhizus species.
Case 4
An elderly 79-year-old male patient was admitted with a clinical diagnosis of post-COVID-19 rhino-orbital Mucormycosis. The patient received treatment for COVID-19 in the form of steroids, antibiotics, and oxygen for 1 week. After around a period of 8 weeks, the patient developed signs and symptoms of rhinosinusitis. He was a known diabetic and was put on oral antidiabetic medications for the last 28 years. The sinonasal endoscopic surgical procedure was planned and the tissue removed was submitted in a fresh state of saline for mycology and in 10% formalin for histopathology for further workup. The KOH preparation yielded thin-walled, aseptate, fungal elements favoring Mucor. The culture was not possible in this case as the specimen submitted for microbiology was scant and only direct microscopy could be performed as no tissue was left for the culture correlation.
Case 5
A 46-year-old male patient had signs and symptoms of rhino-orbital sinusitis for which he visited the hospital. He narrated the past treatment for COVID-19 around 6 to 8 weeks ago, in the form of corticosteroids, antibiotics and oxygen support, and hospitalization for a week. There was no history of comorbid conditions including DM. The patient was admitted for bilateral sinonasal exenteration and polypectomy. The fresh tissue sample processed in the mycology laboratory did not yield evidence of fungal infection either on direct microscopy or on culture; histopathology, however revealed features of invasive mixed fungal infection.
Case 6
A 39-year-old male patient was clinical radiologically diagnosed with bilateral rhino-orbital Mucormycosis. The detailed history revealed symptoms of facial pain, watery discharge, and nasal obstruction which he developed around 6 to 7 weeks after his recovery from COVID-19. For COVID-19, he received corticosteroids, and antibiotics as per the treatment protocol. The surgical management was planned as sinonasal endoscopic exenteration. The KOH preparation from fresh tissue sample displayed, dual fungal morphology comprising of broad, aseptate hyphae with right angle branching favoring Mucor and hyaline, septate hyphae with acute angle branching favoring Aspergillus. The culture on Saboraud dextrose agar (SDA) revealed Aspergillus flavus and Rhizopus arrhizus species.
Case 7
A 45-year-old patient presented with complaints of progressive breathlessness, heaviness in the chest with pain. The patient had a history of COVID-19 infection 2 months back and received treatment as steroids, antibiotics, and oxygen support for a period of one week. Contrast-enhanced computed tomography (CT) scan revealed area of consolidation in right lower lobe with cavitation measuring 7.7 × 6.2 × 6.0 possessing thick irregular walls. There was evidence of bronchopulmonary fibrosis and hydropneumothorax. The Monteux test and sputum for acid-fast Bacillus were also negative. Due to patients exacerbating symptoms, the surgical intervention in the form of lobectomy of right lung was performed. The histopathology showed a cavitary disease with a large area of necrosis with the peripheral zone of inflammation along with presence of broad, thin-walled, aseptate hyphae showing right angle branching suggestive of Mucor admixed with, thick-walled, septate hyphae having acute angle branching suggestive of Aspergillus. The adjacent tissue showed giant cell reaction and acute inflammation in lung parenchyma with fibrosis. The patient was treated with antifungal drugs and follow-up was uneventful till 6 months. As there was no clinical suspicion of fungal infection, the mycological evaluation could not be carried out.
This study composed of seven male patients who belonged to the age range of 39 to 79 years, with majority being in fifties. The association with comorbidities like DM was observed in 42.85% (3/7; Table 1) The period of hospital admission for COVID-19 ranged from 7 to 14 days, and most (6/7) received treatment in the form of steroids, antibiotics, and oxygen support with reference to the patient’s clinical condition and COVID-19 management protocol. One patient (case 7) presented with respiratory symptoms and admitted with clinicoradiological diagnosis of pulmonary cavitary disease. Histopathological examination of tissue samples received in all the seven cases revealed presence of fungal organisms comprising of Mucormycosis (Mucorales) and Aspergillosis (Figure 1A). In tissue sections, Mucor exhibited morphology as thin-walled, broad, aseptate, irregular hyphae, with right angle branching (Figure 1B), while Aspergillus displayed narrow, septate hyphae with acute angle branching, highlighted in GMS and PAS stain (Figure 1C). The fungal elements were seen embedded in variable amount of necrosis as observed in all the seven cases. The tissue response ranged from suppurative inflammation, necrotizing granulomas, angioinvasion, angiodestruction, and neural invasion (Figure 1D). The commonest reaction pattern was suppurative inflammation noted in 71% (5/7), fibrin thrombi in 57% (4/7) followed by necrotizing granulomas in 28% (2/7; Table 1) The KOH preparation, performed in six out of seven patients, revealed fungal organisms with dual morphology in only three cases (Figure 2A), while only Mucorales were identified in another two cases and no organisms in a single case. The fungal culture on SDA with chloramphenicol was possible in five, and revealed Mucorales (Rhizopus arrhizus) as sole organism in two, while mixed organisms like Aspergillus flavus with Rhizopus arrhizus were isolated also in two and no organisms could be isolated in one case (Figure 2B) The smears subsequently prepared from the growth using lactophenol cotton blue preparation highlighted mixed fungal organisms (Figure C and D).
| No | Age/Sex | Clinical history | Radiological Findings (CT/MRI) |
History of comorbidity | Treatment of fungal infection | Key histological features | Microbiological profile | Outcome | |
|---|---|---|---|---|---|---|---|---|---|
| KOH | Culture | ||||||||
| 1 | 49/M | Bilateral nasal discharge, congestion, heaviness of face, headache, facial pain | Pansinusitis and leptomeninges enhancement premaxillary region involvement | DM and steroid for COVID-19 | Surgical exenteration and amphotericin B and voriconazole | Necrosis, Suppurative inflammation angioinvasion and angiodestruction | Aseptate, right angle branched hyphae and hyaline, septate, with acute angle branched hyphae | Aspergillus flavus and Rhizopus arrhizus | Doing well |
| 2 | 66/M | Bilateral nasal discharge, congestion, swelling of nose, eye pain | B/L max sinusitis (nasal/orbital) | DM and steroids for COVID-19 | Surgical exenteration with amphotericin B and voriconazole | Necrosis, with angioinvasion and angiodestruction | Mucor and Aspergillus organism |
Rhizopus arrhizus | Succumbed to illness |
| 3 | 45/M | Head ache, facial pain | Left sinusitis | No history of comorbid factors | Surgical exenteration, with amphotericin B and voriconazole | Necrosis, Suppurative inflammation angioinvasion and angiodestruction | Only Mucorales | Rhizopus arrhizus | Doing well |
| 4 | 79/M | Nasal discharge, congestion, pain in eye & cheek region | B/L max sinusitis, (nasal/orbital) | History of DM and Steroid intake for COVID-19 | Surgical exenteration, with amphotericin B and voriconazole | Necrosis, granulomatous inflammation, angioinvasion and angiodestruction | Only Mucorales | Not done | Doing well |
| 5 | 46/M | Nasal discharge, congestion, headache | Bilateral sinusitis | No History of DM; received steroids for COVID-19 | Surgical exenteration, with amphotericin B | Necrosis and suppurative inflammation | No fungal elements seen | Not done | Doing well |
| 6 | 39/M | Nasal discharge, congestion, facial pain, abnormal protrusion of eye with difficulties in vision | Bilateral sinusitis, right eye proptosis | No history of DM; received steroids for COVID-19 | Surgery with antifungal medication | Necrosis, granulomatous inflammation | Mucor and Aspergillus organism | Aspergillus flavus and Rhizopus arrhizus | Doing well |
| 7 | 45/M | Facial pain, nasal discharge, congestion, difficulty in breathing. | Bilateral sinusitis Right lung cavitary lesion in middle lobe | No history of DM; received steroids for COVID-19 | Pneumonectomy with post op amphotericin B and voriconazole | Necrosis, suppurative inflammation, angioinvasion and angiodestruction | Not done | Not done | Doing well |
Abbreviations: COVID-19, coronavirus disease 2019; CT, computed tomography; DM, diabetes mellitus; KOH, potassium hydroxide; MRI, magnetic resonance imaging.
![(A) Invasive mixed fungal infection comprising of colonies of both Mucormycosis and Aspergillosis (hematoxylin and eosin [H&E]; 10X). (B) Mucormycosis: The fungal organisms display thin walled, broad, aseptate, right angle branched hyphae, embedded in areas of necrosis (H&E stain; 20X). (C) Aspergillosis: The fungal elements forming colonies and displaying narrow, septate, acute angled branched hyphae (Gomori methenamine silver stain; 20X). (D) The Mucor hyphae exhibiting property of angiodestruction and angioinvasion with surrounding area of necrosis (periodic acid Schiff stain; 20X).](/content/164/2024/16/2/img/JLP-16-228-g001.png)
- (A) Invasive mixed fungal infection comprising of colonies of both Mucormycosis and Aspergillosis (hematoxylin and eosin [H&E]; 10X). (B) Mucormycosis: The fungal organisms display thin walled, broad, aseptate, right angle branched hyphae, embedded in areas of necrosis (H&E stain; 20X). (C) Aspergillosis: The fungal elements forming colonies and displaying narrow, septate, acute angled branched hyphae (Gomori methenamine silver stain; 20X). (D) The Mucor hyphae exhibiting property of angiodestruction and angioinvasion with surrounding area of necrosis (periodic acid Schiff stain; 20X).
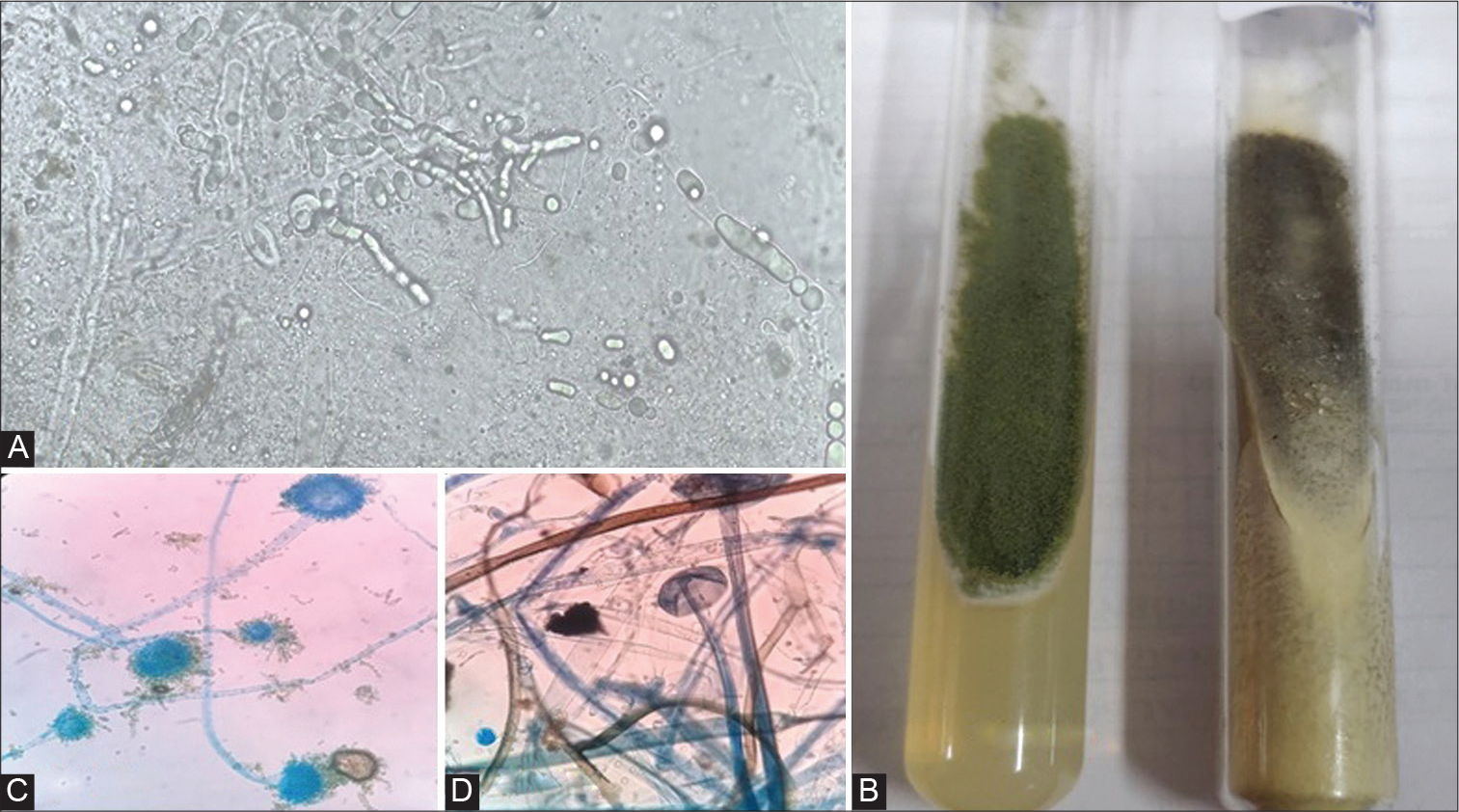
- (A) Potassium hydroxide preparation displaying hyaline, septate acute angle branched hyphae of Aspergillus flavus and thin walled, broad, aseptate hyphae of Rhizopus arrhizus (40X). (B) Growth on Saboraud dextrose agar medium with chloramphenicol: left tube (Green) representing Aspergillus flavus and right tube (black) represents Rhizopus arrhizus. (C) Smears prepared from culture growth stained with lactophenol cotton blue revealed morphology of Aspergillus flavus (40X). (D) Smears prepared from culture growth stained with lactophenol cotton blue revealed morphology of Rhizopus arrhizus (40X).
DISCUSSION
The rise in the global incidence of opportunistic fungal infections during the COVID-19 second wave was phenomenal, especially in India. The attributable factors include high incidence of DM, environmental conditions, and unregulated steroid use for treating COVID-19.[8] Radotra and Challa in their review quoted that hyperglycemia, acidosis, availability of free iron, lowered host defenses, and fungal virulence were the factors that promoted the growth of Mucorales.[11] The COVID-19 treatment modality might have resulted in dysregulation of the glycemic control and predisposition to secondary fungal infections, especially in the setting of comorbid factors like DM. Amalanathan et al reported a case of Mucormycosis that presented as orbital cellulitis in a patient of COVID-19 pneumonia with steroid dependence and uncontrolled DM.[7] Singh et al studied fungal infections among COVID-19 patients over a 1-month period and observed 10 cases of mixed fungal disease. DM as a comorbid factor was evident in all their patients and all were treated with steroids as per protocol.[9] In the present series of seven cases, association with DM was evident in 42% (3/7), while 85% (6/7) received steroids as per the treatment protocol. El-Kholy et al studied 36 patients with acute invasive fungal rhinosinusitis and reported Mucor in 77.8% and Aspergillus in 30.6% of patients who had sinonasal, orbital, cerebral, and palatine involvement in 100, 80.6, 27.8, and 33.3%, respectively.[1] In this study, the incidence of mixed infection was 15% (7/47) of Aspergillus and Mucor species and most patients presented with facial pain, numbness, headache, ophthalmoplegia, blackish discoloration, and crusting of nasal mucosa, while diminution of vision and features of orbital cellulitis was noticed in a single case. The clinical manifestations of COVID-19 were mainly due to the activation of immuneregulatory cytokines affecting the multi-organ system in response to cytokine storm. The pathogenesis of fungal infection in COVID-19 is multifactorial and can also be less sensitive, but diagnostic) was confirmatory for the diagnosis of invasive fungal disease.[11] The tissue diagnosis of fungal disease was even more challenging, particularly in conventional H&E stains. In suspected cases, additional histochemical stains like GMS or PAS need to be applied for better visualization of fungi admixed with a gamut of tissue reaction patterns and can augment and aid pathologist for its early diagnosis. The other modalities proposed for the identification of fungi are diagnostic biomarkers that can help clinicians in the early diagnosis of suspected individuals. The molecular platform proposed was polymerase chain reaction (PCR) studies for Mucorales. Tools such as screening assays for Aspergillosis using serum galactomannan and 1,3 β-d-glucan antigens may also be more useful in high-risk cases.[8] The definition of acute invasive fungal rhinosinusitis included the presence of tissue invasion by fungal elements with a clinical course of 4 to 6 weeks.[12] The disease progresses quickly resulting in vascular invasion and thrombosis. Mixed invasive fungal infection consisting of Mucormycosis and Aspergillosis was diagnosed on histopathology in all seven cases. These opportunistic fungi can also cause systemic mycosis in immunocompromised hosts and can involve nasal cavity, paranasal sinuses, lung, orbit, brain and may turn out to be lethal.[7] The dual invasive fungal infections can become more aggressive, leading to high morbidity and mortality, when associated with comorbid factors.[13] Fungal infection is considered, one of the important causes of death in approximately 25 to 73.7% of post COVID-19 patients.[12] The invasive fungal disease may exhibit a gamut of tissue reactions such as necrotizing to chronic granulomatous to suppurative inflammation. In present series, the most consistent histopathology feature in all seven cases was presence of varying amounts of necrosis attributed to the angioinvasion and angiodestruction property of Mucorales. The variable density of fungal hyphae was seen embedded in the necrosis and displayed admixture of both broad, aseptate, thin-walled hyphae favoring Mucor and Aspergillus exhibiting narrow, septate, acute angled, and pigmented fungal elements. The morphology was well appreciated on special stains such as PAS and GMS. It can be inferred and emphasized that the necrotic tissue must be sampled thoroughly so as to identify these fungal organisms. The study conducted by Mohapatra et al revealed seven (5.3%) patients of mixed fungal infections among 150 suspected cases of post-COVID-19 Mucormycosis. The mixed infection exhibited as fruiting bodies of Aspergillus and hyphae of Mucorales and the granulomatous inflammatory reaction was noticed in two out of a total of seven cases. They inferred that the presence of Aspergillus fruiting bodies can be considered as a tell-tale sign of mixed infection in clinically suspected cases of post COVID-19 Mucormycosis.[8]
The direct microscopy that was possible in six out of seven patients in the present study revealed mixed fungal organisms in three Mucorales alone observed in another three cases (Table 1). The fungal culture was processed in five patients, displayed isolates of both Aspergillus flavus and Rhizopus arrhizus in two, single isolates of Mucorales in another two, and no organisms could be isolated in one patient. The culture examination was not done in two patients. The study of Singh et al, in their series of 10 cases, revealed growth of Rhizopus arrhizus with Aspergillus flavus in seven, while Aspergillus fumigatus with Mucorales was noted in three patients.[9] Paul et al, in their 2 months’ retrospective study of 70 cases, observed 12 patients of invasive mixed fungal disease, in the form of thin-walled aseptate hyphae favoring Mucor and narrow hyaline septate hyphae with acute angle branching suggesting Aspergillus on KOH findings. The culture examination in their study confirmed isolates of mixed infection in six, Aspergillus alone in four, and no growth in two patients. The histopathology could successfully identify mixed infection in 2 out of 12 cases, Mucor alone in nine, and no organism could be identified in one case. All their patients had DM as an associated comorbid condition and were treated with systemic liposomal amphotericin B and surgical debridement.[14]
Rai and Kumar reported a case of dual pulmonary invasive fungal infection comprising of Aspergillus and Mucor in COVID-19 patients; the imaging findings were highly suggestive of post-COVID-19 pulmonary fungal disease. The diagnosis was confirmed by the galactomannan antigen test for Aspergillus and PCR for Mucorales on bronchoalveolar avage fluid.[10] Fekkar et al identified seven (4.8%) cases of pulmonary fungal infection, in COVID-19 and they linked them with high mortality.[15] Benhadid-Bhrahmi et al reported a case of a previously immunocompetent patient with severe acute respiratory syndrome coronavirus 2 infection, complicated during the disease course with pulmonary Aspergillosis and Mucormycosis coinfection.[16] A case reported by Mohanty et al had a fungal storm with Aspergillosis and Mucormycosis and superadded Klebsiella in a post COVID-19 patient. She was initially treated with voriconazole and later switched to liposomal amphotericin B when the diagnosis of mixed fungal disease was confirmed, along with antibiotics, surgical debridement, with supportive care. Their patient improved after a long stay in the hospital and was doing well[17] (Table 2). In the present series, dual fungal infection was detected in seven cases (15%). Six had features of sinonasal infection, while there was a single case of pulmonary mixed fungal disease. The treatment of fungal disease was also challenging for dual etiology and needed utmost care because Aspergillus infection is known for metastatic spread and required medical management where voriconazole was the mainstay of treatment, while Mucormycosis a locally invasive pathogen required surgical management supplemented with amphotericin-B. All the patients in the present series were treated with a combination of drugs such as amphotericin-B and voriconazole along with surgical debridement. There was a single patient (case 2) who was diagnosed on the 10th day of admission and in spite of the initiation of treatment he could not be saved, reflecting the necessity for prompt and timely diagnosis; remaining six all patients were doing well till the last follow up.
| S no |
Authors | No cases | Comorbidities | Treatment (steroid) | Clinical findings | Histopathology | Microbiological isolates | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | El-Kholy et al[1] |
3 | DM, HT, malignancy |
Yes | Facial pain, numbness and swelling, headache, skin ulceration | Aspergillus and Mucormycosis in all 3 cases | NM | Not detailed about individual case |
| 2 | Mohapatra et al[8] | 7 | NM | NM | NM | Aspergillus and Mucormycosis | Types of isolates not specified | NM |
| 3 | Singh et al[9] | 10 | DM (7/7) | Yes (7/10) | Rhizopus arrhizus mixed with Aspergillus flavus in 7 and Aspergillus fumigatus in 3 cases | |||
| 4 | Rai and Kumar[10] | 1 | DM | Yes | Chest pain, cough, dyspnea on exertion, and generalized weakness | Not done | KOH: Septate fungal hyphae in nasal crust and positive galactomannan antigen test in serum and BAL fluid Positive PCR— Mucorales species in BAL | Succumbed to illness |
| 5 | Paul et al[1] | 12 | DM 12/12 | 9/12 | Facial pain swelling, loss of vision, palatal ulcer, nasal congestion | Culture: mixed organism in 6/12 Single isolates 4/12, Negative in 2/12 | 2/12 died of disease | |
| 6 | Benhadid- Brahmi et al[16] |
Single case pulmonary COVID-19 | Treated case of gastric lymphoma, non-DM | Yes | Cough and a fever X 4 days & progressed to respiratory distress | Not done | BAL fluid KOH: Aspergillus and Mucorales -type mycelium Culture: Rhizopus delemar, Aspergillus welwitschia |
Succumbed to disease |
| 7 | Mohanty et al[17] |
Case report | DM | No | Swelling in cheek with pain and redness & black nasal discharge X 5-6 days | Mucor only | KOH and lactophenol blue: Nasal endoscopic tissue Aspergillus and Mucor. Culture: NM | Doing well |
| 8 | Present study | 7 (6 Sinonasal– orbital and 1 lung) |
DM in 3/7 | All pts | Facial pain, numbness and swelling, loss of vision, nasal congestion, discharge, skin ulceration |
Aspergillus and Mucormycosis in all 7 cases | KOH mount: 3/6 mixed, Mucorales in only 2, no organism in 1 Culture: 2 cases isolates of mixed Rhizopus arrhizus and Aspergillus flavus, two only Rhizopus arrhizus, one no isolates and in two culture not done |
1 out of 7 died of disease |
Abbreviations: BAL, bronchoalveolar lavage; COVID-19, coronavirus disease 2019; DM, diabetes mellitus; HT, hypertension; KOH, potassium hydroxide; NM, not mentioned.
Limitations
The selection criteria of mixed invasive fungal disease in present series of cases, even though, were based on histopathology findings, the identification of growth in all corresponding culture examination as mixed disease on a single occasion was not possible and was one of the limitations of our study.
CONCLUSIONS
Despite the risk of fatality associated with mixed fungal infection in post COVID-19 patients, acquaintance and knowledge about morphology and multidisciplinary comprehensive diagnostic approach may not only aid in the reduction of disease-associated mortality but also provide a timely diagnosis to initiate specific and prompt treatment. The mixed fungal disease may be under-reported; hence, awareness about the possibility of dual nature and associated risk factors may aid in early identification, prevention, and better patient’s outcome.
Abbreviations
DM Diabetes Mallitus
GMS Gomoris Methanamine Silver;
H&E Hematoxylin and Eosin
KOH Potassium Hydroxide;
PAS Periodic Acid Schiff ’s
SDA Saborauds Dextrose Acetate
Conflict of Interest
None declared.
References
- Invasive fungal sinusi-tis in post COVID-19 patients: a new clinical entity. Laryngoscope. 2021;131:2652-2658.
- [CrossRef] [PubMed] [Google Scholar]
- A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579:270-273.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): a multi-center study in Wenzhou city, Zhejiang, China. J Infect. 2020;80:388-393.
- [CrossRef] [PubMed] [Google Scholar]
- Invasive paranasal mucormycosis with peripheral eosinophilia in an immunocompetent patient. Med Mycol. 2010;48:406-409.
- [CrossRef] [PubMed] [Google Scholar]
- Sinoorbital mucormycosis in a COVID-19 patient: a case report. Int J Surg Case Rep. 2021;82:105957.
- [CrossRef] [PubMed] [Google Scholar]
- Fungal co-infections associated with global COVID-19 pandemic: a clinical and diagnostic perspective from China. Mycopathologia. 2020;185:599-606.
- [CrossRef] [PubMed] [Google Scholar]
- Mucormycosis complicating diabetes mellitus and COVID-19: a diagnostic and therapeutic threat. Inter J Otorhinolaryngology & Head and Neck Surgery. 2021;7:679.
- [CrossRef] [Google Scholar]
- Incidence of mixed fungal infections in post-COVID-19 outbreak of Mucormycosis India. Med Mycol. 2022;???:60.
- [CrossRef] [Google Scholar]
- Mixed invasive fungal infections among COVID-19 patients. Curr Med Mycol. 2021;7:19-27.
- [CrossRef] [Google Scholar]
- Dual invasive fungal infection by Aspergillus and Mucor in COVID-19 patient: a rare case report with literature review. Arch Med Health Sci. 2021;9:278-282.
- [CrossRef] [Google Scholar]
- Pathogenesis and pathology of COVID-associated Mucormycosis: what is new and why. Curr Fungal Infect Rep. 2022;16:206-220.
- [CrossRef] [PubMed] [Google Scholar]
- Post Covid-19 infection presenting as rhino-orbital mycosis. Indian J Otolaryngol Head Neck Surg. 2021;14:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- Strategy of following voriconazole versus amphotericin B therapy with other licensed antifungal therapy for primary treatment of invasive aspergillosis: impact of other therapies on outcome. Clin Infect Dis. 2005;41:1448-1452.
- [CrossRef] [PubMed] [Google Scholar]
- Invasive Mucormycosis and Aspergillosis coinfection in post COVID-19 pneumonia in a tertiary care hospital. Med Mycol J. 2022;63:59-64.
- [CrossRef] [PubMed] [Google Scholar]
- Occurrence of invasive pulmonary fungal infections in patients with severe COVID-19 admitted to the ICU. Am J Respir Crit Care Med. 2021;203:307-317.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19-associated mixed mold infection: a case report of aspergillosis and mucormycosis and a literature review. J Mycol Med. 2022;32:101231.
- [CrossRef] [PubMed] [Google Scholar]
- Mucormycosis and aspergillosis: the deadly duo in COVID-19-a case report. J Family Med Prim Care. 2022;11:6529-6532.
- [CrossRef] [PubMed] [Google Scholar]



