
Translate this page into:
Microbiological profile and antibiotic resistance pattern of skin and soft-tissue infections: A study from Northern India
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
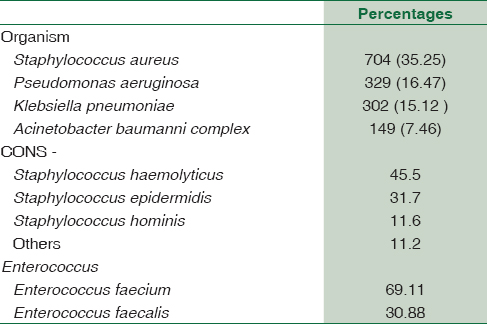
Skin and soft-tissue infections (SSTIs) require wise choice of antimicrobials in addition to aggressive surgical intervention to limit tissue loss and preserve life.[1] The aim of this study was to determine the microbiological profile and antibiotic susceptibility patterns of organisms isolated from SSTIs in our hospital. We studied 4551 consecutive pus samples collected from both inpatients and outpatients of our hospital from January 1, 2017, to December 31, 2017. All isolates were identified by matrix-assisted laser desorption ionization time of flight mass spectrometry using the bioMérieux VITEK MS system (IVD database version 2.0) (Cambridge, Boston, USA) and susceptibility by disc diffusion method.[2] Of the 1997 bacterial isolates, 772 (38.65%) were gram-positive cocci and 1225 (61.34%) gram-negative bacilli. The most common pathogen isolated was shown in Table 1. Extended-spectrum beta-lactamase (ESBL) production was observed in 819 (66.85%) isolates, and it was highest in Escherichia coli (44.08%). Resistance to methicillin was detected in 24.18% of Staphylococcus aureus isolates and 13.94% CoNS. High proportion 71.64% of isolates exhibited HLARG. High rates of ESBL production (66.85%) and methicillin resistance were noted, which is comparable to previous studies from India.[34] More than half (71.64%) of the enterococcal isolates were HLARG, with the implication that the combination of beta-lactam plus aminoglycoside will not be active against them. Therefore, there is need of monitoring of resistance pattern of enterococci. The high rates of antibiotic resistance observed in the present study may be due to the fact that ours is a tertiary care hospital with wide use of broad-spectrum antibiotics leading to selective survival advantage of isolates and lack of definite antibiotic policy. This is reinforced by the fact that in a previous study from our institute, similar high rates of methicillin-resistant S. aureus (38.56%), ESBL production (66.75%), and HLARG (53.3%) were reported in SSTI's.[5] There is need for continued monitoring of susceptibility pattern in individual settings to prevent their further emergence by misuse of drugs.
Limitations of our study are retrospective study and collection of data from single-center only. To conclude, there is need for strategic, coordinated, and sustained infection prevention and control measures to combat these superbugs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Necrotising infections of soft tissues – A clinical profile. Eur J Surg. 2002;168:366-71.
- [Google Scholar]
- Performance Standards for Antimicrobial Susceptibility Testing (26th ed). Wayne PA: CLSI; 2016.
- Ciprofloxacin in the management of soft tissue infections in diabetes mellitus. J Assoc Physicians India. 2000;48:757-8.
- [Google Scholar]
- Methicillin resistance among isolates of Staphylococcus aureus: Antibiotic sensitivity pattern & phage typing. Indian J Med Sci. 2002;56:330-4.
- [Google Scholar]
- Bacteriological and antimicrobial susceptibility profile of soft tissue infections from Northern India. Indian J Med Sci. 2004;58:10-5.
- [Google Scholar]



