
Translate this page into:
Microfilaria in pleural fluid cytology: A rare finding
Address for correspondence: Dr. Subrata Pal, Sahid Colony, Sodepur, PS- Khardah, North 24 Parganas. Kolkata, West Bengal, India. E-mail: subratapal1985@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Lymphatic filariasis is endemic in India and Southeast Asia. Detection of microfilaria is infrequently reported during cytological evaluation of various lesions or body cavity fluids. Presence of microfilaria in pleural fluid cytology is very rare finding even in endemic areas. Few cases of accidental finding of microfilaria have been reported in association with malignant pleural effusion. But pleural effusion of filarial origin is extremely rare manifestation. Here we report a classical case of microfilaria in pleural fluid cytology.
Keywords
Microfilaria
pleural effusion
Wuchereria bancrofti

Introduction
Filariasis is a very common vector-borne disease in tropical countries like India.[12] It is a major health problem in India and endemic along the sea costs and river banks.[23] Clinical manifestations of filariasis range from asymptomatic microfilariasis to acute manifestations such as fever, epididymo-orchitis, lymphangitis, lymphadenitis, or chronic symptoms such as hydrocele, lymphedema, elephantiasis, and topical pulmonary eosinophilia.[34] Microfilaria in peripheral blood examination is frequent in filarial-endemic regions both in symptomatic or asymptomatic cases. However, the presence of microfilaria in pleural fluid cytology is very rare finding even in endemic areas.[245] Few cases have been reported in association with malignant pleural effusion. However, pleural effusion of filarial origin is extremely rare manifestation.[14] In the present case, we are reporting a classical case of microfilaria in pleural fluid cytology.
Case Report
A 38-year-old male patient attended pulmonology clinic of our institution with a history of cough, right-sided chest heaviness, and breathlessness for 3 weeks. On examination, he had average built, normal surface temperature. On chest percussion, there was dullness at lower zone of the right lung and diminished breath sound was noted on auscultation. He was partially treated with oral antibiotics by local physician in earlier stage. He had no past history of tuberculosis and no history of hemoptysis.
On chest X-ray, he had right-sided pleural effusion. Routine blood examination showed eosinophil count 18%. Sputum examination was negative for acid-fast Bacilli and Mantoux test was also negative. Diagnostic pleurocentesis was performed, and aspirated fluid was straw color. Biochemical tests of pleural fluid revealed sugar level 72 mg/dl, protein - 3.1 g/dl, lactate dehydrogenase level 248 IU/L, and adenosine deaminase level 14 IU/L. Total cell count of pleural fluid was 240/cmm and differential cell count showed lymphocyte 84%, eosinophil 12%, and neutrophil 4%. Ziehl–Neelsen stain of pleural fluid smear did not reveal acid-fast Bacilli. On cytological examination of centrifuged deposit of pleural fluid revealed lymphocytes, eosinophils, few reactive mesothelial cells and microfilaria of Wuchereria bancrofti [Figures 1 and 2]. No malignant cell was found in the smear examination. Repeat peripheral blood examination failed to reveal any microfilaria. He was treated with diethylcarbamazine for 3 weeks. He responded quickly with the improvement of symptoms. Repeat chest X-ray after 3 weeks revealed reduced effusion and complete resolution at 5th week.
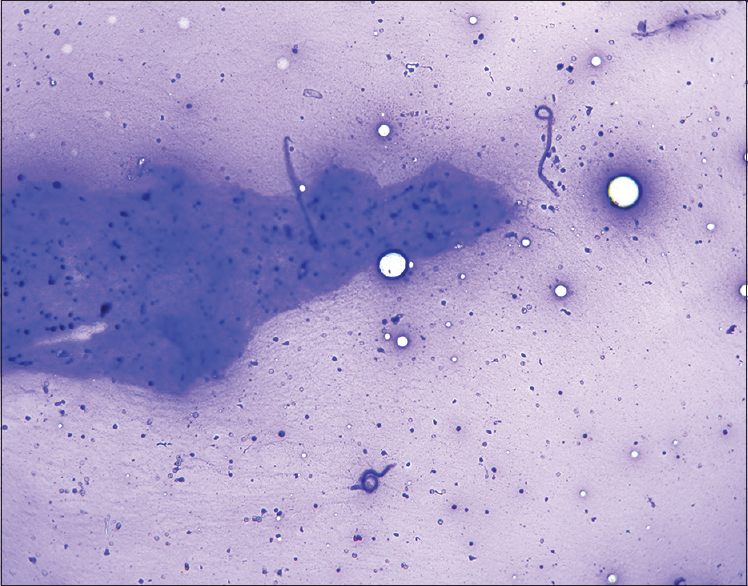
- Smear shows three microfilariae in the background of thick proteinaceous material and chronic inflammatory cells (Leishman and Giemsa stain, low power view)

- Smear shows microfilaria of Wuchereria bancrofti in pleural fluid cytology smear (Leishman and Giemsa stain, high power view)
Discussion
Filariasis is a major health problem in India.[23] It is endemic in the states along the sea costs and river banks.[36] W. bancrofti is the most common species identified.[56] Microfilaria is occasionally identified in cytology smears. Aspirates from lymph nodes, subcutaneous nodules, breast, and hydrocele fluid containing microfilaria are infrequently reported from the endemic region.[256] The presence of microfilaria in association with malignant lesions also documented in cytological evaluation.[25] However, pleural effusion as sole manifestations of filariasis is very rare.[46]
In India, most of the cases of pleural effusion are caused by tuberculosis. Exudative pleural effusion with lymphocyte predominance is supposed to be a case of tuberculous in origin. Cytological evaluation of pleural fluid is done for evaluation of differential cell count, evaluation of malignant cells, and Ziehl–Neelsen stain for acid-fast Bacilli.
Topical pulmonary eosinophilia is an occult form of lymphatic filariasis with pulmonary manifestation presents with paroxysmal cough, wheezing, shortness of breath, malaise, anorexia, and weight loss.[23] In the present case, pulmonary symptoms and peripheral blood eosinophilia both manifestations were found. Pathophysiology of topical pulmonary eosinophilia is immunological hypersensitivity to indwelling microfilarial antigen in pulmonary lymphatics.[23] Whereas filarial pleural effusion occurs due to immunological reaction against filarial antigen, lymphangitis, and incomplete lymphatic obstruction.[45] Filarial pleural effusion may be chylous or nonchylous in nature. Chylous pleural effusion occurs due to rupture of chyle from occluded thoracic duct.[6] Nonchylous effusion is supposed to be coincidental finding in the presence of microfilaria in pleural effusion. Most of the previously reported cases in literatures have shown presences of W. bancrofti species.[16] Similarly, in our case also pleural effusion was nonchylous exudative type and microfilariae of W. Bancrofti were isolated. Exudative pleural effusion in such case can be explained by lymphangitis due to incomplete obstruction of pulmonary lymphatics.
Resolution of effusion after diethylcarbamazine therapy provides strong evidence of causation of pleural effusion primarily of filarial origin. The present case report suggests a careful microscopical examination of pleural fluid before administration of specific treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Early diagnosis of filarial pleural effusion. Indian J Med Microbiol. 2003;21:207-8.
- [Google Scholar]
- Nonresolving pleural effusion in an elderly woman: A case report. Ann Thorac Med. 2010;5:247-8.
- [Google Scholar]
- Pleural effusion due to lymphatic filariasis. Indian J Chest Dis Allied Sci. 1994;36:159-61.
- [Google Scholar]
- Microfilaria in malignant pleural effusion: An unusual association. Indian J Med Microbiol. 2010;28:392-4.
- [Google Scholar]
- Microfilarial pleural effusion in a case of tropical pulmonary eosinophilia. Indian J Chest Dis Allied Sci. 2008;50:241-3.
- [Google Scholar]



