
Translate this page into:
Mixed Medullary – Papillary Carcinoma Thyroid: An Uncommon Variant of Thyroid Carcinoma
Address for correspondence: Dr. Deepti Verma, E-mail: vermadeepti09@rediffmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Mixed medullary-papillary carcinoma of the thyroid, a variant of medullary carcinoma is a rare thyroid malignancy accounting for less than 1% of the thyroid malignancies. We are presenting a case of 57-year-old lady with complaints of gradually increasing thyroid swelling for 1½ months. Fine-needle aspiration was suggestive of medullary carcinoma. Serum calcitonin levels were elevated. The patient underwent total thyoidectomy with regional cervical lymph node excision. Histopathologically, the diagnosis of mixed medullary-papillary carcinoma of the thyroid was made. It is important to know about this entity due to its prognostic implications and to prevent any diagnostic dilemmas.
Keywords
Carcinoma
mixed medullary-papillary
thyroid

INTRODUCTION
The medullary thyroid carcinomas (MTC) comprise 5-10% of all thyroid carcinomas.[1] It is known to show many cytoarchitectural variations. Mixed medullary-papillary thyroid carcinoma, a variant of MTC is a rare malignancy and known to represent <1% of all thyroid malignancies.[2] Fewer than 40 such cases have been reported so far.[3] The WHO classification of thyroid tumors[4] includes an entity called mixed medullary-follicular carcinoma and describes such tumors showing morphological features of both, medullary carcinoma with immunoreactivity for calcitonin and follicular (or papillary) carcinoma with immunoreactivity for thyroglobulin. Under this entity tumors showing mixed medullary and follicular carcinomatous components have been observed more often than medullary mixed with papillary carcinoma.
CASE REPORT
A 57-year-old lady presented to surgery outpatient department with a gradually increasing thyroid swelling since one and half months which was soft and nontender involving central and left lobe of the thyroid. Ultrasonographically, a 4 cm × 3.2 × 3 cm left solitary thyroid nodule with hypervascularity was noted. The thyroid function test was normal. The fine-needle aspiration (FNA) suggested the possibility of medullary carcinoma, thyroid. The serum calcitonin levels thus performed were elevated (450 pg/ml). Patient underwent total thyroidectomy with regional cervical lymph node excision. The specimen showed a circumscribed, solid, nodular, gray-white mass measuring 4.5 cm × 4 cm × 3.5 cm in the left lobe, also involving the isthmus [Figure 1]. The right lobe was unremarkable. Histopathologically, tumor comprised of papillary fronds [Figure 2a] with fibrovascular core; these were lined by cuboidal cells having round to oval nuclei with nuclear clearing, overlapping, and grooving. Few nuclei showed pseudoinclusions [Figure 2b]. Interspersed between these papillae were nodules separated from each other by fibrous septae. These nodules [Figure 3a] composed of dispersed cell population of round to polyhedral to plasmacytoid cells having moderate to abundant granular cytoplasm. Foci of pink amorphous amyloid-like material were also seen. The presence of dual tumor population was confirmed on immunohistochemistry. The thyroglobulin was positive while calcitonin was negative in the papillary component [Figure 2c]; thus suggestive of papillary carcinoma. The presence of calcitonin [Figure 3b], NSE, CEA and chromogranin and the absence of thyroglobulin [Figure 3c] in the nodular component suggested a simultaneous medullary carcinoma. The resected cervical lymph node showed metastatic deposits from the medullary component. Thus, a diagnosis of mixed medullary-papillary thyroid carcinoma with cervical metastasis was established.
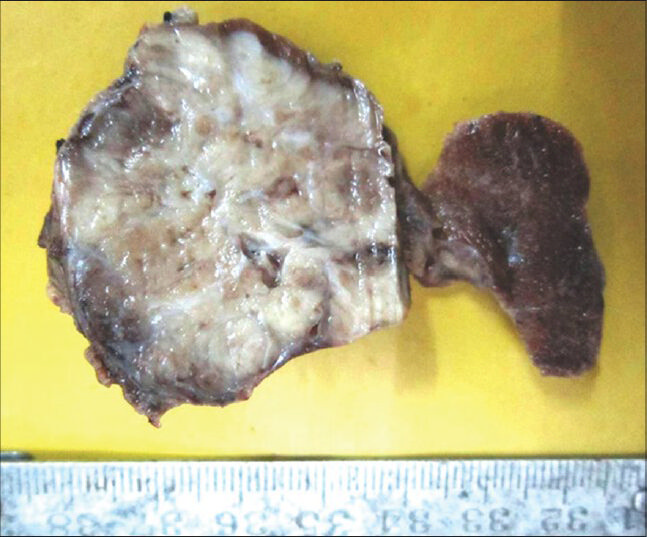
- Gross findings of the thyroidectomy specimen: A circumscribed, infiltrative, solid, gray-white mass measuring 4.5 cm × 4 cm × 3.5 cm involving the left lobe and the isthmus. The residual normal thyroid can be seen compressed at the periphery of the tumor. The right lobe was unremarkable
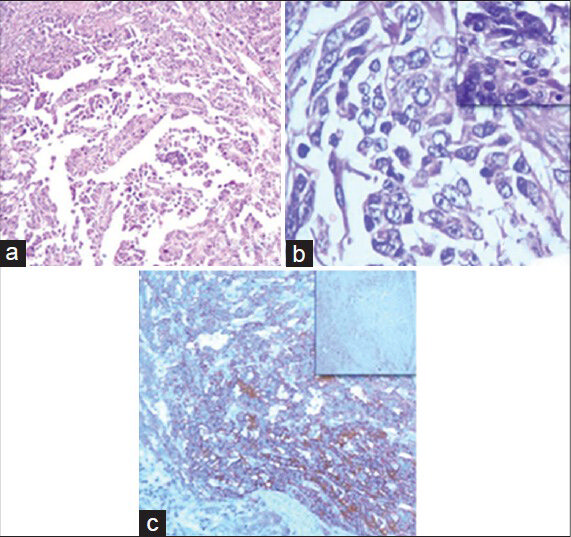
- The papillary component of the tumor: (a) The tumor comprised of papillae with fibrovascular core being lined by cuboidal cells with round to oval nuclei (H and E, ×10). (b) The nuclei showed clearing, overlapping, grooving, and the presence of pseudoinclusions (inset) in few cells (H and E, ×40). (c) The tumor showed cytoplasmic immunopositivity for thyroglobulin and immunonegativity for calcitonin (inset) (immunohistochemistry, ×10)
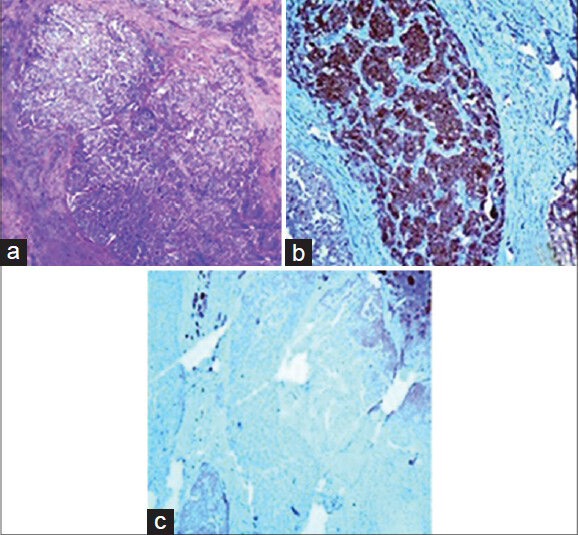
- The medullary component of the tumor: (a) The tumor was present as nodules composed up of dispersed cell population of round to polyhedral to plasmacytoid cells having moderate to abundant granular cytoplasm (H and E, ×10). (b) The tumor showed cytoplasmic immunopositivity for calcitonin (immunohistochemistry, ×10). (c) The tumor was immunonegative for thyroglobulin; thyroglobulin positivity is seen in the entrapped normal thyroid follicles acting as positive internal control (immunohistochemistry, ×10)
DISCUSSION
The thyroid carcinomas have been divided into two groups based on the proposed cell of origin: Follicular and papillary tumors arising from follicular cells and medullary neoplasms arising from parafollicular cells.[5] Tumors showing concurrent medullary and papillary features are rare.
Albores-Saavedra et al.[6] reported two cases of mixed medullary- papillary carcinoma of the thyroid showing intimately admixed distinctive population of medullary and papillary carcinomas in which medullary component predominated.
Matias-Guiu et al.[7] described a case with two components of medullary and papillary carcinomas which merged imperceptively in some and were clearly separate in few areas.
Gero et al.[5] reported a case of the collision tumor of medullary and papillary carcinoma thyroid that showed predominantly a papillary component and a separate small firm white nodule grossly that demonstrated medullary carcinoma. Similar three cases were reported by Rossi et al.[2]
Many different variants of MTC are known in the literature such as papillary, pseudopapillary, follicular, clear cell, oxyphil, small cell, squamous, and melanotic variants. Shukla et al.[8] have described the papillary variant of MTC, which can be confused morphologically with mixed medullary-papillary carcinoma. The immunohistochemical markers are important to differentiate it from mixed medullary-papillary carcinoma. The calcitonin positivity and negativity for thyroglobulin favor the papillary variant of MTC.
Our case showed two distinct tumors: MTC arranged as nests and trabeculae and comprising round to plasmacytoid cells with moderate to abundant granular cytoplasm and showing calcitonin, CEA, NSE, and chromogranin immunopositivity and immunonegativity for thyroglobulin. The second tumor was papillary thyroid carcinoma formed up of papillae lined by round to cuboidal thyroglobulin positive and calcitonin negative cells displaying nuclear clearing, overlapping, grooving, and pseudoinclusions in few cells. However, this papillary component was missed on FNA. The thyroglobulin positivity and negativity for calcitonin, CEA, NSE, and chromogranin in the papillary component ruled out the possibility of papillary variant of MTC and hence supported the diagnosis of mixed medullary-papillary thyroid carcinoma.
The cellular origin for the mixed medullary follicular carcinoma is not exactly established, yet one of the hypothesis shows that the tumor might arise from multipotent stem cells and that the ultimobranchial rests might play a role.[1] An alternative hypothesis presumes a common oncogenic stimulus affecting both follicular and parafollicular cells.
It is difficult to comment upon the prognosis of such combined thyroid carcinomas as few cases have been reported.[9] Patients with papillary carcinoma have the highest 10 year relative survival while MTC is considered to have a worse prognosis, difficult to cure and more likely to recur.[10] However, according to WHO,[4] prognosis of mixed medullary and follicular thyroid carcinoma depends upon the medullary component. Hence, presence of the medullary component makes the prognosis worse as compared to pure papillary carcinoma.
To conclude, knowledge of this rare less known variant of MTC is important to avoid diagnostic dilemma and due to its prognostic implications. Furthermore, the current case highlights the importance of immunohistochemical markers to make a correct diagnosis and rule out the other similar tumors.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Mixed medullary and follicular carcinoma of the thyroid – A rare entity. Med Case Stud. 2011;2:12-4.
- [Google Scholar]
- Medullary and papillary carcinoma of the thyroid gland occurring as a collision tumour: Report of three cases with molecular analysis and review of the literature. Endocr Relat Cancer. 2005;12:281-9.
- [Google Scholar]
- Mixed medullary-papillary carcinoma of the thyroid: A case report. Laryngoscope. 2010;120(Suppl 4):S153.
- [Google Scholar]
- Mixed medullary and follicular cell carcinoma. In: World Health Organization Classification of Tumors: Pathology and Genetics: Tumors of Endocrine Organs. Lyon: IARC Press; 2004. p. :92.
- [Google Scholar]
- Medullary and papillary carcinomas occurring as a collision tumor: Report of a case. Clin Nucl Med. 1989;14:171-4.
- [Google Scholar]
- Mixed medullary-papillary carcinoma of the thyroid: A previously unrecognized variant of thyroid carcinoma. Hum Pathol. 1990;21:1151-5.
- [Google Scholar]
- Compound medullary-papillary carcinoma of the thyroid: True mixed versus collision tumour [corrected] Histopathology. 1994;25:183-5.
- [Google Scholar]
- Papillary variant of medullary carcinoma thyroid. Indian J Pathol Microbiol. 2014;57:151-2.
- [Google Scholar]
- Coexistence of papillary and medullary carcinoma of the thyroid gland-mixed or collision tumour? Clinicopathological analysis of three cases. Virchows Arch. 1994;424:441-7.
- [Google Scholar]
- Simultaneous medullary and papillary thyroid cancer: Two case reports. J Med Case Rep. 2007;1:133.
- [Google Scholar]



