
Translate this page into:
Necrotizing Soft-Tissue Infection: Laboratory Risk Indicator for Necrotizing Soft Tissue Infections Score
Address for correspondence: Dr. Madhuri Kulkarni, E-mail: mkmysore@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Necrotizing soft tissue infections (NSTI) can be rapidly progressive and polymicrobial in etiology. Establishing the element of necrotizing infection poses a clinical challenge. A 64-year-old diabetic patient presented to our hospital with a gangrenous patch on anterior abdominal wall, which progressed to an extensive necrotizing lesion within 1 week. Successive laboratory risk indicator for necrotizing softtissue infections (LRINEC) scores confirmed the necrotizing element. Cultures yielded Enterococci, Acinetobacter species and Apophysomyces elegans and the latter being considered as an emerging agent of Zygomycosis in immunocompromised hosts. Patient was managed with antibiotics, antifungal treatment and surgical debridement despite which he succumbed to the infection. NSTI's require an early and aggressive management and LRINEC score can be applied to establish the element of necrotizing pathology. Isolation of multiple organisms becomes confusing to establish the etiological role. Apophysomyces elegans, which was isolated in our patient is being increasingly reported in cases of necrotizing infections and may be responsible for high morbidity and mortality. This scoring has been proposed as an adjunct tool to Microbiological diagnosis when NSTI's need to be diagnosed early and managed promptly to decrease mortality and morbidity, which however may not come in handy in an immunocompromised host with polymicrobial aggressive infection.
Keywords
Laboratory risk indicator for necrotizing soft tissue infections score
necrotizing infection
zygomycosis

INTRODUCTION
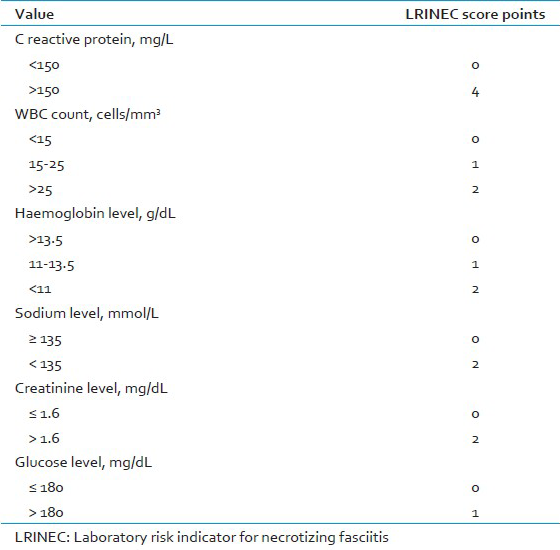
Necrotizing soft tissue infections (NSTIs) are often encountered in surgical practice, especially in immunocompromised hosts.[123] These infections progress very rapidly and need prompt debridement and specific antimicrobial therapy.[4] Attributing pathogenic roles to the isolated organisms becomes a Microbiologists dilemma while establishing the necrotizing element poses a challenge to the attending surgeon. The Laboratory Risk Indicator for Necrotizing Soft Tissue Infections (LRINEC) scoring proposed by Wong et al.[5] [Tables 1 and 2] was adapted in our patient to guide management; however being immunocompromised, the patient succumbed to the supposedly severe infection, the clinical scenario often a surgeon's nightmare.

CASE REPORT
A 64-year-old male patient was brought to the surgical OPD of JSS Medical College, Mysore, Karnataka, on the 29th of February, 2013, with the complaints of fever and a painful blackish lesion on the right lower abdomen. Patient was a diabetic, on dietary modification, under glycemic control. He was also a known case of bronchiectasis on treatment with steroids and had visited a local doctor a week back for neuritic type of pain in the right lower abdomen, for which a Diclofenac patch, had been applied by the doctor. Patient noticed pain and swelling in the area 2 days later. When the lesion started spreading and he also began to have spikes of fever, patient was brought to our hospital.
On examination, there was a patch of gangrene on the anterior abdominal wall in the iliac region measuring 5 cm × 5 cm. There was pus oozing from a small area of the wound. Patient was febrile; there were no other significant findings except bilateral basal crepitations.
In view of the immunocompromised state, the toxicity and the gangrene, possibility of a necrotizing infection was considered and biochemical and hematological workup was ordered. The LRINEC score at the time of admission was 7 as indicated [Table 3]. Pus was collected and subjected to Gram stain, acid fast stain and bacterial, mycobacterial and fungal cultures were put up. Gram stained smear revealed the presence of plenty of inflammatory cells, Gram positive cocci in chains and Gram negative coccobacilli. There were also a large number of broad aseptate fungal hyphae, suggestive of Zygomycosis. Blood culture (BacT Alert) did not yield any bacterial or fungal growth.

In view of the clinical and laboratory findings, the patient was posted for wide excision and debridement. He was started on treatment with Imipenem, Linezolid and also low dose amphotericin B.
There was soakage of the dressing on the 2nd day after surgery, there was sloughing of the skin and subcutaneous tissue and pain persisted. Repeat Gram stain showed the same findings. Aerobic bacterial culture yielded the growth of Enterococci sensitive to Linezolid and Acinetobacter sensitive to piperacillin-tazobactam, imipenem, meropenem and amikacin. The bacterial isolates were identified by using Vitek 2 automated system. Anaerobic cultures (Gaspak) did not yield any bacterial growth.
Fungal culture showed a fluffy wooly white colony with no sporulation after 3 days. On slide culture at 25°C and 40°C in biological oxygen demand incubator, sporulation was observed after 10 days. Broad aseptate hyphae with unbranched sporangiophores, prominent funnel shaped apophyses and pyriform sporangia were observed [Figure 1]. Based on thermotolerance (up to 40°C) and morphological features the fungus was presumptively identified as Apophysomyces elegans.

- Lactophenol Cotton Blue mount of slide culture showing funnel shaped sporangia and sporangiospores of Apophysomyces elegans
Histopathological examination (H and E stain) revealed broad aseptate hyphae suggestive of Zygomycosis. The hyphae were periodic acid schiff (PAS) positive. Vascular invasion was observed.
Antibiotic treatment was continued, repeat LRINEC scores were validated [Table 3] and a repeat wider debridement was done. However, the lesion continued to spread relentlessly, the edge of the lesion was black and necrotic muscle tissue was seen in the wound [Figure 2]. Meanwhile patient's respiratory distress also worsened. He was put on oxygen support initially, ventilated later for respiratory distress. Patient succumbed to his illness on the 10th day after admission.

- Extensive anterior abdominal wall necrosis, blackened edge of the lesion
DISCUSSION
NSTI are group of infections that require early and aggressive surgical debridement.[123] These infections can occur in almost any anatomical area, but they most frequently involve the perineum, abdomen and lower extremities. Surgery and trauma are common etiologies, but in some cases the etiology remains uncertain.[67] Immunocompromised patients, especially those with diabetes are more likely to develop necrotizing infections. The infection spreads rapidly through soft-tissue planes and produces severe systemic sepsis. Even with timely and skilled treatment death from NSTIs is all too frequent.[8]
Wong et al.[5] have created a score, the LRINEC score wherein, they have compared a set of laboratory variables between patients with necrotizing and non-necrotizing soft tissue infections and identified 6 independent variables associated with NSTI [Table 1]. The total score has a range 0-13 and patients were categorized according to the risk of NSTI among 3 groups [Table 2]. After validation, Wong et al. showed that for intermediate and high risk patients (score 6) the score had a positive predictive value of 92% and negative predictive value of 96%.
Our patient had a LRINEC score of 7 on admission and the score became 11 on the 5th day. Inspite of early scoring; surgical intervention and antibiotic treatment the patient could not be saved. The etiology was polymicrobial and we isolated Apophysomyces elegans, which is being increasingly reported as an emerging pathogen in cutaneous zygomycosis.[8910] Whether the Diclofenac patch was the source of infection in our patient remains debatable. The immunocompromised state of the patient could have been responsible for the rapid deterioration in spite of optimum management. Isolation of multiple organisms from the wound can create a dilemma for the Microbiologist to assign pathogenic importance; however in the background of the LRINEC score the case can be worked up to establish the element of necrotizing pathology, thereby aim to resolve the surgeon's nightmare to some extent. However, in an immunocompromised patient, in spite of prompt management guided by the LRINEC scoring the patient may not be saved in these aggressive and polymicrobial infections.
CONCLUSION
The LRINEC scoring entails to establish the necrotizing element in NSTI's for immediate medical urgency of debridement and initiation of an effective multiple antimicrobial and antifungal treatment for prompt rapid management of the immunocompromised cases of NSTI.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Necrotizing soft-tissue infection: Diagnosis and management. Clin Infect Dis. 2007;44:705-10.
- [Google Scholar]
- Necrotizing soft tissue infections. Risk factors for mortality and strategies for management. Ann Surg. 1996;224:672-83.
- [Google Scholar]
- Nosocomial zygomycotic post-surgical necrotizing fasciitis in a healthy adult caused by Apophysomyces elegans in south India. J Med Vet Mycol. 1997;35:61-3.
- [Google Scholar]
- The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32:1535-41.
- [Google Scholar]
- Primary cutaneous zygomycosis from a tertiary care centre in north-west India. Indian J Med Res. 2010;131:765-70.
- [Google Scholar]
- Zygomycotic necrotizing fasciitis caused by Apophysomyces elegans. J Clin Microbiol. 1993;31:1368-9.
- [Google Scholar]
- Apophysomyces elegans: An emerging zygomycete in India. J Clin Microbiol. 2003;41:783-8.
- [Google Scholar]



