
Translate this page into:
Pattern of bone marrow involvement in non Hodgkin's lymphoma classified according to WHO classification: Report of a developing country Pakistan
Address for correspondence: Dr. Sadia Sultan, Department of Hematology and Blood Bank, Liaquat National Hospital and Medical College, Karachi, Pakistan. E-mail: sadiasultan96@yahoo.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
BACKGROUND:
Limited information is available from developing countries in patients of non-Hodgkin's lymphoma (NHL). Hence, we reviewed the demographical profile along with bone marrow infiltration pattern in patients with NHL presented at Liaquat National Hospital and Medical College.
MATERIALS AND METHODS:
In this descriptive study, adult patients with NHL were enrolled from January 2011 to December 2015.
RESULTS:
One hundred and Eighty-four histopathologically confirmed cases of NHL were identified. There were 139 males and 45 females, with a male-to-female ratio of 3:1. The mean age was 48.5 ± 16.0 years with the median age of 50 years. B-symptoms were present in 80.4% of patients. Lymph node enlargement was present in 71.1% of the cases. One hundred and sixty-eight patients had B-cell lymphoma (91.3%) and 16 patients had T-cell lymphoma (8.6%). Overall 158 (85.8%) patients had aggressive lymphoma. The frequency of bone marrow infiltration in our NHL patients was found to be 31.5%. Pattern of infiltrate was diffuse (14.6%) predominantly followed by interstitial (6.5%) and paratrabecular (5.4%) types of infiltration. The least common was nodular infiltrate accounted in 9 (4.8%) patients.
CONCLUSIONS:
B-cell lymphoma is more frequent than T-cell lymphoma. Younger age, aggressive lymphoma, and predominance of B-symptoms are more frequently seen. Diffuse bone marrow infiltration is more common in our set up probably because of a relatively late presentation in our patients.
Keywords
Non-Hodgkin's lymphoma
Pakistan
WHO subtypes

Introduction
Non-Hodgkin lymphoma (NHL) is a broad group of lymphoma comprising divergent tumors with variable clinical behaviors. NHL tends to be a disease of older age in North America and Europe.[1] It is characterized by neoplastic transformation of lymphoid lineage with the high potential for spread to various tissues throughout the body, especially bone marrow, liver, and spleen.[23]
Bone marrow biopsy is an essential component of staging workup in NHL and those patients presenting with bone marrow infiltration and/or other tissues are in Stage IV disease have shown poor prognosis and response to therapy.[4] It has been regularly reported that patients in developing countries often present at a relatively advanced stage in comparison with patients from the Western site.[567]
Bone trephine biopsy not only permits an assessment of infiltration but also the pattern and extent of infiltrate can be determined, which carries both diagnostic and prognostic significance.[8] At times, trephine biopsy may demonstrate lymphoma even when no abnormal cells have been identified in peripheral blood and bone marrow smears. Lymphomatous infiltrations by NHL are observed in various distinct patterns.
This report describes the demographical data, clinical features, and laboratory findings in NHL patients. Second, we also determined the frequency and pattern of bone marrow infiltration by NHL at the time of diagnosis.
Materials and Methods
This descriptive study was conducted over a period of 5 years from January 2011 to December 2015 at Hematology Department of Liaquat National Hospital. All NHL cases were diagnosed by morphology on hematoxylin and eosin sections and immunohistochemical (IHC) profile according to the WHO classification of lymphoid neoplasms. IHC stains using antibodies against CD 20, CD 3, CD 10, CD 5, CD 23, BCL2, cyclin D1, and CD 79a were done in each case.[9] Additional CD markers were applied if deemed necessary. Adult patients diagnosed as NHL who were ≥15 years of age were included in this analysis.
A total of 184 participants with newly diagnosed untreated NHL were included in this study. Complete blood counts were determined by automated analyzer (Cell Dyn counter). Bone marrow aspirate and trephine specimens were taken from posterior iliac spine by the standard technique after written consent. The bone marrow slides were reviewed by two hematopathologists, and the following data were collected: clinical diagnosis, lymphoma subtype, and pattern of involvement.
Statistical analysis
Data were collected and analyzed using the Statistical Package for the Social Sciences version 22.0 (SPSS Inc, Chicago, IL, USA). The results were expressed as mean (± standard deviation) for quantitative variables and are presented as frequency and percentages for qualitative variables.
Results
Demographic characteristics
Out of 184 patients, 139 were male (75.5%) and 45 were female (24.4%) with male-to-female ratio of 3:1. Age ranged between 16 and 74 years with the mean age was 48.5 ± 16.0 years and the median age of 50 years. Majority of patients (60.8%) were under 50 years of age.
Clinical findings
B-symptoms were present in 80.4% of patients, out of which low-grade fever was most common seen in 120 (65.2%), night sweating in 59.2%, while 84 (45.6%) patients had a history of weight loss. Lymph node enlargement was present in 71.1% cases. The splenomegaly and hepatomegaly were noted in 33 (17.9%) and 22 (11.9%) patients, respectively.
Subtypes of non-Hodgkin's lymphoma
168 patients had B-cell lymphoma (91.3%) and 16 had T-cell (8.6%) lymphoma. Overall 158 (85.8%) patients had aggressive lymphoma and remaining 26 (14.1%) had indolent disease. Histopathologically, diffuse large B-cell lymphoma (DLBCL) constituted major subtype in 125 (67.9%) patients, followed by follicular lymphoma in 14 (7.6%) patients and marginal lymphoma in 3.8% patients; 3.2% patients had mantle cell lymphoma, 2.7% patients of anaplastic large cell, and 2.1% patients each for Burkitt's lymphoma and T-cell-rich lymphoma. The least encounter was small lymphocytic lymphoma in 1.6% patients as shown in Figure 1.
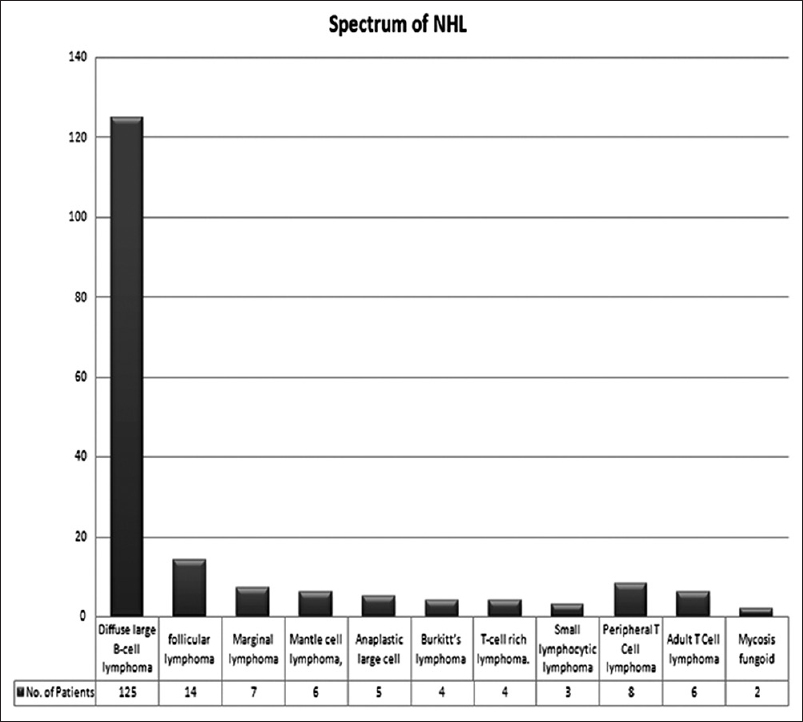
- Spectrum of NHL
In T-cell neoplasm, peripheral T-cell lymphoma and adult T-cell lymphoma are the main variants accountable in 4.3% and 3.2% patients, respectively. Merely, two patients (1.0%) were presented with mycosis fungoid.
Laboratory features
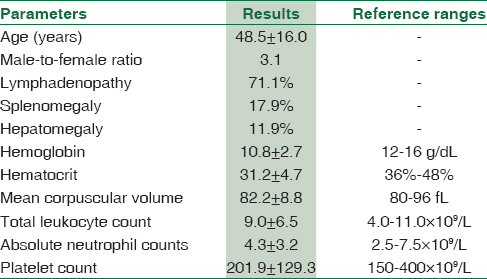
Mean hemoglobin was 10.8 ± 2.7 g/dl with the mean corpuscular volume of 82.2 ± 8.8 fl. The mean total leukocyte count was 9.0 ± 6.5 × 109/L, mean absolute neutrophil count was 4.3 ± 3.2 × 109/L, and the mean platelet count was 201.9 ± 129.3 × 109/L. Anemia (Hb <10 g/dl) was noted in 21 (11.4%) patients as shown in Table 1.
The frequency of bone marrow infiltration in our NHL patients was found to be 31.5% (n = 58). Overall, the pattern of infiltrate was diffuse in 27 (14.6%) patients, followed by interstitial in 12 (6.5%) patients and paratrabecular infiltrate in 10 (5.4%) patients. The least encountered type was nodular in 9 (4.8%) of patients as shown in Figure 2. Diffuse infiltrate is frequently seen in DLBCL patients while paratrabecular variant was seen in indolent lymphomas [Figure 3].
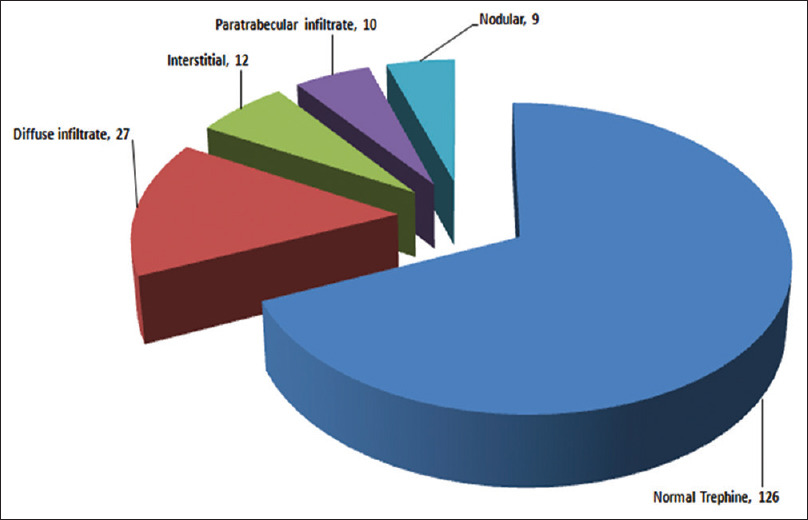
- Pattern of bone trephine infiltrate in non-Hodgkin's lymphoma
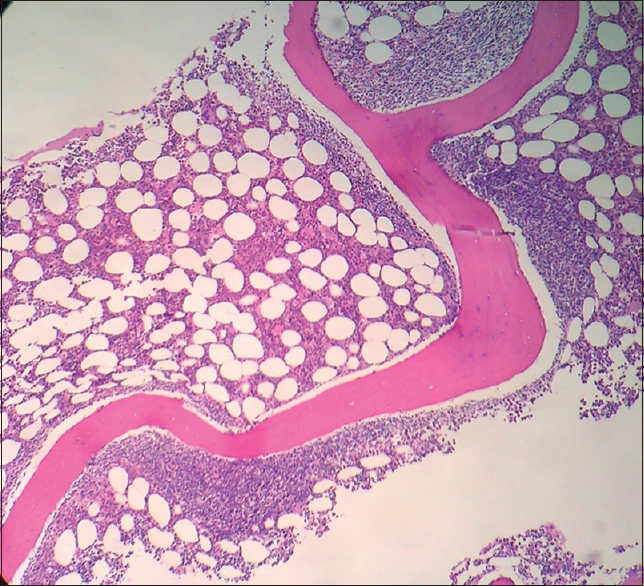
- Paratrabecular infiltrate in follicular lymphoma
Discussion
Geographically, Pakistan is located in the “lymphoma belt,” which geological boundaries are broadening from Southwestern Asia to Middle East to Northern Africa.[7] Today lymphoma is a major health problem all over the world. Its incidence is increasing largely attributed to NHL. As Hodgkin's lymphoma accounts for only ~10% of all lymphomas and the remaining 90% of cases are of NHL type globally.[10]
Regional data regarding lymphoma are limited; hence, an insight is needed to identify the disease spectrum and burden locally. The risk of NHL amplifies with the age. Mostly patients are diagnosed in their sixth or seventh decade of life. NHL is a disease of older age in Europe countries.[1] However, the median age of disease onset is ~50 years in our series. Studies from India and Southern Punjab also reveal the average age for NHL to be between 40 and 45 years, which is in concurrence to our findings.[1112] Age discordance with Western studies may be explicated by relatively longer life expectancy and more elder population in the West.
Among the NHL, B-cell NHL is much more common than T-cell variant worldwide.[13] DLBCL is the most common malignant B-cell lymphoma all over the world, and we also determined the same in our series.[214]
Staging of the NHL is foremost important for the therapeutic decisions in the management of these patients. Lymphomatous infiltration by NHL indicates advanced Stage IV disease, is usually recognized in distinct patterns, and includes interstitial pattern, in which lymphoid cells are loosely dispersed amidst hematopoietic tissue; diffuse (packed marrow) pattern, in which lymphoid cells are densely packed within the marrow spaces; lymphoid nodular pattern, in which multiple, partly confluent nodular aggregates of lymphoid cells are recognized; and paratrabecular pattern, in which the lymphoid infiltrate is adjacent to bony trabecula.
Literature searched from within the country has shown three published studies regarding marrow infiltrates by NHL. In these studies, the predominant pattern of lymphoma tissue infiltrates is diffuse variant in 46.3% and 66% cases, followed by focal aggregates and paratrabecular infiltrates.[151617] In the present study, the most common pattern of bone marrow infiltration was that of diffuse type, followed by interstitial and paratrabecular pattern of invasion.
A previous study reported from Turkey revealed relatively lower prevalence of lymphomatous infiltration (18.7%) when compared with our results.[18] In contrast to our findings, the Western studies have shown patterns of bone marrow infiltration varying from mainly focal, paratrabecular, or interstitial to diffuse intermittently.[19] We found high rate of diffuse infiltration in our series, and this perhaps reflects that most of our patients present late when disease has already been advanced to Stage IV. The comparative pattern of bone trephine infiltrate with others studies is shown in Table 2.

Conclusions
Finally, NHL occurs at a younger median age in Pakistan. B-cell lymphoma is more frequent than T-cell lymphoma with DLBCL being the most common NHL. Aggressive lymphoma and predominance of B-symptoms are more frequently seen. Diffuse bone marrow infiltration is more common in our set up probably because of a relatively late presentation in our patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors sincerely thank all patients. We are also thankful to Mr. Zain Mahmood for data analysis.
References
- Hodgkin's and Non-Hodgkin's lymphomas in an Indian Rural medical institution: Comparative clinicopathologic analysis. Asian Pac J Cancer Prev. 2010;11:1605-8.
- [Google Scholar]
- Adult non-Hodgkin's lymphoma patients: Experience from a tertiary care cancer centre in North East India. Asian Pac J Cancer Prev. 2015;16:2879-81.
- [Google Scholar]
- Signs, symptoms and complications of non-Hodgkin's lymphoma according to grade and stage in South Iran. Asian Pac J Cancer Prev. 2015;16:3551-7.
- [Google Scholar]
- Detection of bone marrow infiltration by non-Hodgkin's lymphoma – comparison of histological findings, analysis of gene rearrangements, and examination by magnetic resonance imaging. Klin Wochenschr. 1991;69:345-50.
- [Google Scholar]
- Malignant lymphomas in Pakistan according to the WHO classification of lymphoid neoplasms. Asian Pac J Cancer Prev. 2008;9:229-32.
- [Google Scholar]
- Prolonged disease-free survival in pediatric non-Hodgkin's lymphoma using ifosfamide-containing combination chemotherapy. Hematol Oncol. 1991;9:281-6.
- [Google Scholar]
- A review of histology of bone marrow trephine in malignant lymphomas. Niger J Med. 2003;12:198-201.
- [Google Scholar]
- WHO Classification of Tumors: Pathology and Genetics of Tumors of Haematopoietic and Lymphoid Tissues. Lyon: IARC Press; 2008.
- [Google Scholar]
- Malignant lymphomas in Jos, Nigeria: A ten-year study. Cent Afr J Med. 1992;38:17-25.
- [Google Scholar]
- Non-Hodgkin's lymphoma in South Punjab. Retrospective analysis of 148 patients. Pak J Med Res. 1989;28:223-31.
- [Google Scholar]
- WHO classification of malignant lymphomas in Korea: Report of the third Nationwide study. Korean J Pathol. 2011;45:254-60.
- [Google Scholar]
- Clinical characteristics, pathological distribution, and prognostic factors in non-Hodgkin lymphoma of Waldeyer's ring: Nationwide Korean study. Korean J Intern Med. 2014;29:352-60.
- [Google Scholar]
- Bone marrow involvement in non-Hodgkin's lymphoma. A study of 41 untreated cases. Pak Armed Forces Med J. 1992;42:90-2.
- [Google Scholar]
- The pattern of bone marrow infiltration in non-Hodgkin's lymphomas. J Pak Med Assoc. 1995;45:173-6.
- [Google Scholar]
- Pattern of bone marrow infiltration in non-Hodgkin's lymphomas. J Rawal Med Coll 2008:12:66-71.
- [Google Scholar]
- Non-Hodgkin's lymphoma in southeast Turkey: Clinicopathologic features of 490 cases. Ann Hematol. 2004;83:265-9.
- [Google Scholar]
- Bone marrow biopsy involvement by non-Hodgkin's lymphoma: Frequency of lymphoma types, patterns, blood involvement, and discordance with other sites in 450 specimens. Am J Surg Pathol. 2005;29:1549-57.
- [Google Scholar]



