
Translate this page into:
Respiratory Epithelium Adenomatous Hamartoma: An Incidental Finding or Precancerous Lesion?
Address for correspondence: Dr. Manoj Madakshira Gopal, E-mail: manoj.gopal@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Hamartoma is a mass of disorganized but mature specialized cells or tissue indigenous to that particular site. Uncommon examples of hamartomas have been noted in the upper aerodigestive tract too.[1] Respiratory epithelial adenomatoid hamartoma (REAH) was first described by Wenig and Heffner.[2]
We encountered a male patient with a squamous cell carcinoma of the maxillary sinus with adjoining mucosa showing histological evidence of REAH. REAH is characterized by glandular proliferation originating from the surface of respiratory epithelium. Thus, REAH can be mistaken for inverted papilloma, nasal polyp, antrochoanal polyp, and even with low-grade adenocarcinoma. Consequently, the differential diagnosis is crucial in this entity. Misinterpretation of the REAH as chronic sinus inflammation may result in inadequate treatment.
The patient underwent left medial maxillectomy with ipsilateral neck dissection. Histological examination of tumor with adjacent mucosa revealed a squamous cell carcinoma with a contiguous lesion composed of well-formed, branching glands of various sizes covered with pseudo-stratified ciliated respiratory epithelial cells separated by stromal tissue. The surface of the lesion was lined with ciliated respiratory epithelium in direct continuity with some of the glands [Figure 1]. Immunohistochemistry showed positivity for pan cytokeratin (CK) and CK7 in the hamartomatous cells, while the basal cells showed nuclear staining with p63. The other markers – CK20, calponin, smooth muscle actin, and S100 were negative [Figure 1].
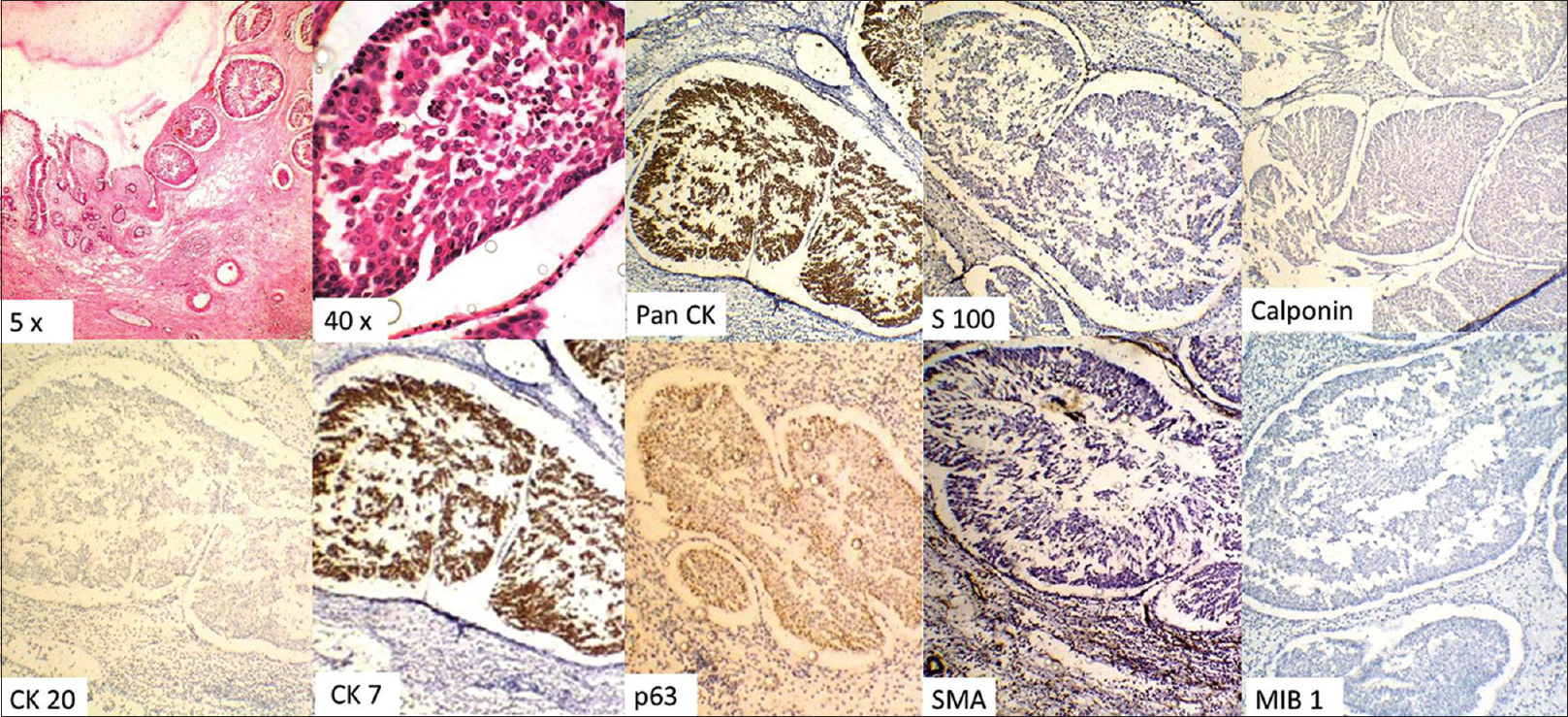
- Composite photomicrograph showing hematoxylin and eosin stained section of the hamartomas glandular proliferation into the stroma, with the epithelial cells being positive for Pan cytokeratin and cytokeratin 7 and negative for S100, calponin, cytokeratin 20, and smooth muscle actin. The basal is seen to be positive for p63. The MIB-1 proliferative index is low
REAH affects men in the third to ninth decades.[1234] Presenting complaints vary from nasal obstruction to chronic recurrent sinusitis.[3] The most common site of occurrence is posterior septum.[1234] Radiologically, there is opacification of affected sinus with a connection to nasal septum.[3] The lesion also tends to grow slowly, as evidenced by bony expansion rather than erosion.[3]
REAH presents as polyps which tend to be fleshy to firm, yellow to white masses of varying sizes.[3] The histologic picture is dominated by presence of a submucosal glandular proliferation.[3] The glands are lined by ciliated respiratory epithelium originating from the surface respiratory epithelium.[1234]
Complex glandular growth and cribriform architecture are absent.[3] The nuclear features of REAH are bland. Long-term chronic inflammation and polyp formation within the respiratory epithelium are thought to be the etiologic precursors to REAH.[1234] The use of Mindbomb 1 (MIB-1) is useful in distinguishing REAH from other neoplasms, since neoplasms tend to have a high proliferation index.[3] Studies on immunohistological profile of REAH have shown the epithelial cells to be Pan CK and CK7 positive, but CK20 negative with p63 staining the basal cells.
The differential diagnoses of REAH in paranasal sinus include inverted papilloma and adenocarcinoma.[1234] The inverted papilloma derives from the Schneiderian membrane and is composed of papillary fronds with a delicate fibro vascular core covered by multiple layers of epithelial cells, the most often of squamous or transitional cells, in contrast to the REAH, which shows adenomatoid structures lined by a single layer of ciliated columnar epithelium. Sinonasal low grade adenocarcinoma may produce an architectural pattern mimicking that of REAH. It can be distinguished from REAH by the presence of numerous uniform small glands or acini arranged in a back-to-back pattern, cellular pleomorphism, atypical mitoses, keratin pearls, loss of basement membranes, and stromal invasion associated with an inflammatory-desmoplastic response.[3]
Head and Neck surgeons should be aware of this pathological entity and its potential to be mistaken clinically for inverted papilloma and/or adenocarcinoma. The definitive treatment for REAH is simple surgical excision whereas the other diagnoses require more complex surgical excision.[134] On the other hand, misinterpretation of REAH as a chronic sinus inflammation may result in inadequate treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Respiratory epithelial adenomatoid hamartoma: Diagnostic pitfalls with emphasis on differential diagnosis. Adv Anat Pathol. 2007;14:11-6.
- [Google Scholar]
- Respiratory epithelial adenomatoid hamartomas of the sinonasal tract and nasopharynx: A clinicopathologic study of 31 cases. Ann Otol Rhinol Laryngol. 1995;104:639-45.
- [Google Scholar]
- The importance of the differential diagnosis in rhinology: Respiratory epithelial adenomatoid hamartoma of the sinonasal tract. Acta Otorrinolaringol Esp. 2012;63:55-61.
- [Google Scholar]
- Basal/myoepithelial cells in chronic sinusitis, respiratory epithelial adenomatoid hamartoma, inverted papilloma, and intestinal-type and nonintestinal-type sinonasal adenocarcinoma: An immunohistochemical study. Arch Pathol Lab Med. 2007;131:530-7.
- [Google Scholar]



