
Translate this page into:
Seropositivity Pattern of Human Cystic Echinococcosis at a Tertiary Care Hospital of India

Address for correspondence: Bijay Ranjan Mirdha, MD, FAMS, Department of Microbiology, All India Institute of Medical Sciences, Room No. 2077, Teaching Block, New Delhi, 110029, India (e-mail: mirdhabr@hotmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cystic echinococcosis (CE), even after several control measures, causes significant morbidity throughout the world. Besides imaging investigation technology, the serological tests are essential for both diagnosis and management of this slowly progressive disease. The present study was a hospital-based retrospective study that examined the seropositivity rate for Echinococcus granulosus sensu lato antibody in patients suspected of CE at our tertiary health care center over 8 years from 2013 to 2020. Records of new visits to hospital/clinics and associated hospital discharge constituted the denominator of calculation. All samples were tested using commercially available indirect immunoglobulin G enzyme-linked immunosorbent assay kit. A total of 925 suspected patients with a clinical diagnosis of CE were screened. The age group that commonly tested positive for CE was 20 to 39 years, and liver was the predominant organ found to be affected. The seropositive rate was 41.2%. On further year-wise analysis, it was observed that the seropositivity rate had significantly declined from 61.4% in 2013 to 33.8% in 2020. This study clearly showed that there is a by 27.6% decline of CE seropositivity rate in 8 years. This declining rate may be attributed to improved socioeconomic status and better implementation of health programs.
Keywords
echinococcus granulosus
ELISA
seropositivity rate
hospital
cystic echinococcosis

Introduction
Echinococcosis, also called hydatid disease or hydatidosis, is a cyclozoonotic disease of global public health and veterinary importance. The disease occurs as a result of infection by the larval (metacestode) stages of taeniid cestodes of the genus Echinococcus. It is characterized by long-term growth of metacestode (larval) stages to hydatid cysts, in internal organs (mainly the liver and lungs) of intermediate host animals, commonly in sheep and goats. Humans do not play a role in the natural cycle but can be an accidental dead-end host. Among various species, Echinococcus granulosus sensu lato causes cystic echinococcosis (CE). Human CE is the most common presentation and nearly accounts for more than 95% of the estimated 2 to 3 million cases worldwide.[1,2] Despite significant progress in the control of echinococcosis as cited by Craig et al, the highest prevalence of this disease has been reported from temperate countries,[3] predominantly from South America, North Africa, Australia, and certain parts of Asia.[4,5] However, the actual prevalence is still considered to be underestimated.
The CE is endemic in India; the foci of the disease exist with highest prevalence in Andhra Pradesh, Tamil Nadu, and Kashmir.[6,7] In India, the annual incidence of human CE varies from 1 to 200 per 10,0000 persons. It has been reported that human CE cases do affect different body organs and parts of the body both primarily and secondarily during the course of the disease process with immense morbidity.[8] It has been documented that most primary infections in humans result in producing a single hydatid cyst; however, 20 to 40% cases are reported to have multiple cysts or multiple organ involvement.[8] The reasons for the site preference in the intermediate host for the final establishment of infection are poorly understood. The preference to a particular site may either be attributed to anatomical or physiological characteristics of the host or it may plausibly be due to different strains of taeniid that may have preferential predilections to a particular organ based on homologous ligand and receptors. Liver and lungs act as the first and second filter organs, respectively, for this parasite, and therefore, these organs are primarily exposed to the infection albeit other organs and body sites. The human hydatid cysts due to Echinococcus granulosus sensu lato infection have often been classified as fertile, sterile, and calcified.[9] The major sources of morbidity are due to pressure effects from both size and location of the cyst(s) and/or rupture of the cyst(s) leading to anaphylaxis or dissemination of the infection.
The useful diagnostic methods for human CE include ultrasonography specially for hepatic and extrahepatic cysts with a sensitivity of 93 to 98% and computed tomography (CT) that helps in detection of the presence of daughter cysts and calcification in the cyst wall with a sensitivity of detection of 90 to 97%.[10] Sometime, magnetic resonance imaging (MRI) is preferred for detail and adequate demonstration of features of the hydatid cyst. The imaging with CT as well as MRI is central to the diagnosis of cerebral hydatid cysts. However, the role of different serological tests applied for the diagnosis of human CE diagnosis can be undermined. Serological assays for the detection of serum antibodies are usually helpful when imaging findings are inconclusive, especially during early stage and are often complementary.[11] Serological screening tests to detect asymptomatic hydatid cases have clearly shown that the prevalence rate is much higher than the corresponding surgical incidence often clinically diagnosed at clinics. The symptomatic cases examined in the hospital may therefore represent only a very small proportion of the total existing infections. The current methods used for serodiagnosis of CE is based on the detection of immunoglobulin G (IgG) antibodies to cyst fluid-derived native or recombinant antigen B (AgB) subunits, either by using enzyme-linked immunosorbent assay (ELISA) or in immunoblot technique. A novel 32 kDa EpC1 antigen, which is located in the germinal layer of the hydatid cyst and the early protoscolex of Echinococcus granulosus sensu lato, demonstrated antibodies in 92.2% of preoperative human cases of CE compared with 84.5% cases detected using native AgB.[3] Rahimi et al assessed the performance of AgB isolated from different E. granulosus intermediate hosts and from different cyst locations for the immune diagnosis of human CE and reported that these are increased with diagnostic sensitivity and specificity of the assay.[12] At present, no circulating antigen detection test is commercially available. The serodiagnosis for echinococcosis is not only important to give a supportive evidence but also for knowing the seroprevalence of the disease in clinically suspected, vulnerable population as well as in the community. So, it is often desirable and necessary to periodically estimate the serostatus of a given population for the diagnosis and appropriate treatment and management of slowly progressive cystic lesions in patients with CE. In this study, we have analyzed the seropositivity rate for Echinococcus granulosus sensu lato antibody in patients suspected of hydatid disease at our tertiary health care centers.
Materials and Methods
The present retrospective hospital-based study analyzes seropositive sera for the diagnosis of CE during the period January 2013 to December 2020 in suspected patients. All clinical serum samples from these patients were submitted to the laboratory from the emergency department, various outpatient clinics, as well as from inpatient departments at the discretion of consulting physicians pertaining to clinical diagnosis. The tests were performed using commercially available IgG detecting indirect ELISA kit (NovaTec, Immundiagnostica, GmbH, Germany) as per manufacturer's instruction, and the results were interpretated accordingly. The above-mentioned commercial kit was used for most of the years and at times when there were difficulties in procuring the ELISA kits based on the same principle with more or less same sensitivity and specificity were used. The sensitivity and specificity of all the commercial kits used ranged between 96 to 97% and 98 to 99%, respectively. The representative sera with confirmed diagnosis of ascariasis, strongyloidiasis, amoebiasis, and toxoplasmosis were tested earlier using these kits to check cross-reactivity, if any, and there was none. The database for all the patients tested positive for CE during the study period was retrieved from the laboratory records and further analyzed.
Results
During this period of study, a total of 925 sera were received from suspected patients with a clinical diagnosis of cystic hydatidosis. All these samples were tested by ELISA for the presence of anti-E. granulosus IgG antibodies. Out of 925 serum samples, 381 samples (41.2%, 381/925) were positive (►Table 1). The seropositivity rate for these 8 years found to be 41.2%; however, it showed decline trend upon year-wise stratification from 61% in 2013 to 30 to 38% in later years (►Fig. 1).
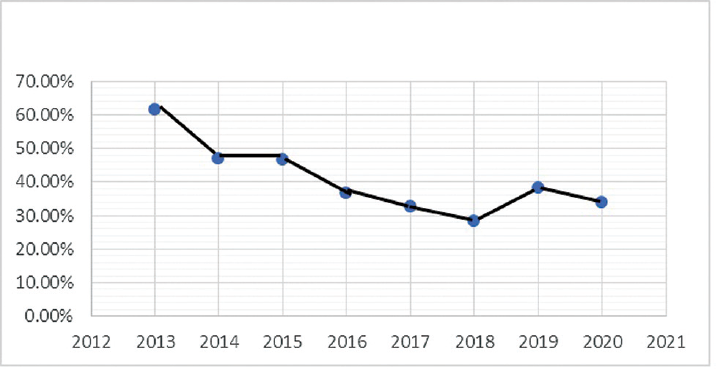
- Year-wise stratification of seropositivity rate.
| Year | No. of total sera (n = 925) | No. of negative sera (n = 554) | No. of positive sera (n = 381) | Seropositivity (overall 41.2%) |
|---|---|---|---|---|
| 2013 | 135 | 52 | 83 | 61.48% |
| 2014 | 113 | 60 | 53 | 46.90% |
| 2015 | 116 | 62 | 54 | 46.55% |
| 2016 | 117 | 74 | 43 | 36.75% |
| 2017 | 122 | 82 | 40 | 32.78% |
| 2018 | 123 | 88 | 35 | 28.45% |
| 2019 | 128 | 79 | 49 | 38.28% |
| 2020 | 71 | 47 | 24 | 33.80% |
On analysis of age-wise distribution among 381 seropositive cases, seropositivity was most common in the age group of 20 to 39 years (34%, 133/381) followed by 0 to 19 years (25.7%, 98/381) and 40 to 59 years (13.6%, 52/381) (►Fig. 2).
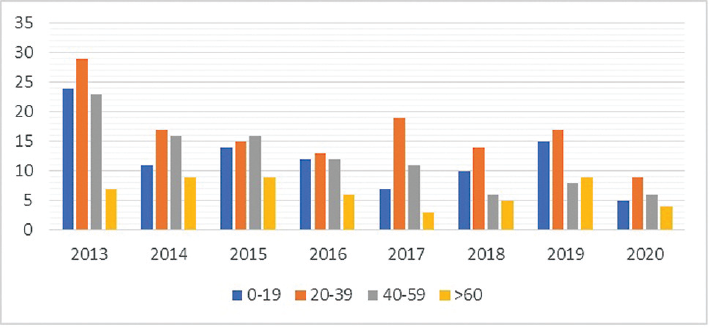
- Age-wise distributions of seropositivity.
All the seropositive cases were further analyzed according to the involvement of the site of the cyst(s) in the infected patient. The most common sites of cyst were reported in liver in 311 cases (81.6%, 311/381) followed by lungs in 45 cases (11.8%, 45/381) (►Table 2).
| Site | No of cases (n = 381) |
|---|---|
| Liver | 311 |
| Lungs | 45 |
| Kidney | 1 |
| Spleen | 1 |
| Ovaries | 1 |
| Parotid | 1 |
| Retroperitoneal space | 1 |
| Both liver and lung | 3 |
| Not known | 17 |
Discussion
As per the World Health Organization (WHO) Informal Working Group on Echinococcosis expert committee, a probable patient with CE is defined as the combination of clinical history, epidemiological history, imaging findings, and serological tests positive on two different occasions by any of the two different techniques. The serology of CE is not only an aid in the diagnosis but also provides an idea about epidemiology of the local geographical area. In the present study, seropositivity data for the past 8 years (2013–2020) showed a downward trend in seropositivity ranging from 61% in 2013 to around 30 to 38% in later years of the study. This decreasing trend is not only unique to this part of subcontinent but also a similar study conducted by Zaman et al shows seropositivity around 28.6%.[13] The study by Pednekar et al had reported that the prevalence of CE in urban centers in India has been showing a consistently decreasing trend over the past few decades, possibly due to economic development and improved government legislation of abattoirs.[14] According to the WHO, in excess of 1 million people are living with this disease at any one time. The 2015 WHO Foodborne Disease Burden Epidemiology Reference Group estimated echinococcosis to be the cause of 19,300 deaths and around 871,000 disability-adjusted life-years globally each year. As suggested by this study, the burden of CE still remains high.[1]
The most common age group affected was 20 to 39 years and male-to-female ratio was found to be 2.5:1. Infection of CE among younger age group has also been reported by Fomda et al. In their study, seropositivity was significantly higher (5.79%) in the younger age group (< 15 years) compared with the 16 to 55 years (4.07%) and over 55 years (3.05%) age groups.[15] Similarly, Andrabi et al found age group of 1 to 17 years had significantly higher number of seropositive subjects.[16] This suggests CE in humans is commonly reported in young adults and can be plausibly and more arguably related to the exposure to infecting agent during childhood, prevailing social life and human activities, and degree of man–dog contact in a community. The age relationship with the incidence and/or prevalence may also be attributed to the fact that the average age over which most people present with overt clinical manifestations for treatment (medical or surgical) and necessary management is 20 to 50 years. This is a reflection that can be attributed to the growth rate of the cyst. It was reported that cysts of E. granulosus increase in diameter between 1 and 5 cm per year. The presence of cysts are often not detected in the early stages of the disease, due to nonavailability of a reliable diagnostic tools and at times due to asymptomatic condition of the disease.
In the present study, as expected the most common site of the cyst(s) was detected in liver 81.6% (311/381). This findings are in concordance with the findings of many other studies both within the country and worldwide. It had also been observed that young adults are most commonly diagnosed with liver CE followed by alveolar echinococcosis and polycystic echinococcosis.[15]
In this study, it has been observed that there is a decline in seropositivity for CE from 61.4% in 2013 to 33.8% in 2020 in this particular region. A decline of 27.6% over a period of 8 years can be attributed to multiple factors such as improved socioeconomic status, better implementation of national programs, and improved veterinary care. As part of a One Health approach, periodic deworming of dogs with praziquantel (at least four times per year), improved hygiene in the slaughtering of livestock (including the proper destruction of infected offal), and public education campaigns in low-income countries have played pivotal role in preventing transmission as well as in alleviating the burden of this human disease. Furthermore, recently, there are many reports across the country[14,17] which have found similar decline of hydaditosis in veterinary population across the country as well as in the northern region of the country.
Limitations
In a clinical setting, the correct interpretation of serological results is often challenging as the stages of the cyst(s) (radiologically classified as active, transitional, and inactive cysts and/or fertile, sterile, and calcified) are likely to influence the outcome of serological tests.[18,19] Unfortunately, cyst stages are infrequently reported and taken into account when results of serology are evaluated in clinical practice.[20] The study essentially conducted on serological tests and other clinical samples such as aspirates and tissue biopsies could not be included as such these samples were often not provided. This could be one of the limitation of the study. Nonetheless, this study finds decline of seropositivity rate over the period of 8 years.
Conclusion
The serological test for CE even though supplementary in the diagnosis of hydatid disease but seropositivity data is absolutely essential for every geographical reason as this is an important aid in the diagnostic algorithm as well as in the approach of management. The study concludes that there is decline of seropositivity of CE over the period which can be attributed to various factors such as improved socioeconomic status and better implementation of national programs.
Authors' Contribution
R.D. contributed to writing the manuscript, and analysis and interpretation of the data; V.G. and S.K. in collection and analysis of the data; N.V. in review and edit of the manuscript; and B.R.M. in concept designing and final editing the manuscript.
Acknowledgments
The authors are thankful to all the clinical colleagues for providing necessary clinical specimens. We are grateful to parasitology laboratory technicians Mr. Vinod K. Sharma and Mr. Ashok Saini for coordinating and processing the samples. Finally, a special thanks to Mr. Varinder Kalra for secretarial assistance.
Conflict of Interest
None declared.
References
- Detection, screening and community epidemiology of taeniid cestode zoonoses: cystic echinococcosis, alveolar echinococcosis and neurocysticercosis. Adv Parasitol. 1996;38:169-250.
- [CrossRef] [PubMed] [Google Scholar]
- Global socioeconomic impact of cystic echinococcosis. Emerg Infect Dis. 2006;12(02):296-303.
- [CrossRef] [PubMed] [Google Scholar]
- Prevention and control of cystic echinococcosis. Lancet Infect Dis. 2007;7(06):385-394.
- [CrossRef] [PubMed] [Google Scholar]
- Echinococcosis: historical landmarks and progress in research and control. Ann Trop Med Parasitol. 2006;100(08):703-714.
- [CrossRef] [PubMed] [Google Scholar]
- Echinococcosis cut to cure but what about control? J Assoc Physicians India. 2012;60:9-10.
- [Google Scholar]
- Morbidity pattern of hydatid disease (cystic echinococcosis) and lack of its knowledge in patients attending Mamata General Hospital, Khammam, Andhra Pradesh. Indian J Pathol Microbiol. 2008;51(01):143-145.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological studies on echinococcosis and characterization of human and livestock hydatid cysts in Mauritania. Iran J Parasitol. 2011;6(01):49-57.
- [Google Scholar]
- Intra-abdominal extrahepatic echinococcosis. Surg Today. 2001;31(10):881-884.
- [CrossRef] [PubMed] [Google Scholar]
- Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114(01):1-16.
- [CrossRef] [PubMed] [Google Scholar]
- Performance of antigen B isolated from different hosts and cyst locations in diagnosis of cystic echinococcosis. Iran J Parasitol. 2011;6(01):12-19.
- [Google Scholar]
- Seroprevalence of human cystic echinococcosis from North India (2004-2015) Trop Parasitol. 2017;7(02):103-106.
- [Google Scholar]
- Molecular and morphological characterisation of Echinococcus from food producing animals in India. Vet Parasitol. 2009;165(1-2):58-65.
- [CrossRef] [PubMed] [Google Scholar]
- Sero-epidemiological survey of human cystic echinococcosis in Kashmir, North India. PLoS One. 2015;10(04):e0124813.
- [CrossRef] [PubMed] [Google Scholar]
- Seroprevalence of human cystic echinococcosis in South Kashmir, India. Parasite Epidemiol Control. 2020;11:e00172.
- [CrossRef] [PubMed] [Google Scholar]
- Molecular epidemiology of echinococcosis from food producing animals in north India. Vet Parasitol. 2012;186(3-4):503-506.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic performances of xommercial ELISA, indirect hemagglutination, and western blot in differentiation of hepatic echinococcal and non-echinococcal lesions: a retrospective analysis of data from a single referral centre. Am J Trop Med Hyg. 2019;101(06):1345-1349.
- [CrossRef] [PubMed] [Google Scholar]
- Factors influencing the serological response in hepatic Echinococcus granulosus infection. Am J Trop Med Hyg. 2016;94(01):166-171.
- [CrossRef] [PubMed] [Google Scholar]
- Serology for the diagnosis of human hepatic cystic echinococcosis and its relation with cyst staging: a systematic review of the literature with meta-analysis. PLoS Negl Trop Dis. 2021;15(04):e0009370.
- [CrossRef] [PubMed] [Google Scholar]



