
Translate this page into:
The Changing Pattern of the Quantum of Biomedical Waste Generated from a Tertiary Care Hospital in Delhi
Address for correspondence: Arvind Achra, MD, Department of Microbiology, Address: Atal Bihari Vajpayee Institute of Medical Sciences, Dr. Ram Manohar Lohia Hospital, Baba Kharak Singh Marg, Near Gurudwara Bangla Sahib, Connaught Place New Delhi, 110001, India (e-mail: arvindachra@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background
As a consequence of growth and advancement in health care, production of health care waste has seen an exponential upward trend. Waste from individual health care facilities can vary based on the nature and scope of health care services they provide.
Objectives
To analyze the amount of biomedical waste generated by a tertiary care hospital.
Methods
Biomedical waste generated by the hospital from 2005 to 2019 was quantified and analyzed to calculate the total amount of incinerable waste, recyclable plastic waste, and sharp and glass waste. The amount of waste generated per bed per day and the compound annual growth rate (CAGR) were also calculated.
Results
The total amount of biomedical waste generated in 2005 was 65,658 kg, which has substantially increased to 374,712 kg in 2019, with a CAGR of 12.5%. The hospital was producing average biomedical waste of 0.179 kg/bed/day in 2005, which has increased four times in 2019 to reach 0.709 kg/bed/day. The overall estimated plastic waste was 31% of the total biomedical waste in 2005 and 53% in 2019.
Conclusion
The generation of biomedical waste is likely to see significant upward trends unless diligent deliberations are held between different stakeholders in regard to the reintroduction of reusable materials and waste reduction strategies.
Keywords
biomedical waste
CAGR
CBWTF
infectious waste
plastic waste

Introduction
Over the years, there has been immense growth and advancement in health care facilities. As a consequence of this betterment and expansion, production of health care waste has seen an exponential upward trend. Waste generated by a health care facility can be infectious or noninfectious. The infectious waste is hazardous and poses serious threat to patients, health care workers, public health, and the environment. As per the World Health Organization (WHO), approximately 75 to 90% of the total health care waste generated by the health facilities is nonhazardous. The remaining 10 to 25% waste is dangerous, infectious, toxic, or with radioactive components.[1]
Waste generation from individual health care facilities can vary based on the type or level of health care facility and location of health care facilities, rural or urban. It may reflect upon the differences in the services provided, scale, organizational complexity, availability of resources, and the number of medical and other staff. Quantification of waste generation can be used to establish baseline data on the rates of production in different medical areas. It also helps in planning, budgeting, calculating revenues from recycling, optimizing waste-management systems, and assessing environmental impact. We have attempted to analyze the amount of biomedical waste (BMW) generated by a tertiary care hospital in New Delhi.
Materials and Methods
This is a retrospective study conducted in a tertiary care hospital in New Delhi from 2005 to 2019. The BMW generated and collected from various parts of the hospital was quantified and analyzed further. The waste generated before the Biomedical Waste Management Rules 2016 was segregated according to the provisions of Biomedical Waste Management and Handling Rules 1998. After the notification of the new rules in 2016, the hospital started complying with the requirements of the revised rules.
For the ease of description, waste is classified under three categories: incinerable waste, recyclable plastic waste, and sharp and glass waste. Quantification is done in terms of the total amount of waste generated annually, the amount of waste generated per bed per day, and compound annual growth rate (CAGR) for total BMW and for all three types of waste categories.
Results
The total amount of BMW generated in 2005 was 65,658 kg, which substantially increased to 374,712 kg in 2019, with a CAGR of 12.5% (►Table 1). CAGR was calculated to be 8.4, 16.4, and 15.4% for incinerable waste, plastic waste, and sharp and glass waste, respectively. The overall estimated plastic waste was 31% of the total BMW in 2005 and increased to 53% in 2019. The total number of beds in the hospital increased from 1,000 in 2005 to 1,447 in 2019. Waste generated per bed per day in different categories is depicted in ►Fig. 1, and overall it was 0.179 kg in 2005, which has increased fourfold to reach 0.709 kg in 2019. CAGR for per bed per day waste has been calculated to be 5.7% for incinerable waste, 13.6% for plastic, 12.6% for sharp and glass waste, and 9.8% for total waste.
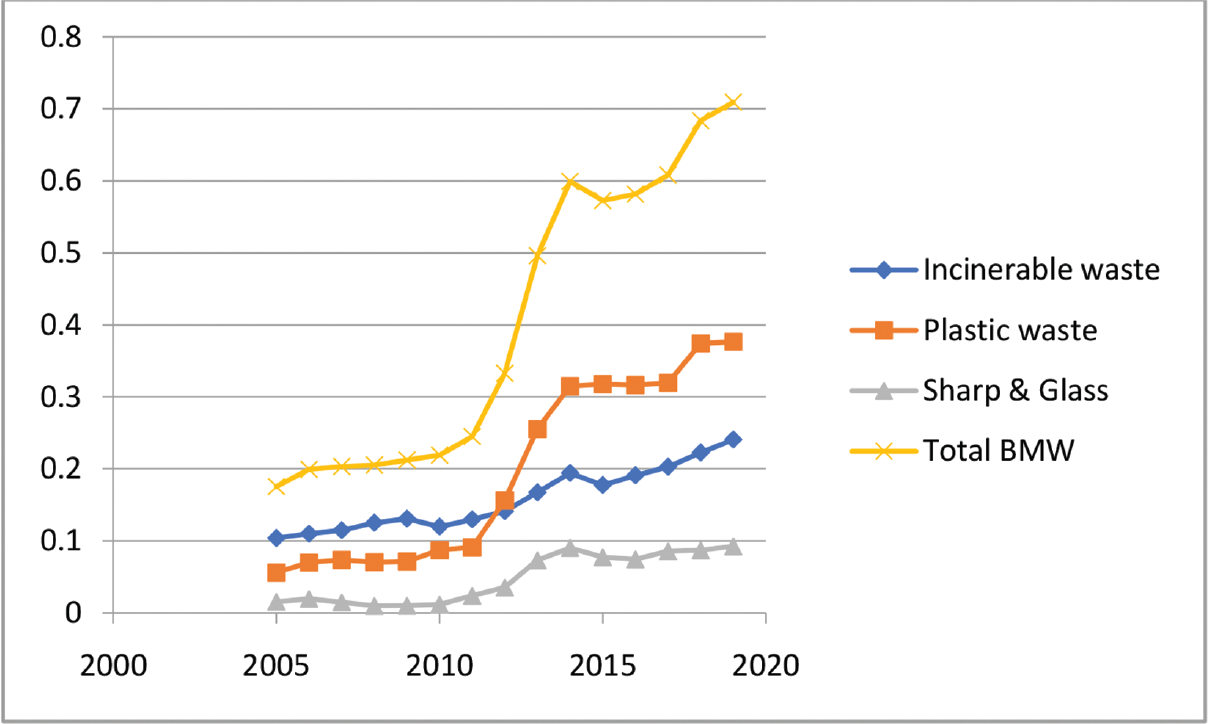
- Line diagram of different categories of BMW generated per bed per day (in kilograms). BMW, biomedical waste.
| Year | Incinerable waste (kg) | Plastic waste (kg) | Sharps and glass waste (kg) | Total BMW (kg) |
|---|---|---|---|---|
| 2005 | 37,937 | 20,400 | 5,683 | 65,658 |
| 2006 | 40,136 | 25,460 | 7,146 | 73,785 |
| 2007 | 41,909 | 26,874 | 5,434 | 75,242 |
| 2008 | 45,689 | 25,633 | 3,619 | 76,085 |
| 2009 | 50,380 | 27,452 | 3,911 | 83,365 |
| 2010 | 46,145 | 33,620 | 4,582 | 85,940 |
| 2011 | 49,976 | 35,033 | 9,299 | 95,571 |
| 2012 | 54,907 | 60,680 | 13,768 | 131,154 |
| 2013 | 65,058 | 99,320 | 28,493 | 192,871 |
| 2014 | 75,514 | 122,345 | 35,127 | 232,986 |
| 2015 | 78,802 | 140,992 | 34,395 | 254,248 |
| 2016 | 98,962 | 163,959 | 38,616 | 301,597 |
| 2017 | 107,166 | 168,799 | 45,283 | 321,248 |
| 2018 | 117,547 | 197,653 | 45,995 | 361,195 |
| 2019 | 127,113 | 198,766 | 48,833 | 374,712 |
Abbreviation: BMW, biomedical waste.
Discussion
According to a joint study conducted by ASSOCHAM (Associated Chambers of Commerce and Industry of India) - Velocity, various health sectors in India were generating approximately 550 tonnes of BMW per day in 2018. It is expected to be 780 tonnes per day by 2022, with an estimated CAGR of 9.13%.[2] The total BMW generated in our hospital from 2005 to 2019 has recorded an increase of 470.7%, with a CAGR of 12.5%. As per the WHO estimates, average hazardous waste production by a country varies from 0.2 to 0.5 kg/bed/day based on their per capita income.[3] A study from a tertiary care hospital in India reported an average of 0.341 kg/bed/per day of infectious waste.[4] Another study from Nigeria reported medical waste generation ranged from 0.116 to 0.561 kg/bed/day in seven hospitals, with an average generation of approximately 0.181 kg/bed/day.[5] Our hospital was producing an average BMW of 0.179 kg/bed/day in 2005, which has increased four times in 2019 to reach 0.709 kg/bed/day. This continued increase reflects advances in the delivery of health care provided by our hospital over the years, and being a public hospital, its bed strength has always been fully occupied.
As of July 2018, there were 1,478 bedded and 3,916 nonbedded health care facilities in Delhi, which produced 24,667.05 kg of BMW every day. However, there are only two common biomedical waste treatment facilities (CBWTFs) to cater to these health care facilities.[6] The way BMW is growing as seen in our hospital, the number of CBWTFs is grossly inadequate to handle the current quantum of waste, and this capital city of Delhi would need to address this issue on the immediate priority of strengthening the number of these facilities.
The infectious plastic waste generated by our hospital from 2005 to 2019 has increased by 874.34%, with a CAGR of 16.4%. In comparison to incinerable waste, the quantity of plastic waste has significantly increased over these years. The CAGR for plastic waste has been 16.4%, which is almost double the CAGR for incinerable waste (8.4%). The plastic waste has also increased at a greater rate of 4% annually as compared with the total BMW and constituted 31% of the total BMW in 2005, but the figure reached to 53% in 2019.
Single-use items such as disposable syringes, needles, catheters, and body fluid collection bags, have become an integral part of the health care delivery and play a significant role in the control of hospital-associated infections. But over the years, single-use variations of some medical devices have been made available, replacing the previous models that were sterilized and reused repeatedly. This replacement of reusable materials with single-use disposables has resulted in a logarithmic expansion in the generation of plastic waste as is evident by the increase in quantities of plastic waste in our hospital.
The majority of plastic waste produced by health care facilities, if properly segregated, is likely to be recycled as per the Biomedical Waste Management Rules 2016. Only blood bags and waste contaminated by cytotoxic drugs is supposed to be incinerated. Improper management of plastic waste may result in adverse health and environmental effects. Combustion of plastics, especially chlorinated ones, may cause a generation of various hazardous substances such as smoke, carbon monoxide, dioxins, furans, and free radicals such as benzene. Some of these substances have negative effects on human and animal health, mainly affecting the endocrine and reproductive systems. Some of these are also well-known carcinogens. Plastic is estimated to be persisting in the environment for hundreds of thousands of years, but it is likely to be far longer in deep sea and nonsurface polar environments. Plastic debris poses a considerable threat by choking and starving wildlife.[7-9]
This creates a sad juxtaposition, in which we are contributing to the negative health effects created by the manufacture and disposal of plastics while delivering care to our patients.
With the advancement in sterilization techniques, we should consider giving a serious thought about reverting back to the use of instruments that can be easily sterilized and reused or exploring the possibilities of biodegradable/compostable plastics in health care.[7,9,10] As the demand for plastic in health care continues to grow, it is highly imperative that manufacturers of medical supplies are encouraged to produce and supply products that have minimal impact on the environment. In addition, medical scientists need to explore the possibilities of treatment modalities that result in reduced generation of plastic and other BMW.
Conclusion
This analysis of BMW data over a period of 15 years provides baseline information for policy development at individual hospitals as well as the national level. Generation of BMW is likely to see significant upward trends unless diligent deliberations are held between different stakeholders in regard to the reintroduction of reusable materials and waste reduction strategies. Health care waste management would require strengthening of capacity in areas of manpower and infrastructure development. It would also require intersectoral cooperation and coordination between different organizations.
Conflicting Interest
None declared.
Funding
None.
References
- Safe Management of Wastes from Health-Care Activities. (2nd). Geneva, Switzerland: WHO Blue Book; 2014.
- [Google Scholar]
- ASSOCHAM Bulletin. Available at: https://www.assocham.org/userfiles/Assocham%20Bulletin%20March%202019.pdf. Accessed July 27, 2020
- [Google Scholar]
- Health-care waste fact sheet. Available at: https://www.who.int/news-room/fact-sheets/detail/health-care-waste. Accessed July 27, 2020
- [Google Scholar]
- Bio-medical waste management in a tertiary care hospital: an overview. J Clin Diagn Res. 2016;10(11):DC01-DC03.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of medical waste management in seven hospitals in Lagos, Nigeria. BMC Public Health. 2016;16:269.
- [CrossRef] [PubMed] [Google Scholar]
- Annual Report on Biomedical Waste Management as per Biomedical Waste Management Rules, 2016 for the Year 2017. Available at: https://cpcb.nic.in/uploads/Projects/Bio-Medical-Waste/AR_BMWM_2017.pdf. Accessed July 27, 2020
- [Google Scholar]
- Toxic pollutants from plastic waste- a review. Procedia Environ Sci. 2016;35:701-708.
- [CrossRef] [Google Scholar]
- Accumulation and fragmentation of plastic debris in global environments. Philos Trans R Soc Lond B Biol Sci. 2009;364(1526):1985-1998.
- [CrossRef] [PubMed] [Google Scholar]
- Plastics and environmental health: the road ahead. Rev Environ Health. 2013;28(01):1-8.
- [CrossRef] [PubMed] [Google Scholar]
- New disinfection and sterilization methods. Emerg Infect Dis. 2001;7(02):348-353.
- [CrossRef] [PubMed] [Google Scholar]



