
Translate this page into:
Thyroid Tuberculosis in a Child: A Rare Entity
Address for correspondence: Dr. Anita Bodh, E-mail: anitabodh@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Thyroid tuberculosis is a rare disease even in countries where tuberculosis is endemic. Clinically tuberculosis is not often suspected in cases of thyroid nodule or swelling. We report a case of 11 years female child who presented with a thyroid swelling. Fine-needle aspiration cytology revealed caseating epithelioid granulomas and acid fast bacilli. Patient improved with antitubercular drugs. Tuberculosis may be considered as differential diagnosis of thyroid swelling.
Keywords
Acid fast bacilli
thyroid
tuberculosis

INTRODUCTION
Thyroid gland is rarely affected by tuberculosis, even in countries where tuberculosis is common.[1] World over about 200 cases of thyroid tuberculosis were reported in the literature.[23] Children constitute very small proportion of these cases and according to Terzidis et al.[3] and Razmpa et al.[4] only four children with thyroid tuberculosis had been reported in the past. Tuberculosis is seldom considered in the differential diagnosis of thyroid nodule or swelling.[5] We present a case of 11-year-old female child of thyroid tuberculosis who presented with a solitary thyroid nodule for 2 months and was diagnosed on cytological examination.
CASE REPORT
The present case is about an 11 years female child presented with a history of swelling in the thyroid region for preceding 2 months. On physical examination, thyroid gland was enlarged measuring 4.0 × 2.5 cm, firm in consistency and moving with deglutition. No palpable cervical lymphadenopathy was found.
On investigation, computed tomography (CT) scan neck showed large bilateral lobes of thyroid right measuring 21 × 13 mm and left 16 × 18 mm showing heterogeneous tissue density with evidence of necrosis, bilateral cervical lymphadenopathy. X-ray chest revealed non-homogenous opacity in the lower zone of lung on the right side. Enlargement of hilar and mediastinal lymph nodes, right side minimal pleural effusion and pleural thickening were found on CT scan of the thoracic cavity. Ultrasound of the abdomen revealed enlarged lymph nodes in periportal, portal, peripancreatic para-aortic regions. Hemoglobin was 10% g and erythrocyte sedimentation rate was 40 mm in 1st h. Peripheral smear of blood revealed microcytic hypochromic anemia. T3, T4 and thyroid stimulating hormone were within the normal limits and anti-thyroid peroxidase antibody was negative. Test for human immunodeficiency virus antibodies was negative. On fine-needle aspiration from the thyroid swelling, thick cheesy fluid was aspirated. The fluid was centrifuged and smears of the sediment showed caseating necrosis, few epithelioid cell granulomas and occasional benign follicular epithelial cells [Figures 1 and 2]. On Ziehl-Neelsen staining, smears showed acid fast bacilli (AFB). Tubercle bacilli were also detected by immunoflorescence microscopy using fluorescent Auramine-O stain. Based on caseating necrosis, epithelioid cell granulomas and demonstration of AFB, diagnosis of thyroid tuberculosis was made. With treatment with antitubercular drugs, thyroid swelling, lymphadenopathy, regressed gradually.
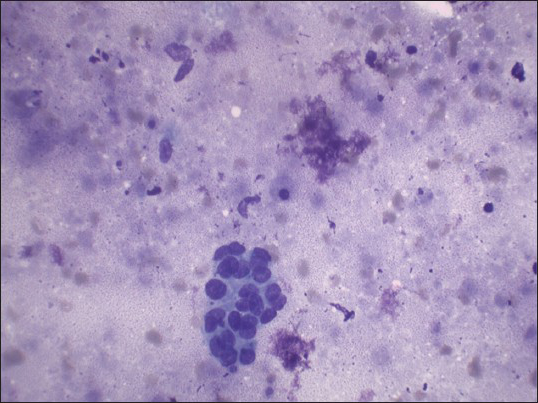
- Benign follicular cells and background of caseating necrosis (Giemsa stain, ×400)
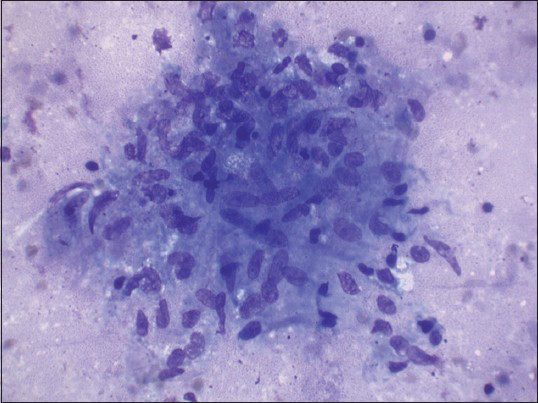
- Epithelioid cell granuloma with caseating necrotic background (Giemsa stain, ×400)
DISCUSSION
Thyroid tuberculosis is a rare entity. The estimation of prevalence of this condition is difficult.[4] However, reported prevalence rate varied from 0.1% to 1%.[6] Rarity of tuberculosis in thyroid has been attributed to bactericidal property of colloid, high vascularity and excess of iodine, enhanced activity of phagocytes in hyperthyroidism and possible antitubercular roles of thyroid hormone.[57]
Involvement of thyroid by tuberculosis can occur by hemetogenous and lymphatic routes or by direct extension from cervical lymphadenitis.[68]
Earlier the criteria described for diagnosis of thyroid tuberculosis were finding of AFB within thyroid, a necrotic or abscessed gland and presence of tuberculous focus outside the thyroid. Since it is not always possible to demonstrate AFB, recently it is stated that multiple coalesced and caseating epithelioid cell granulomas along with giant cells are considered to be diagnostic of thyroid tuberculosis.[56]
In our case, the diagnosis of tuberculosis of thyroid was confirmed by demonstration of tubercular bacili in the specimen. Other extra thyroid lesions were also found in the present case which is similar to findings noted in many previous reports.[4578910] Although pathological assessment of these extra thyroid tissues was not done in the present case to avoid invasive investigations, however, regression of these lesions with anti-tubercular drugs lends evidence to the possible tuberculous etiology in these lesions as well. One of the peculiarities of our case is that involvement of large number abdominal lymph nodes (periportal, portal, peripancreatic para-aortic regions) besides cervical, mediastinal lymph nodes and pulmonary lesion. To the best of our knowledge, no case of thyroid tuberculosis was reported in the past wherein such widespread extra thyroid involvement was observed. Usually the tubercular involvement of lymph nodes in such patients was limited to one or two lymph node regions with or without pulmonary tuberculosis. Khan et al.[5] in their study have reported four cases of thyroid tuberculosis, among them one case had cervical and axillary lymphadenopathy, another case had tuberculosis of cervical lymph nodes and third one had pulmonary tuberculosis and remaining one case did not reveal any involvement of extra thyroid tissue. Likewise in the case reported by Oklah and Al-Kaisi[10] concomitant pulmonary tuberculosis and tubercular mediastinal lymphadenitis was found and Mondal and Patra[9] in a study of 18 cases of thyroid tuberculosis found three cases had associated tubercular cervical lymphadenitis and four cases had pulmonary tuberculosis. Other atypicality is the younger age of our case, only very few cases were reported in this age group in the past, the most of previously reported patients were adults with the median age around 40s and.[139]
There are case reports that suggest the possibility of primary thyroid tuberculosis in which there is no known focus of tuberculosis outside thyroid and such condition is even more uncommon.[211] Like in current case, thyroid function test is generally found to be normal in these patients, but cases of thyrotoxicosis and hypothyroidism have also been reported.[578912]
The diagnosis of tuberculosis of the thyroid gland is rarely made clinically. Being a rare entity, tuberculosis as the cause of thyroid swelling is unlikely to be suspected clinically. Many of previous reported cases were found on examination of surgical or autopsy specimens.[27] However, like in the present case, fine-needle aspiration has also been found to be diagnostic in cases of thyroid tuberculosis thus preventing the unnecessary surgery.[17]
Differential diagnosis of granulomatous inflammation in thyroid includes subacute thyroiditis, goitrous autoimmune thyroiditis, tuberculosis and sarcoidosis.[6] However, caseating necrosis is the distinguishing feature that is diagnostic of tuberculous inflammation.[56]
It may be concluded that in cases of thyroid swellings tubercular thyroiditis should be considered as one of the differential diagnosis.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- Tuberculosis of the thyroid gland: Review of the literature. World J Surg. 2006;30:149-55.
- [Google Scholar]
- Primary tuberculosis of thyroid gland: A rare case report. Am J Otolaryngol. 2007;28:267-70.
- [Google Scholar]
- Clinical and paraclinical aspects of thyroid tuberculosis. Acta Med Iran. 2007;45:389-94.
- [Google Scholar]
- Tuberculosis of the thyroid gland: A clinicopathological profile of four cases and review of the literature. Aust N Z J Surg. 1993;63:807-10.
- [Google Scholar]
- Efficacy of fine needle aspiration cytology in the diagnosis of tuberculosis of the thyroid gland: A study of 18 cases. J Laryngol Otol. 1995;109:36-8.
- [Google Scholar]
- Tuberculosis of the thyroid presenting as multinodular goiter with hypothyroidism: A rare presentation. Indian J Pathol Microbiol. 2010;53:579-81.
- [Google Scholar]



