
Translate this page into:
Unusual Presentation of Multibacillary Nodular Leprosy
Address for correspondence: Dr. Gita Nataraj, E-mail: gitanataraj@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Despite India achieving the goal of elimination of leprosy as a public health problem, leprosy is still being transmitted in India. However, due to decreased clinical suspicion of leprosy and atypical case presentations, such cases may be not be diagnosed. We present a case report of an unusual presentation of multibacillary leprosy which presented as nodular lesions. This case report indicates that atypical presentations of leprosy may be missed out by primary care physicians.
Keywords
Granulomatous inflammation
multibacillary leprosy
nodular leprosy

INTRODUCTION
While India has achieved the goal of elimination of leprosy as a public health problem, defined as <1 case per 10,000 population, at the national level in December 2005,[1] leprosy still persists in certain high endemic districts. A total of 125,785 new cases were detected during the year 2014–15, which gives Annual New Case Detection Rate of 9.73 per 100,000 population.[2] A total of 88,833 cases are recorded as on April 1, 2015, giving a prevalence rate of 0.69 per 10,000 population.[2] Due to the decreasing prevalence of leprosy, the clinical suspicion for diagnosing the same has reduced. Atypical presentations may therefore be missed out. We report an unusual presentation of multibacillary leprosy which was diagnosed on slit skin smear examination from the lesion.
CASE REPORT
A 21-year-old man, working as a priest, presented with a history of generalized raised nodular lesions for 2 years. The patient was apparently asymptomatic 2 years back when he started developing reddish raised small lesions over the right knee. The lesions gradually increased in size and then ruptured with blood-stained purulent discharge. There was no loss of sensation. Lesions were not accompanied by pain, itching, or burning sensation. Similar lesions gradually developed over other sites such as left knee, both elbows, and ears. Other symptoms, such as joint pain, swelling of joints, or fever, were absent. The patient consulted a local doctor who advised a biopsy of the lesions. This biopsy report was suggestive of fungal infection; hence, the patient was treated with itraconazole and amoxicillin-clavulanic acid but without any relief. No acid-fast Bacilli (AFB) staining was done.
In our hospital
On clinical examination, multiple erythematous nodules and plaques of varying sizes ranging from 3 mm to 3 cm in diameter were seen on bilateral ear pinna and bony prominences of the extremities, i.e., elbows, knees, malleoli, and dorsal aspect of bilateral feet [Figure 1]. Some lesions were covered with hemorrhagic crusts. The lesions were nontender and firm to hard in consistency. The patient had neither oozing of fluid, discharge, sinus, nor ulcers. No history of contact with leprosy patients could be elicited.

- Nodular lesions on the right leg
Laboratory investigations
The blood parameters were within normal limits. Slit skin smears and biopsy from multiple lesions were collected and processed for bacterial and fungal culture since a provisional diagnosis of subcutaneous mycoses was considered. Microscopy as well as culture for both was negative. Slit skin smear received for detection of Mycobacterium leprae was stained by modified Ziehl–Neelsen (ZN) staining using 5% sulfuric acid. Examination of stained smear revealed characteristic AFB in large numbers [Figure 2]. A bacterial index of 4+ (10 AFB per oil immersion field) was recorded.[3] Histopathological examination of skin biopsy showed an unremarkable epidermis with underlying dermis showing a diffuse polymorphous inflammatory infiltrate coexisting with foamy histiocytes, neutrophils, plasma cells, and lymphocytes, extending from dermis to subcutis [Figure 3]. AFB were highlighted by Fite–Faraco stain [Figure 4]. Standard nerve stimulation test was done which showed evidence of mild axonal sensory mononeuritis multiplex in bilateral upper limbs and axonal sensory polyneuropathy affecting bilateral lower limbs with bilateral greater auricular, ulnar, common peroneal nerves showing thickening. This finding supported the microbiological diagnosis of leprosy.
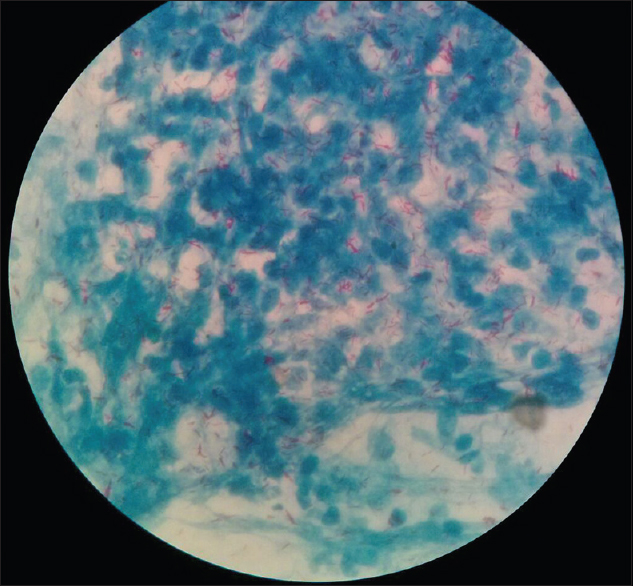
- Acid-fast Bacilli in large numbers, grouped together in cigar-bundle appearance. Stained with modified Ziehl–Neelsen staining, ×100
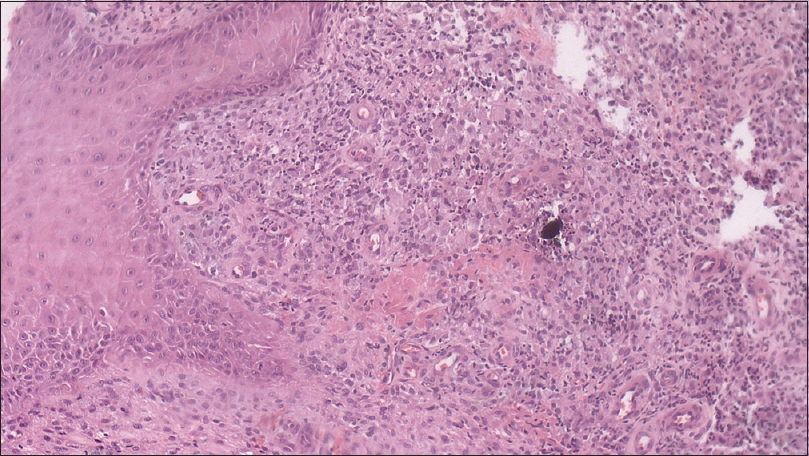
- Dermis showing diffuse polymorphous inflammatory infiltrate with foamy histiocytes, neutrophils, plasma cells, and lymphocytes; stained with H and E, ×100
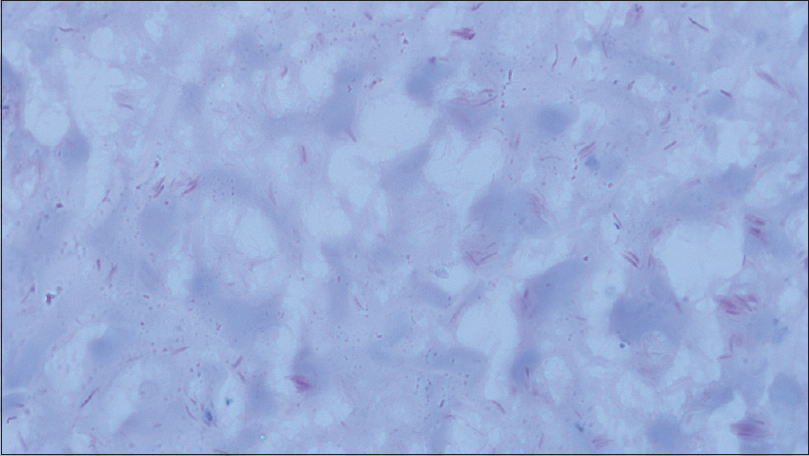
- Fite-Faraco stain demonstrating acid-fast Bacilli, ×100
Based on ZN stain results and histopathological report, the patient was considered as a case of lepromatous leprosy and started on multidrug therapy (MDT). Two months after commencement of MDT, the patient showed improvement with reduction of the nodular lesions.
DISCUSSION
Recent reports from India indicate that leprosy continues to be transmitted within the community despite advances in multidrug therapy. Continued findings of childhood leprosy cases ranging from 9.6% (2015)[4] to 11.43% (2009)[5] corroborate this theory as persistently high childhood proportion signifies ongoing transmission in general population.[6]
Leprosy presents as a wide spectrum of clinical manifestations, varying from polar tuberculoid to polar lepromatous disease.[5] Variable clinical presentations of leprosy, depending on an increasing bacterial load and loss of M. leprae-specific cellular immunity,[78] make it difficult to arrive at an accurate diagnosis, thereby emphasizing the need for appropriate investigations in every suspect case.
Mild symptoms in early stages of leprosy may be overlooked by the patient leading to a delay in seeking medical attention. Lack of clinical suspicion and appropriate investigation on the part of the health care professional may lead to a missed diagnosis and further delay in instituting appropriate therapy.[7] Given that the patient exhibited nodular lesions and lack of sensory loss, he was misdiagnosed as a case of subcutaneous fungal infection at the primary point of therapy. He was treated with antifungals and antibiotics which did not cure the lesions. The specimen obtained from the patient did not show any fungal element on microscopy and culture and there was no response to empiric antifungal therapy which helped to rule out fungal etiology. Leprosy should therefore be considered as a differential diagnosis for atypically presenting skin lesions not improving on empiric treatment.
With histopathological examination, leprosy presents as granulomatous inflammation that may mimic other granulomatous diseases including tuberculosis, sarcoidosis, leishmaniasis, and subcutaneous fungal infections.[910] Special stains such as Fite–Faraco stain have an added advantage in demonstrating M. leprae in histopathogical examination but may show negative results in tuberculoid leprosy cases where the lesions are paucibacillary in nature.[910]
This is a rare case of lepromatous leprosy presenting as nodular lesions without obvious sensory loss. In the current scenario, when the disease is considered as eliminated in India and patients coming with typical signs have become a rarity, a high index of clinical suspicion is necessary so as to not miss out on cases with atypical presentation. It is difficult to perform a histopathological examination in each case. However, slit skin smear from selective sites, which is a relatively minor procedure, should always be done in suspected leprosy cases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We are grateful to Dr. Sumeet Gujral, Consultant Hematologist, and Dr. Angad Singh, Tata Memorial Hospital, Mumbai, for providing the histopathological images of the specimen.
REFERENCES
- National Leprosy Eradication Programme. Available from: http://www.nlep.nic.in/about.html
- World Health Organization Leprosy Elimination, Microbiology of M. leprae, the Bacteriological Index (BI). Available from: http://www.who.int/lep/microbiology/en/
- Leprosy scenario at a tertiary level Hospital in Delhi: A 5-year retrospective study. Indian J Dermatol. 2015;60:55-9.
- [Google Scholar]
- Leprosy in post-elimination era in India: Difficult journey ahead. Indian J Dermatol. 2013;58:443-6.
- [Google Scholar]
- Single lesion multibacillary leprosy, a treatment enigma: A case report. J Med Case Rep. 2009;3:8.
- [Google Scholar]
- Granulomatous infections: Etiology and classification. Clin Infect Dis. 1996;23:146-58.
- [Google Scholar]
- A histopathological study of granulomatous inflammation. Nitte Univ J Health Sc. 2012;2:15-9.
- [Google Scholar]



