
Translate this page into:
Utility of horizontal and vertical sections of scalp biopsies in various forms of primary alopecias
Address for correspondence: Dr. Seetu Palo, Department of Pathology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Rae Bareli Road, Lucknow - 226 014, Uttar Pradesh, India. E-mail: seetu.pearl@gmail.com
-
Received: ,
Accepted: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
BACKGROUND:
This study was performed to demonstrate the usefulness of horizontal and vertical sections of scalp biopsies in diagnosing various forms of primary alopecias and to highlight the importance of error-free grossing.
MATERIALS AND METHODS:
A retrospective analytical review of 228 scalp biopsies was done, noting down the diagnostic histopathological features evident in horizontal and vertical sections of each cases. The idealness of the sections, especially horizontal section, was also analyzed.
RESULTS:
Out of the 228 cases, 44 scalp biopsies were classified histologically as cicatricial alopecias and the remaining 162 as noncicatricial alopecia. 22 cases were inconclusive owing to erroneous grossing. We found horizontal sections to be more useful in cases of noncicatricial alopecias, whereas vertical sections proved superior in cicatricial alopecias.
CONCLUSION:
Combining both horizontally and vertically sectioned scalp biopsies maximizes the diagnostic yield. When a single biopsy is submitted, the choice between horizontal and vertical section should depend on clinical diagnosis/suspicion.
Keywords
Cicatricial alopecia
horizontal section
noncicatricial alopecia
vertical section

Introduction
The microscopic evaluation of scalp biopsies forms an integral tool for the diagnosis of both cicatricial and noncicatricial alopecias.[1] However, rendering a histological diagnosis may, sometimes, prove daunting, especially if the grossing technique is improper. Substantial debate exists regarding the optimal sectioning technique of scalp biopsies. Both horizontal and vertical sections have their own potential advantages and disadvantages. However, when a single biopsy is received, the pathologist has to decide whether to section the specimen vertically or horizontally. Lack of clinical details further adds to the dilemma.
Aims
In an effort to reconcile the conflicting views regarding horizontal versus vertical sectioning, this study was undertaken to illustrate the utility of vertically and horizontally sectioned scalp biopsies in various forms of primary alopecias and to analyze which is superior. We also intend to highlight the importance of precise grossing of scalp biopsies.
Materials and Methods
A retrospective analytical study of scalp biopsies obtained from 228 patients attending Dermatology outpatient clinic attached to Bangalore medical college and research institute with the complaint of hair loss, from July 2011 to June 2014 was conducted. Two 4-mm punch biopsies, from appropriate sites, were obtained in each case for diagnostic purposes. These biopsies were received in 10% buffered formalin and were routinely processed. Grossing was carried out just before embedding. One of the biopsies was vertically sectioned, whereas the other biopsy was horizontally sectioned, approximately 1–1.5 mm below the epidermal surface. The grossed tissues were then embedded in paraffin with their cut surface down. About 3–4 μ thick microtomed sections were stained with hematoxylin and eosin (H and E). Both cicatricial and noncicatricial alopecias cases were included in the study. Cases, where only a single punch biopsy was received, were excluded.
All the H and E slides available, including the serial sections, were retrieved from the archives and jointly reviewed by two pathologists, along with the accompanying pathology request forms. Demographic data, clinical details, and provisional clinical diagnoses were also collected. The diagnostic histomorphologic features that were evident in horizontal and vertical sections of each case were noted down in detail. The utility of each section was analyzed qualitatively. The idealness of the sections, especially the horizontal sections, was also critically assessed.
Results/Observation
Out of the 228 biopsies analyzed, cases of noncicatricial alopecia (n = 162) outnumbered the cases of cicatricial alopecia (n = 44). Among the nonscarring ones, alopecia areata (AA) topped the list. Table 1 depicts the distribution profile of the cases. In Table 2, we have mentioned the utility of vertical and horizontal sections in arriving at a histological diagnosis as experienced by us during the study. We also assessed the idealness of the horizontal sections in each case. Of the 228 cases, 156 cases (68.4%) had ideally cut horizontal sections displaying the pilosebaceous units [Figure 8a]. 28 cases (12.3%) were dissected at the level of subcutis, and the remaining 44 cases (19.3%) were obliquely sectioned [Figure 8b and c]. We could not arrive at a final diagnosis in 22 (9.6%) cases owing to grossing errors.


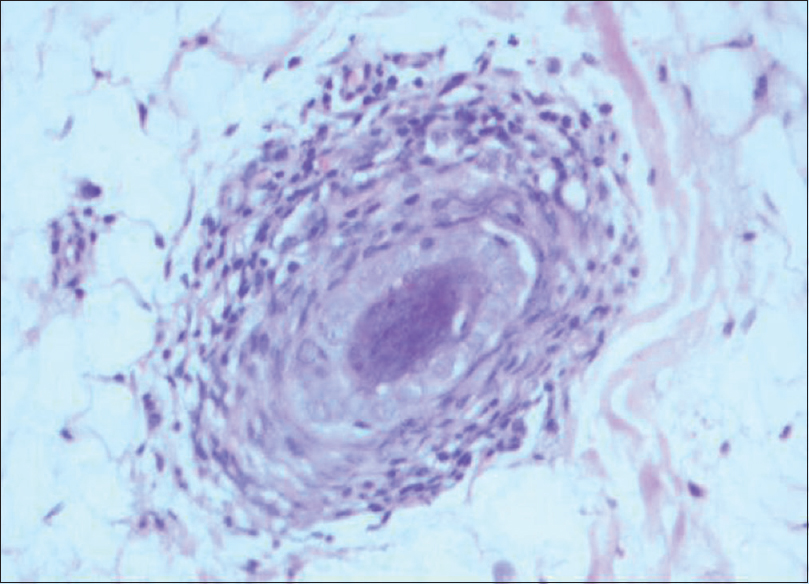
- Perifollicular fibrosis seen on vertical section in a case of alopecia areata (H and E, ×400)
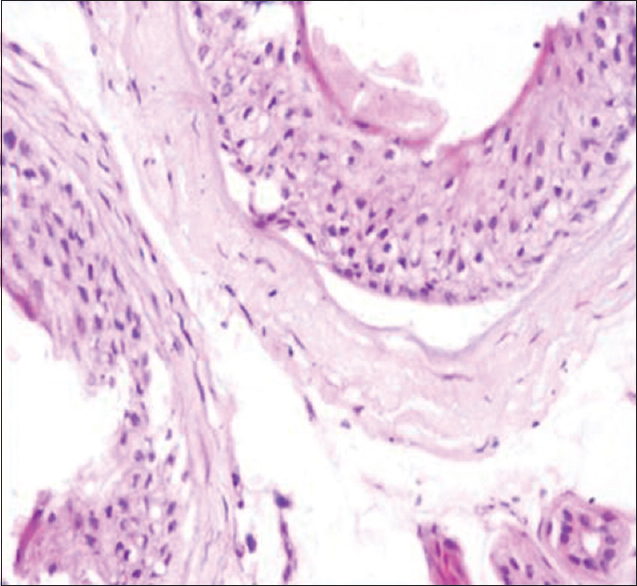
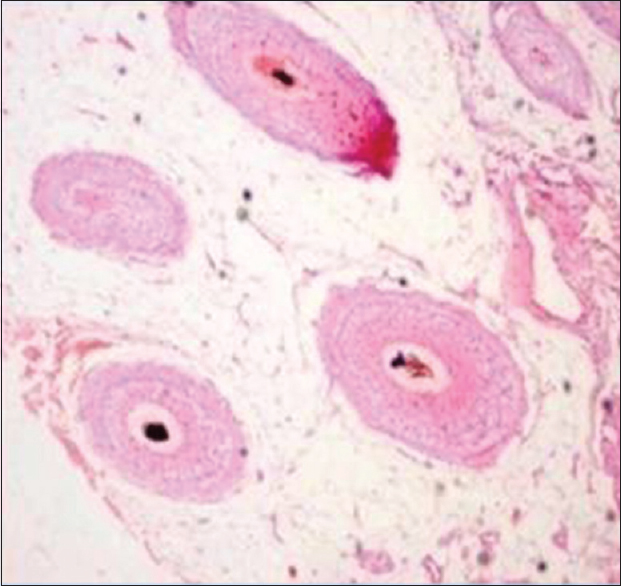
- Perifollicular mononuclear cell infiltrate seen on horizontal section in a case of alopecia areata (H and E, ×400)
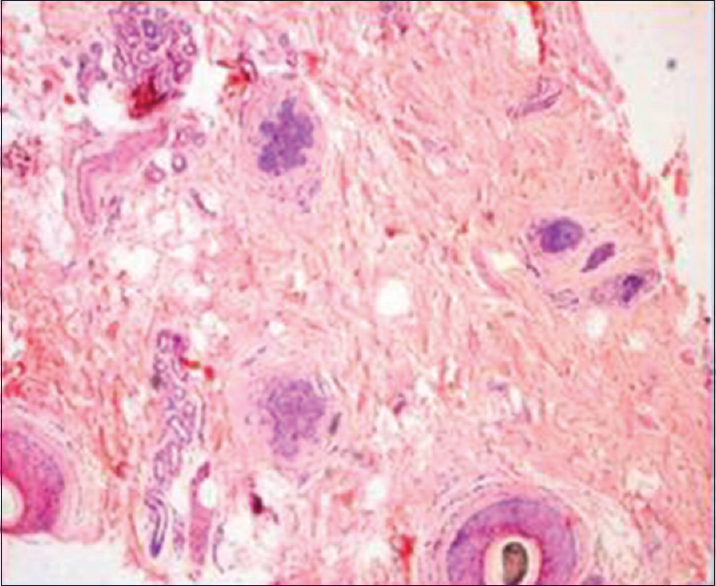
- Horizontal section showing increased number of telogen in a case of telogen effluvium (H and E, ×100)
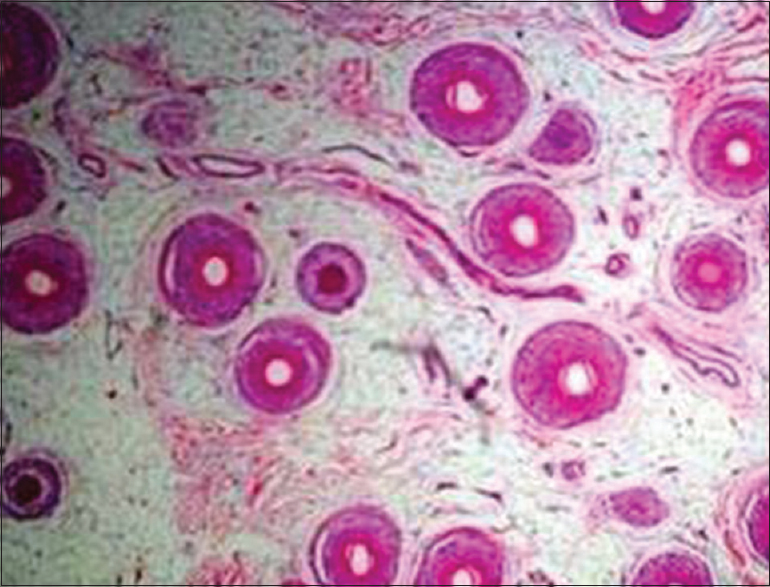
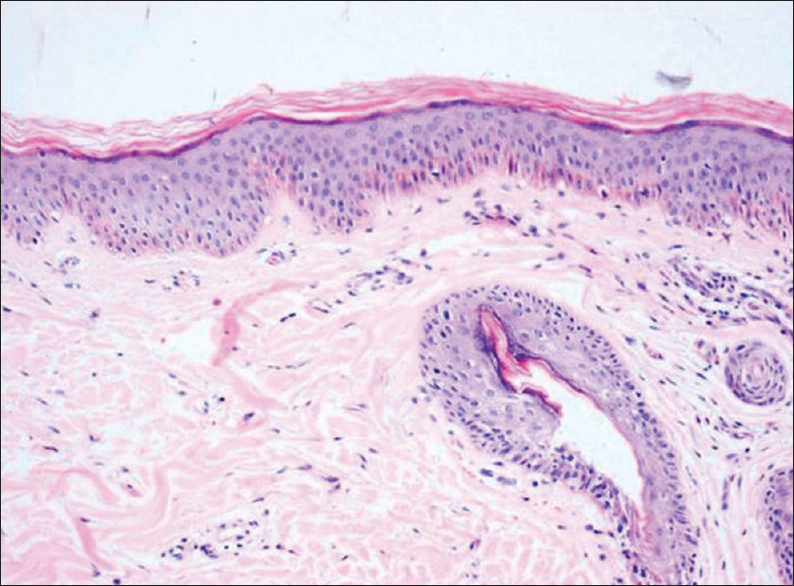
- Miniaturized hair follicles seen on horizontal section in a case of androgenetic alopecia (H and E, ×100)
- Melanin pigment cast noted on horizontal section in a case of trichotillomania (H and E, ×100)
- Dysmorphic hair follicle noted on horizontal section in a case of Trichotillomania (H and E, ×100)
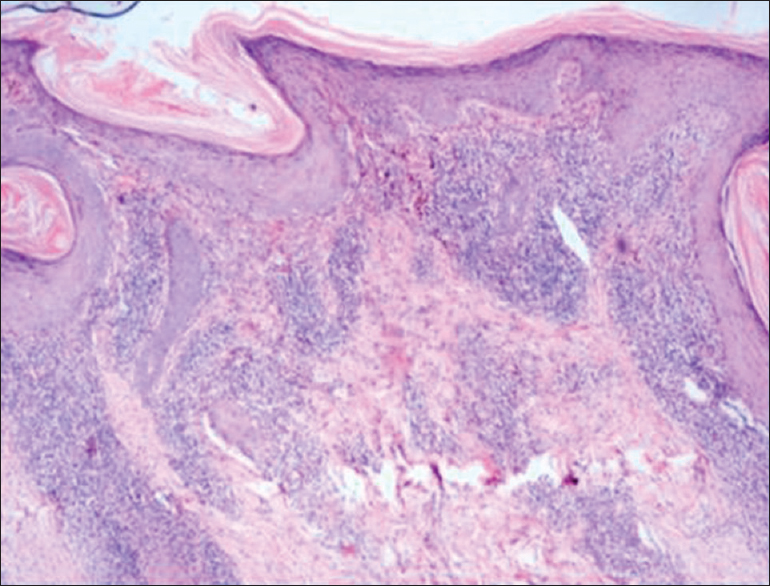
- Characteristic features of discoid lupus erythematosus noted on vertical section (H and E, ×100)
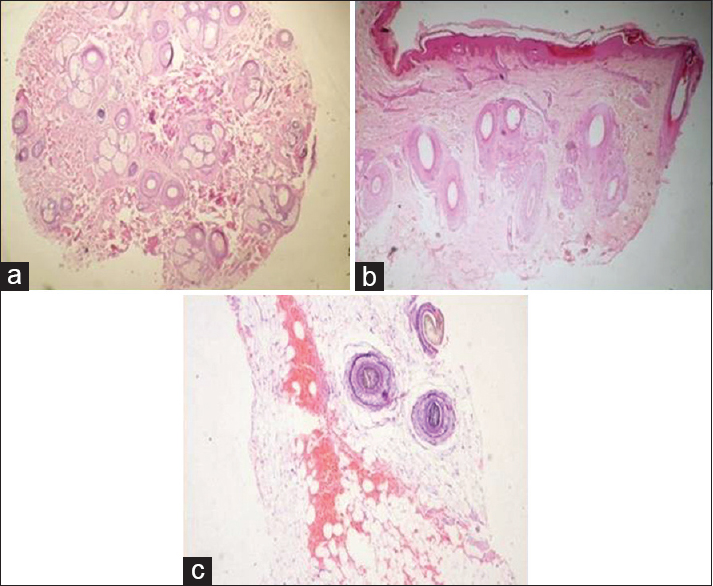
- (a) An ideal horizontal section displaying the pilosebaceous units (H and E, ×40). (b) An obliquely cut scalp biopsy (H and E, ×40). (c) A scalp biopsy sectioned at the level of subcutis (H and E, ×100)
Discussion
Several studies have been conducted to address the problem of horizontal versus vertical sectioning of scalp biopsies, and it is a well-known fact that both the techniques have their inherent pros and cons. Du et al.[2] meta-analyzed the published literature in this context and found that no significant difference exists between horizontal and vertical sectioning techniques in the diagnosis of alopecia and suggested future well-designed studies in this area. Elston et al.,[3] Sinclair et al.,[4] and Stefanato[5] concluded that combining both horizontal and vertical sections maximizes the diagnostic yield when compared to either section alone. Our findings also ascertain the same, that is, if two biopsies are available, the best way of processing is to section one of the biopsies horizontally and the other vertically.
A 2001 consensus meeting[6] acknowledged the merits of combined horizontal and vertical sections in various forms of alopecia and added that horizontal sectioning is to be preferred if a single biopsy is received. We suggest, whenever a single scalp biopsy is submitted, the decision should be based on the clinical diagnosis. We found horizontal sections to be more useful in cases of noncicatricial alopecias, whereas vertical sections conferred a diagnostic advantage in cicatricial alopecias. This is in concordance with the study by Elston et al.[7] Özcan et al.[8] opined that it is preferable to have horizontal sections in cases of noncicatricial alopecia, vertical sections in cases of suspected lichen planopilarsis (LPP) and either type of sections in cicatricial alopecia when LPP is clinically ruled-out.
We observed that the vertically sectioned scalp biopsies provide the benefit of viewing full thickness of skin and complete hair profile, from root to top. Interface changes can be well made out. Subcutaneous pathology, if any, is not missed. The degree of peribulbar inflammation and fibrosis can be better assessed. Grossing is much easier as compared to horizontal sections. The major drawback of vertical sections is that the follicular counts and ratio cannot be assessed. Furthermore, vertical sections show only 10%–20% of the total number of follicles and the probability of sampling error is quite high. Serial sectioning may be required to find the ‘diagnostic follicle’ which adds to the laboratory expenses and increases the turnover time. Bathish et al.[9] found that serial vertical sectioning of scalp biopsies increases the diagnostic yield substantially, in noncicatricial as well as cicatricial alopecias. Tandon et al.[10] studied 27 cases of LPP and found vertical sections to provide sufficient histological clues.
The potential utility of horizontal sections lies in deducing follicular counts, density and ratio. It allows visualization of all the hair follicles present in the biopsy core. Follicular growth dynamics and hair morphometry can be studied. Hence, we found horizontal sections to be crucial for diagnosis in cases of Telogen effluvium and androgenetic alopecia where follicular ratios are important. In cases of Discoid lupus erythematosus and LPP, we failed to assess the dermoepidermal junction on horizontal sections; and hence, it was of minimal diagnostic utility in these cases. Another disadvantage of horizontal sections is that the grossing is cumbersome and demands some degree of expertise and experience.
We studied 97 cases of AA and noted horizontal and vertical sections to be complementary to each other. If a single biopsy is submitted, then we prefer horizontal sectioning of the specimen. Singh et al.[11] could diagnose 100% cases of AA by horizontal sections alone and 93.3% cases by vertical sections alone. They found horizontal sections to be superior as it provided a better assessment of the histological features of AA. Jameel et al.[12] also found horizontally sectioned scalp biopsies to be beneficial in diagnosing AA as well as predicting the disease stage.
In the present study, we assessed the idealness of the horizontal sections in all the cases. Out of 228 cases, 72 (31.6%) cases were inappropriately grossed, that is, either obliquely sectioned (44 cases) or cut at the level of subcutis (28 cases). Serial sectioning had to be done in these 28 erroneously grossed cases to reach the pilosebaceous apparatus for microscopic evaluation, whereas the 44 obliquely sectioned ones had to be reoriented, reblocked, and then resectioned. These factors led to tissue loss, increased the turnover time and decreased the cost-effectiveness. A conclusive diagnosis was not possible in 22 (9.6%) cases due to improper grossing. Hence, we lay emphasis on efficient grossing techniques of the scalp biopsies, especially the horizontal ones.
Headington[13] demonstrated that “the best area to bisect a punch biopsy for the horizontal section is 1 mm above the dermal-subcutaneous junction.” In our practice, we find it difficult to pinpoint the dermal-subcutaneous junction in a processed specimen. It is equally difficult to make a clean cut at the aforementioned area in an unprocessed biopsy sample. Frishberg et al.[14] advocated the idea of slicing the biopsy specimen into 3 or 4 horizontal sections, and embedding all the slices with cut surface down in the same cassette. We feel that this technique demands proper embedding and recuts will lead to critical tissue loss. Another interesting technique, “the Tyler technique,” involves first vertically sectioning the entire specimen into two halves, followed by horizontal sectioning of one of the halves.[15] The demerit of this method is that it limits the evaluation of hair density and ratio as only half of the actual biopsy is studied microscopically. In the “St. John's Protocol,” two 4-mm punch biopsies of the scalp are procured. In suspected cases of cicatricial alopecias, one biopsy is bisected horizontally and the other vertically whereas in cases of noncicatricial alopecias, both the biopsies are transected horizontally 1 mm below the epidermis.[3] After employing this very protocol, Tailor et al.[16] observed a significant increase in the diagnostic yield of scalp biopsies.
In our institution, we usually receive two scalp biopsies. One of the biopsies is bisected vertically, making sure that the cut is made parallel to the direction of hair growth. The other biopsy is cut horizontally, following the technique proposed by Solomon.[17] We dissect the scalp biopsies 1–1.5 mm below the epidermal surface after overnight processing, just before the embedding step. We find this procedure quite feasible, easy, and rewarding. Needless to say, special attention must be given to the final microtomy step to avoid tangential cuts and obtain a perfect horizontal section.
Recently, the new “Hovert technique”[18] is gaining popularity, wherein the scalp biopsy is transected approximately 1 mm below the epidermal surface to obtain an “epidermal disc.” This epidermal disc is subjected to vertical sectioning in conventional fashion, whereas the remaining lower portion of the biopsy is sliced for horizontal sections. Kolivras and Thompson[19] employed the Hovert technique and found the procedure to improve and simplify the diagnostics. However, more studies need to be conducted to affirm the efficiency and reproducibility of this newer method.
Conclusion
We found that the combination of two punch biopsies (one horizontally and other vertically sectioned) is ideal for microscopic diagnosis in cases of alopecia. Whenever a single biopsy is submitted, grossing technique should be dictated by the clinical diagnosis. Vertical sectioning is to be preferred in noncicatricial alopecias and horizontal sectioning to be preferred in noncicatricial alopecias. Furthermore, utmost care should be taken to make grossing error-free to avoid serial sectioning and/or inconclusive diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The scalp biopsy for hair loss and its interpretation. Semin Cutan Med Surg. 2015;34:57-66.
- [Google Scholar]
- Diagnostic value of horizontal versus vertical sections for scarring and non-scarring alopecia: A systematic review and meta-analysis. Eur J Dermatol. 2016;26:361-9.
- [Google Scholar]
- Vertical and transverse sections of alopecia biopsy specimens: Combining the two to maximize diagnostic yield. J Am Acad Dermatol. 1995;32:454-7.
- [Google Scholar]
- The reliability of horizontally sectioned scalp biopsies in the diagnosis of chronic diffuse telogen hair loss in women. J Am Acad Dermatol. 2004;51:189-99.
- [Google Scholar]
- Histopathology of alopecia: A clinicopathological approach to diagnosis. Histopathology. 2010;56:24-38.
- [Google Scholar]
- Summary of North American Hair Research Society (NAHRS)-sponsored workshop on cicatricial alopecia, Duke University Medical Center, February 10 and 11, 2001. J Am Acad Dermatol. 2003;48:103-10.
- [Google Scholar]
- A comparison of vertical versus transverse sections in the evaluation of alopecia biopsy specimens. J Am Acad Dermatol. 2005;53:267-72.
- [Google Scholar]
- Vertical vs. Transverse sections of scalp biopsy specimens: A pilot study on the comparison of the diagnostic value of two techniques in alopecia. Clin Exp Dermatol. 2011;36:855-63.
- [Google Scholar]
- A study of serial vertical sectioning of scalp biopsies to increase the histological diagnostic yield in alopecias. J Eur Acad Dermatol Venereol. 2010;24:709-15.
- [Google Scholar]
- A histologic review of 27 patients with lichen planopilaris. J Am Acad Dermatol. 2008;59:91-8.
- [Google Scholar]
- A comparison of vertical and transverse sections in the histological diagnosis of alopecia areata scalp biopsy specimens. Int J Trichology. 2016;8:111-5.
- [Google Scholar]
- Value of transverse section scalp biopsy in alopecia areata - A clinicopathological correlation. J Coll Physicians Surg Pak. 2008;18:338-41.
- [Google Scholar]
- Transverse microscopic anatomy of the human scalp. A basis for a morphometric approach to disorders of the hair follicle. Arch Dermatol. 1984;120:449-56.
- [Google Scholar]
- Transverse scalp sections: A proposed method for laboratory processing. J Am Acad Dermatol. 1996;35:220-2.
- [Google Scholar]
- The current state of play in the histopathologic assessment of alopecia: Two for one or one for two? J Cutan Pathol. 2013;40:298-304.
- [Google Scholar]
- The transversely sectioned scalp biopsy specimen: The technique and an algorithm for its use in the diagnosis of alopecia. Adv Dermatol. 1994;9:127-57.
- [Google Scholar]
- The HoVert technique: A novel method for the sectioning of alopecia biopsies. J Cutan Pathol. 2011;38:401-6.
- [Google Scholar]
- Primary scalp alopecia: New histopathological tools, new concepts and a practical guide to diagnosis. J Cutan Pathol. 2017;44:53-69.
- [Google Scholar]



