
Translate this page into:
Xp11.2 Translocation Renal Cell Carcinoma Diagnosed by Immunohistochemistry and Cytogenetics
Address for correspondence: Dr. Biswajit Dey, E-mail: drbish25@rediffmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Xp11.2 translocation renal cell carcinomas (TRCCs) are a group of neoplasms with distinct clinical, histopathological appearance, immunohistochemical, and cytogenetic profile. We report a case of Xp11.2 translocation TRCC in an 11-year-old male diagnosed based on immunohistochemistry and fluorescence in situ hybridization.
Keywords
Immunohistochemistry
renal cell carcinoma
translocation

INTRODUCTION
Xp11.2 translocation renal cell carcinoma (TRCC), characterized by translocation of the transcription factor E3 (TFE3) gene located on the locus Xp11.2, is a rare subtype of TRCC. It was recognized as a separate entity in 2004 World Health Organization classification of kidney tumors.[1] Primarily described in children and adolescents, TRCCs have been reported in the adult population, with a poor prognosis.[2] Xp11.2 TRCCs are a group of neoplasms with distinct clinical, histopathological appearance, immunohistochemical, and cytogenetic profile. We report a case of Xp11.2 TRCC in an 11-year-old male diagnosed based on morphology, immunohistochemistry (IHC) and confirmed by cytogenetics.
CASE REPORT
An 11-year-old male presented with five to six episodes of hematuria and intermittent abdominal pain of 10 days duration. The patient had congenital hearing deafness and was on hearing aids. There were no other significant medical or surgical illnesses in the past. There was no history of previous exposure to any cytotoxic chemotherapy. Computed tomography of his abdomen revealed a 4 cm × 4 cm × 3 cm mass involving predominantly the upper pole of the right kidney [Figure 1a]. A metastatic workup revealed no evidence of lung, liver, or nodal metastasis. A clinical diagnosis of Wilms’ tumor was made and a right nephroureterectomy was done.

- (a) Contrast-enhanced computed tomography abdomen showed a 4 cm × 4 cm × 3 cm mass involving the upper pole of the right kidney. (b) Grossly, the upper pole of the kidney revealed a mass, which was tan yellow and necrotic with cystic areas. (c) Microscopically, tumor cells were arranged in papillary configuration (H and E, ×40). (d). On high power, the tumor cells had voluminous, clear to eosinophilic cytoplasm, vesicular nuclear chromatin and prominent nucleoli (H and E, ×400)
On gross examination, the upper pole of the kidney revealed a 4 cm × 4 cm × 3 cm mass, which on cut section was tan yellow and necrotic with cystic areas [Figure 1b]. Microscopically, the tumor cells were arranged in papillary configuration [Figure 1c]. The tumor cells had voluminous, clear to eosinophilic cytoplasm, vesicular nuclear chromatin, and prominent nucleoli [Figure 1d]. The nuclear grade corresponded to Fuhrman Grade 2. However, psammomatous calcifications were not seen. On IHC, these tumor cells were focally positive for CD10, vimentin, and epithelial membrane antigen (EMA) but were negative for CK7 and Melan-A [Figure 2a–d]. These features were suggestive of Xp11.2 TRCC. IHC for TFE3 showed nuclear positivity in the tumor cells [Figure 3a]. A fluorescence in situ hybridization (FISH) testing was performed for TFE3 translocation. FISH analysis showed positive TFE3 translocation in 90% of the tumor cells, thus confirming the diagnosis of Xp11.2 TRCC [Figure 3b].
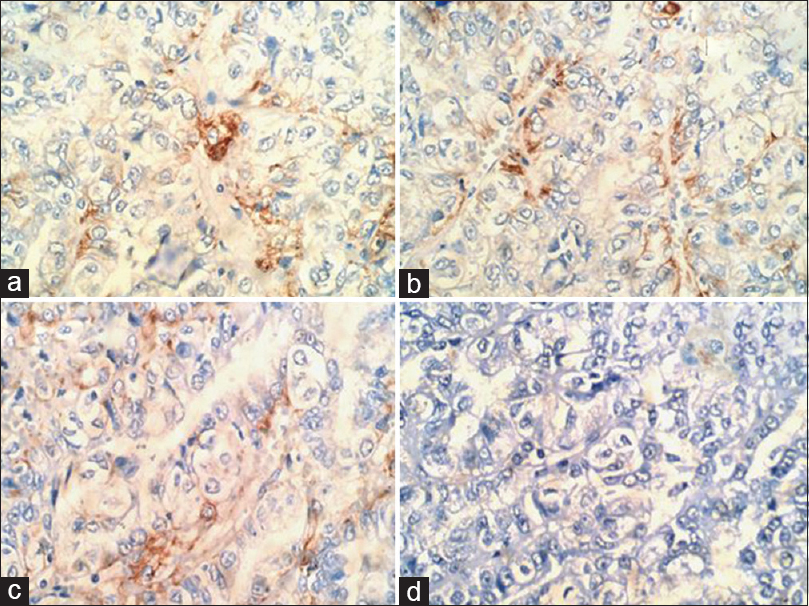
- (a-c) Tumor cells showing positivity for CD10, epithelial membrane antigen, and vimentin, respectively (IHC, ×400). (d). Tumors cells showing negativity for CK7 (IHC, ×400)

- (a) Tumor cells showing strong nuclear positivity for transcription factor E3 (IHC, ×400). (b) Fluorescence in situ hybridization showing positive transcription factor E3 translocation in the tumor cells
At 17-months postoperative follow-up, the patient is doing well without any locoregional recurrence.
DISCUSSION
Recently recognized as a separate entity in 2004, TRCC is a rare neoplasm with distinct clinical and pathological characteristics.[12] Xp11.2 TRCCs occur primarily, but not exclusively, in children and young adults with a strong female predominance.[2] One-third of pediatric renal carcinomas are related to TFE3 translocation accounting for 20–40% of pediatric TRCC.[2] The incidence of Xp11.2 TRCCs has been reported to be 1–1.6% of all renal tumors in adults.[3] Its actual incidence remains underestimated in India, and only a few case reports are available from India.[456] Clinically, Xp11.2 TRCCs usually present as an asymptomatic, painless mass, often identified incidentally during abdominal imaging.[2] Cytotoxic chemotherapy is the only known predisposing factor to the development of Xp11.2 TRCC.[7]
Grossly, Xp11.2 TRCCs usually have variegated appearance and may mimic conventional clear cell RCC and papillary RCC. A multilocular cystic gross appearance is uncommon.[7] Microscopically, Xp11.2 TRCCs show papillary or nested architecture in a background of prominent capillary vasculature.[278] The neoplastic cells are voluminous and polygonal, with clear and eosinophilic granular cytoplasm. The nuclei are vesicular with prominent nucleoli.[278] Psammomatous calcifications and foci of stromal eosinophilic hyaline globules may be numerous. Satellite tumor nodules, necrosis, and lymphovascular invasion are frequently observed.[8]
IHC typically reveals positivity for CD10 and weak or rare reactivity to cytokeratins (CK7, AE1/AE3), EMA, and melanocytic markers such as Melan-A. Vimentin is variably expressed.[278] However, the most sensitive and specific immunohistochemical markers for these neoplasms are TFE3 protein and cathepsin K.[28] FISH assay and real-time polymerase chain reaction are useful confirmatory tests for TFE3 gene rearrangement.[4]
In Xp11.2 TRCCs, because of the genetic rearrangements with one of the five known partner genes described (ASPL on 17q25, PRCC on 1q21, PSF on 1q34, NonO on Xq12, and CLTC on 17q23), there is overexpression of the fusion product. The fusion product is found to contain C-terminal portion of TFE3, which is a member of the microphthalmia-associated transcriptional factor family.[89]
Clinical outcome data are still inconclusive. Children with isolated lymph node metastasis are found to have a favorable short-term prognosis whereas adults often have widespread metastasis at the time of presentation connotes a poor outcome. Regardless of the age, a long-term follow-up is recommended as the tumor can metastasize decades after its initial presentation.[7]
The current management of Xp11.2 TRCC is similar to conventional RCC. For localized Xp11.2 TRCC including patients with positive regional lymph nodes, surgery is the treatment of choice. For patients with hematogenous metastases, the current options are VEGFR-targeted therapies and mammalian target of rapamycin inhibitors.[48]
Our case demonstrates the importance of performing IHC as the distinction of Xp11.2 TRCC is crucial in determining surveillance protocol and management. Cytogenetic analyses for TFE3 gene rearrangement should be done besides the IHC for confirmation of the diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Renal carcinomas associated with Xp11.2 translocations/TFE3 gene fusions. In: Eble JN, Sauter G, Epstein JI, Sesterhenn IA, eds. Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs (World Health Organization Classification of Tumours). Lyon, France: IARC; 2004. p. :37-8.
- [Google Scholar]
- Xp 11.2 translocation renal carcinoma in young adults; recently classified distinct subtype. Radiol Oncol. 2014;48:197-202.
- [Google Scholar]
- Renal cell carcinoma associated with Xp11.2 translocation/TFE3 gene fusion: A rare case report with review of the literature. Case Rep Urol 2013 2013:810590.
- [Google Scholar]
- Xp11 translocation renal cell carcinoma morphologically mimicking clear cell-papillary renal cell carcinoma in an adult patient: Report of a case expanding the morphologic spectrum of Xp11 translocation renal cell carcinomas. Int J Surg Pathol. 2015;23:234-7.
- [Google Scholar]
- Renal cell carcinoma associated with Xp11.2 translocation/transcription factor E3 (TFE3) fusion. J Cytol Histol. 2013;4:173.
- [Google Scholar]
- Review of renal carcinoma associated with Xp11.2 translocations/TFE3 gene fusions with focus on pathobiological aspect. Histol Histopathol. 2012;27:133-40.
- [Google Scholar]



